Hidradenitis suppurativa: what’s new in pathogenesis and management

Hidradenitis suppurativa is a chronic autoinflammatory skin condition with significant comorbidities. Advances in our understanding of its pathogenesis are leading to new potential treatments.
- Hidradenitis suppurativa (HS) is an autoinflammatory skin condition involving the innate immune system.
- The pathogenesis of HS is not fully understood; inflammation has been regarded as secondary to follicular occlusion but is now considered the likely initial event.
- Genetics, the skin and gut microbiome and biofilms are also likely to play significant roles in HS pathogenesis.
- HS is part of the follicular occlusion tetrad, and evidence is emerging that the other members (acne conglobata, dissecting cellulitis of the scalp and pilonidal sinus) are anatomical variants of HS.
- Biologics such as interleukin-23 and interleukin-1 are emerging off-label treatments for patients with HS, although large-scale randomised clinical trials are lacking.
Hidradenitis suppurativa (HS) is a chronic, autoinflammatory skin condition characterised by the development of inflammatory nodules and abscesses in intertriginous, hair-bearing areas.1 It is associated with several comorbidities, including metabolic syndrome, polycystic ovary syndrome, inflammatory bowel disease (IBD) and depression.2-6 The prevalence of HS is 1 to 4%, and it affects three times as many women as men.1 HS is associated with a reduced quality of life, psychosocial impact and physical pain.7 There is often a significant delay between disease onset and diagnosis, and this may be due to lack of recognition of the disease in its early stages in addition to poor awareness of HS among medical practitioners and the general public.
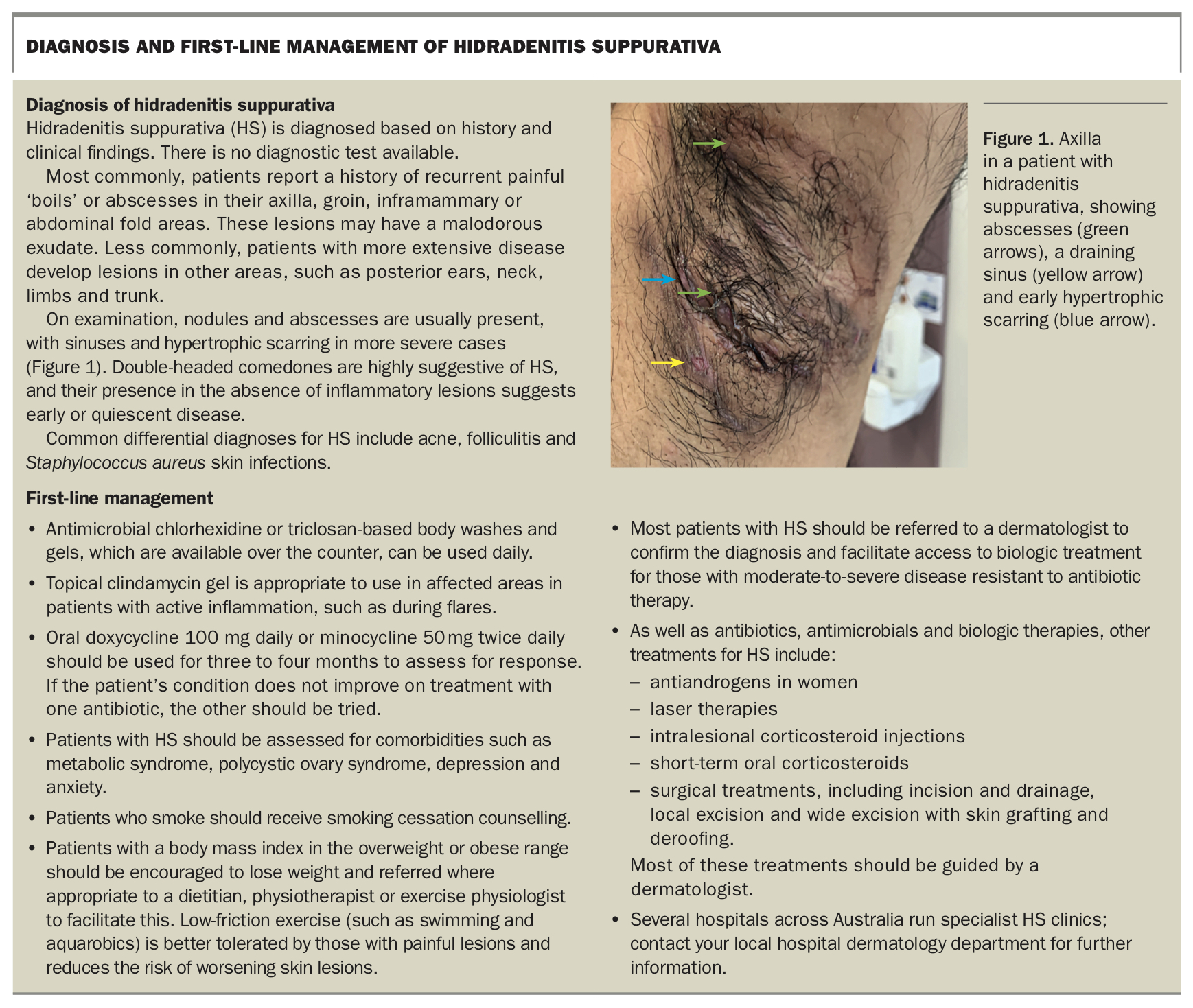
Over the past few years, our understanding of the pathogenesis of HS has evolved. This review focuses on evolving and emerging concepts of HS pathogenesis and its implications for management with biologic treatments. Diagnosis and first-line management of HS are summarised in the Box.
{kind=link}
Evolving models of pathogenesis of HS
The pathogenesis of HS is not fully understood. Classically, it has been considered an inflammatory skin disease triggered by occlusion of hair follicles, with secondary inflammation. New evidence suggest that HS should be considered a disease with multifactorial causes including genetic factors, the skin and gut microbiome, skin biofilms and dysregulation of the innate immune system.
Genetic factors
About one-third of patients with HS have a family history of the disease.8 Several genetic variants have been identified in the genes encoding the gamma-secretase enzyme complex, which regulates the function of the Notch cell membrane protein. Notch is responsible for normal skin function in humans and animals, and disruption of gamma-secretase function in mice has been shown to result in the formation of epidermal cysts and epidermal hyperplasia reminiscent of HS in humans.9 However, most patients with HS do not have mutations in the gamma-secretase complex genes, suggesting that pathogenesis is multifactorial.10 Additionally, Notch disruption in mice via knockout is associated with disrupted barrier function, epidermal differentiation and alopecia, which are not seen in humans with HS.11 Caution is needed in interpreting results from animal models of HS.
The skin microbiome and biofilms
HS has previously been viewed as an infective disease. However, it is now recognised as an autoinflammatory condition with a significant burden of comorbidities associated with systemic inflammation. Although the role of bacteria in disease pathogenesis requires further elucidation, the inflammatory process is thought to be driven by cutaneous microbiome dysbiosis.12 A study showed that perilesional skin in affected individuals has greater microbial diversity than lesional skin.13 The axillary microbiome has also been shown to be altered, with reduced diversity, in prelesional skin in affected individuals versus healthy controls.14
Biofilms, composed of bacteria and the extracellular matrix that they produce, have been identified in both chronic HS lesions and perilesional skin and are often associated with treatment resistance.15 The development of a biofilm may partly explain the chronicity and treatment resistance of lesions, as well as disease recurrence after surgical excision. Additionally, biofilms may be implicated in disease progression over time. It is known from chronic wound studies that biofilms cause host immune alterations and induce the release of proinflammatory cytokines.15
The cutaneous microbiome is a growing area of scientific interest in a number of skin diseases, and establishing what constitutes the ‘normal’ microbiota is a crucial next step. Similarly, ongoing research is needed to identify the role of biofilms in HS pathogenesis, progression and treatment resistance.
Inflammatory pathways
Classically, HS has been considered a cutaneous disease characterised by follicular occlusion with a secondary inflammatory response. However, some evidence suggests that follicular occlusion is secondary to the underlying inflammatory process, thought to be driven by interleukin (IL)-1.12 Additionally, the interleukins IL-12, IL-17 and IL-23 and tumour necrosis factor-alfa (TNF-alfa) have all been identified in active HS lesions.16 Phase 3 studies are now underway to assess the efficacy and safety of anti-IL-17 and anti-IL-23 treatments in patients with HS.
The skin-gut-brain axis
The evolving skin-gut-brain axis model of skin disease may be applicable to HS. Neural and systemic inflammation secondary to gut dysbiosis may contribute to the association between HS and depression and anxiety via bidirectional signalling, rather than the link being exclusively a result of the experience of the physical symptoms and associated emotional impact of HS. Research in germ-free mice models has shown depressive-like behaviours after transplantation of faecal microbiota from patients with major depressive disorder versus microbiota from healthy controls.17
Alterations in the gut microbiome can increase gut permeability, resulting in local and systemic inflammation through bacterial translocation, as seen in patients with non-alcoholic fatty liver disease.18 Gastrointestinal microflora can also be associated with skin disease, as seen in the association between rosacea and Helicobacter pylori.19
The skin-gut axis may also explain the association between IBD and HS through alterations to gut microflora. IBD is associated with gut dysbiosis and impaired gut epithelial function.20 Further research is required to establish this relationship.
Emerging concepts in HS
Follicular occlusion tetrad
HS belongs to the follicular occlusion tetrad, which also includes acne conglobata, dissecting cellulitis of the scalp and pilonidal sinus. All four diseases in this tetrad share common histological and cytochemical findings, indicating that they are likely to represent anatomical variants of a single disease process.21,22 Further studies comparing histological, inflammatory mediator and clinical outcomes in these diseases are necessary to elucidate the true relationship.23 It is likely that the local skin microbiome is involved.
HS phenotypes
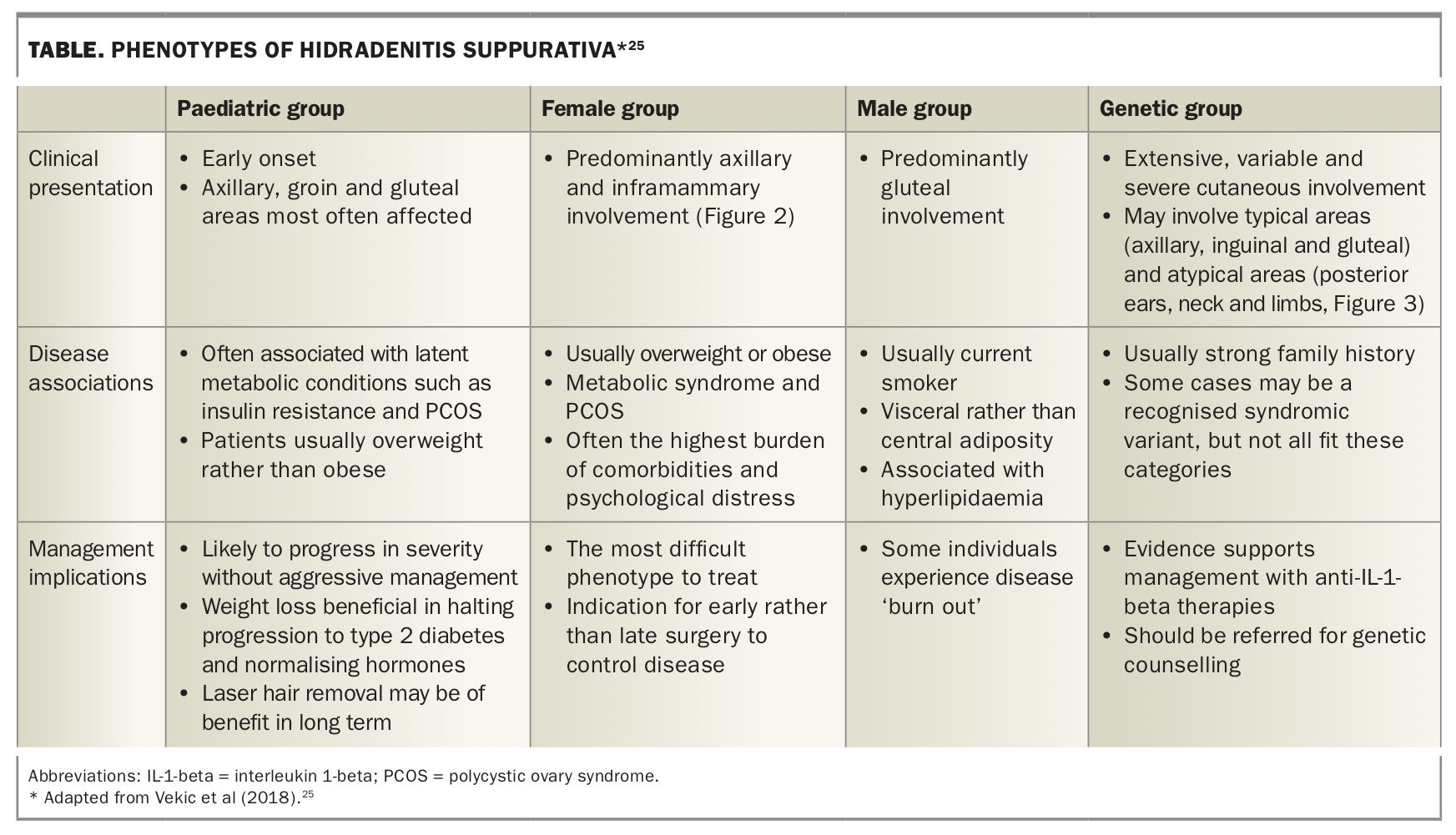
HS is not a homogeneous disease.10 There is preliminary work on differentiating HS phenotypes.24 A recent simple classification system into paediatric, female, male and genetic forms is based on age of onset, body site involvement and associated comorbidities (Table, Figure 2 and Figure 3).25 It is hoped that an improved definition of phenotypes will allow more targeted therapies and better understanding of prognosis.
{kind=link}
.jpg){kind=link}
.jpg){kind=link}
Precise correlation between HS phenotype and genotype is not currently possible. This probably reflects the multiple factors involved in HS pathogenesis.
Emerging treatments
Current systemic treatments for patients with HS include oral antibiotics and the TNF-alfa blocker adalimumab. Patients whose condition fails to respond adequately to these treatments currently have no alternative biologic treatment options available through the PBS in Australia. Recognition of the role of interleukins in HS has led to trials of interleukin inhibitors in the treatment of patients with HS. Some of these are available off-label and on compassionate grounds for patients with HS.
Ustekinumab, an IL-12 and IL-23 inhibitor, was shown in a small open-label study to be effective in treating patients with HS. In this study, 47% of patients achieved a 50% or greater reduction in inflammatory lesion count.26 Ustekinumab is not PBS listed for HS and is used off-label in Australia for these patients. Other IL-23 inhibitors such as tildrakizumab are used in Australia off-label via compassionate access. At present, several phase II trials of IL-23 inhibitors are underway.
Anakinra, an antagonist of IL-1 (a central proinflammatory cytokine), was shown in a small randomised controlled trial to be effective in patients with moderate to severe HS; 78% of participants achieved a 50% or greater reduction in inflammatory lesion count.27 Anakinra may be available via compassionate access for patients with treatment-resistant HS through dermatologists. It is not PBS listed for HS. Administration requires a daily injection, which some patients find painful.
Interleukin-17 has been identified in HS lesions, along with IL-1 and TNF-alfa.28 The efficacy and safety of anti-IL-17 biologic treatments in HS is under investigation, with phase III trials currently or soon to be underway. However, the association of HS with IBD is a concern. IL-17 is gut protective in mice models, with blocking of IL-17 associated with increased gut permeability.29 As discussed above, increased gut permeability is implicated in bacterial translocation and disease pathogenesis. Exacerbations of IBD have been observed in trials of IL-17 biologics in patients with psoriasis, and their use is therefore avoided in those who have psoriasis and concomitant IBD.30 Further human studies are required to assess whether IL-17 plays a similar role in gut homeostasis in humans as in mice.
Implications for practice
Patients with HS should be screened extensively for comorbidities, such as metabolic syndrome, depression and hyperandrogenism. Optimising treatment of these comorbidities is important to reduce HS disease severity and decrease systemic inflammation. Smoking cessation and weight loss should be strongly encouraged for the same reason. All patients with HS benefit from low-friction exercise such as swimming, as this improves concurrent metabolic syndrome and facilitates weight loss.
Additionally, patients with common comorbidities such as metabolic syndrome and polycystic ovary syndrome should be screened for HS. This will help identify patients with mild HS, in whom treatments are more efficacious, and aggressive early management is likely to lead to optimal long-term outcomes. Patients with these comorbidities should be asked about blackheads, abscesses, nodules and pustular lesions in their axillary, inguinal and gluteal regions, and should also be examined for the presence of these lesions.
At present, the only biologic treatment for moderate-to-severe HS that is available on the PBS is adalimumab, a TNF-alfa blocker. This is a nonspecific targeted therapy that is used in other inflammatory conditions such as IBD and rheumatoid arthritis.
All patients with known or suspected HS should be referred to a dermatologist for review and specialist management. This will enable patients to access adalimumab, in addition to off-label and clinical trial treatments when clinically indicated.
Conclusion
HS is a complex autoinflammatory disease associated with debilitating cutaneous manifestations and a high burden of comorbidities. Patients with HS should be extensively screened for associated comorbidities. Likewise, screening for HS should be part of standard care for patients with common comorbidities such as metabolic syndrome, to identify those with latent and early cases of HS.
Ongoing research examining pathways of disease pathogenesis in HS is required, particularly to identify the inciting causes of HS and determine why it progresses in severity. This will enable us to optimise patient outcomes through new treatments, and allow us to identify how best to prevent the disease and disease progression. MT