Recurrent urinary tract infections. Management in women
Recurrent lower urinary tract infection (UTI) is a common problem seen in general practice affecting more women than men. Fifty per cent of women will experience at least one UTI during their lifetime and 20% will have recurrent UTIs.
- Lower urinary tract infections (UTIs) are among the most common patient presentations to general practice.
- For various anatomical and physiological reasons, UTIs are more common in women, with 50% experiencing at least one UTI in their lifetime.
- Evidence of two or more UTIs in six months, or three or more UTIs in one year is defined as recurrent UTI (rUTI).
- Urine microscopy, culture and sensitivity is the gold standard diagnostic investigation for UTI and rUTI.
- Women with rUTI need further investigations to identify underlying causes.
- Antibiotics are at the core of UTI treatment, but for rUTIs they may be considered as a prophylactic option.
- Nonantiobiotic options include methenamine hippurate and topical oestrogens.
- General advice to women with rUTI is directed at lifestyle modification, personal hygiene, safe sex practice and sexual behaviour modification.
Lower urinary tract infections (UTIs) are among the most common patient presentations to general practice with symptoms of frequent urination, urgency, dysuria, suprapubic pain, turbid or offensive-smelling urine, haematuria, fever and nonspecific lower back pain.1 UTIs are more common in women, with about one in three with having at least one UTI requiring antibiotic treatment by 24 years of age and 50% experiencing at least one UTI in their lifetime.2,3
Evidence of two or more UTIs in six months or three or more UTIs in one year is defined as recurrent UTI (rUTI).4,5 In a US study of healthy, college-age women who were followed for six months after an index UTI, almost 30% had one or more symptomatic recurrence.6 In another study of 179 Finnish women who were followed for one year after an index Escherichia coli UTI, 44% had one or more further UTIs and 5% had more than three UTIs.7
Symptomatic UTI can be particularly distressing for patients, with lower urinary tract symptoms, general malaise and restrictions on everyday activities, days lost from work and even hospitalisation in the case of elderly patients.8
Why do women get rUTIs?
In most cases, no obvious cause can be found. However, any abnormality of the structure or function of the urinary tract can predispose women to rUTI and this should be considered. Possible risk factors contributing to rUTIs are shown in the Box and are usually detected by careful history taking.
{kind=link}
Women have a shorter urethra than men and their external urethral meatus is close to and at risk of bacterial contamination from the vaginal introitus and anal canal, increasing the risk of ascending UTIs.9-11 Physiological changes associated with pregnancy can predispose to asymptomatic bacteriuria and increase the risk of UTIs.9 Furthermore, menopause and oestrogen deficiency lead to vaginal atrophy, change in pH and vaginal flora. All these physiological changes can predispose women to UTI and rUTI.9,12
Diagnosis of rUTIs
Urine microscopy, culture and sensitivity is the gold standard diagnostic investigation to detect the presence of uropathogens and decide on the most appropriate antimicrobial therapy.13 UTI is defined as a positive urine culture of greater than 100,000 cfu/mL from a mid-stream urine sample. However, lower counts have been described in symptomatic patients with acute cystitis (e.g. greater than 1000 cfu/mL).14,15 Dipstick urine analysis is a useful screening test in general practice. It can improve the accuracy of clinical symptoms in confirming or ruling out acute UTI in women. A positive nitrite test is more useful than a positive leukocyte esterase (LE) test, although both increase the odds of a UTI diagnosis. If nitrite and LE tests are negative, the odds of a UTI decrease by 40 to 60%.16 A urine culture is recommended for all women presenting with rUTI, to detect any uropathogens and determine bacterial sensitivity.14
Types of recurrence
UTIs may recur as a result of reinfection and relapse. Relapses generally occur within the first two weeks of treatment, usually with the same uropathogen.17 This can happen due to lack of sensitivity to the prescribed antibiotic agent, poor patient adherence or concurrent conditions that would diminish efficacy of treatment (e.g. gastroenteritis, use of medications that would interact with the antibiotic agent prescribed). Reinfections happen more than two weeks after the initiation of the therapy, usually preceded by a negative urine culture, and may be caused by the same pathogen or a different one.14 Furthermore, UTIs can be classified as uncomplicated, when the urinary tract is anatomically and functionally normal with no underlying conditions that could cause deterioration in its function; or complicated, if there are underlying conditions such as vesicoureteral reflux or renal calculi.
Investigations
Women with rUTI need further investigations to identify any underlying causes. Correct choice of antibiotic, based on urine culture to detect the uropathogen and ascertain susceptibility, and patient adherence to antibiotic treatment are required. Urinary tract ultrasound is an inexpensive and cost-effective first-line test to assess obvious anomalies of the upper or lower urinary tract as well as pre- and postvoid bladder volume to assess bladder emptying and increased postvoid urine residue. The latter can be checked with a bladder scan if available or simply by using an ‘in and out’ catheter in the clinic.
Investigation by CT intravenous urography can further delineate the abnormal findings from an ultrasound. MRI can give more information about the perirenal soft tissue and urinary tract but is more expensive and may not be readily accessible.
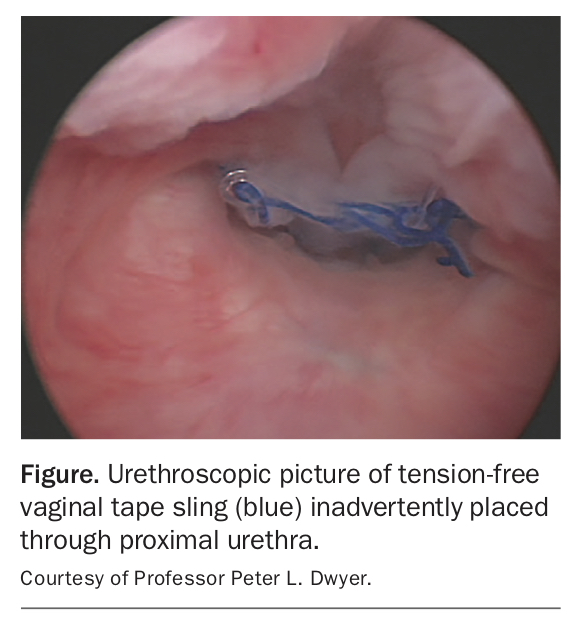
Cystourethroscopy may help assess the underlying causes of rUTI and is usually performed with flexible or rigid scopes using local anaesthetic lubricant. During the cystoscopy, the operator has direct vision of the lower urinary tract and can assess for any obvious abnormality such as cancer, strictures or calculi. The Figure shows a tension-free vaginal tape sling misplaced through the urethra in a woman who had stress incontinence and presented with voiding difficulty and rUTI postoperatively.
{kind=link}
Management of rUTIs
General therapies
General advice to women with rUTI is directed at lifestyle modification, personal hygiene, safe sex practice and sexual behaviour modification.
Increasing fluids has not been shown to be an effective prophylaxis; however, patients should be advised to keep well hydrated as one of the natural defensive mechanisms of the urinary system is to flush the pathogens. Counselling should focus on regular voiding and complete bladder emptying.
Personal hygiene, wearing loose cotton underwear, keeping the genital area dry and wiping the genitals from front to back to avoid contamination of the peri-urethral area with perianal flora may be recommended but have not been scientifically proven.
Sexual intercourse is one of the greatest risk factors for rUTIs. Avoiding intercourse with multiple partners not only reduces risk of rUTI but also of sexually transmitted infections. Avoiding spermicides, vaginal diaphragms and vaginal douching has shown to reduce the risk of rUTI.18,19
Antimicrobial therapy
Antibiotics are at the core of UTI treatment to eradicate the pathogens. However, for rUTIs they may be considered as a prophylactic option. Prescribing antibiotics to women with rUTI should take into account patient preferences, allergen profile, drug interactions, renal and liver function status, pregnancy, breastfeeding, previous UTIs and susceptibility, and local guidelines.
A Cochrane review has shown antibiotics to be superior to placebo in preventing rUTI in nonpregnant women with a number needed to treat of 1.85. However, there was no difference seen between antibiotics of different classes. The review concludes that continuous low-dosage antibiotic prophylaxis for six to 12 months reduced the rate of UTI during prophylaxis but not after prophylaxis; two studies showed no difference in recurrence of UTI between different antibiotics. There were more adverse events in the antibiotic group. One randomised controlled trial compared postcoital versus continuous daily ciprofloxacin and found no significant difference in rates of UTIs, suggesting that postcoital treatment could be offered to women who have UTI associated with sexual intercourse.4
Antibiotic prophylaxis regimens can be continuous or postcoital, and practitioner or patient initiated. Low-dosage regimens of antibiotics for rUTI prophylaxis are available in Australia and all are listed on the PBS (e.g. trimethoprim 150 mg at night, cefalexin 250 mg at night or nitrofurantoin 50 mg at night).20
Long-term use of nitrofurantoin has been associated with an increased risk of rare adverse effects, including pulmonary toxicity, hepatotoxicity and peripheral polyneuropathy. Monitor for these adverse effects with regular spirometry and liver and kidney function tests. Polyneuropathy is more likely to occur in patients with impaired kidney function.20
Postcoital prophylaxis involves administration of a single dose of antibiotic immediately after sexual intercourse. This method is associated with fewer side effects and reduced antibiotic use in women for whom coitus is the initiating factor.
A patient-initiated regimen is associated with less antibiotic use overall compared with continuous prophylaxis. However, patients should be instructed to seek advice if there is no resolution of symptoms within 48 hours. This method is more suitable for those who are self-motivated and have good medication adherence and comprehension of correct antibiotic use.21
Other nonantibiotic options
Oestrogen
Vaginal lactobacilli decrease and vaginal pH rises during menopause as a result of a lack of local and circulating oestrogen. This allows Gram-negative bacilli and potential uropathogens to multiply, increasing the risk of ascending urinary infection from the changed vaginal flora. Topical estrogen reverses this by increasing the proliferation of lactobacilli and lowering pH.
Topical estrogen products such as vaginal pessaries and creams are available in Australia and listed on the PBS. The application is usually twice a week.
A 2008 Cochrane review found no benefit from oral estrogen supplements compared with placebo in reducing rUTI, based on four studies with nearly 2700 participants. However, estrogen applied vaginally showed reduction in rUTI compared with placebo (based on two studies) but results were conflicting when compared with oral antibiotics (two studies). Potential side effects for vaginal estrogens include breast tenderness, vaginal bleeding, non-physiological discharge, vaginal irritation, burning and itching but are all uncommon.22
It is important to note that restoration of vaginal flora to lactobacilli takes almost 12 weeks using vaginal estrogen supplements.23
Methenamine hippurate
Methenamine hippurate has been used in Australia for many years as a prophylactic agent for prevention of rUTI. Methenamine hippurate is excreted by the kidneys into the bladder where it is broken down in acidic urine (pH less than 6) to formaldehyde and ammonia. It is often taken with once-daily vitamin C to enhance effectiveness. Formaldehyde has nonspecific bacteriostatic effects, which helps prevent rUTI. There has been no resistance reported to methenamine hippurate. It is sold as 1 g tablets and is listed on the PBS.
A 2012 Cochrane review found methenamine hippurate may be effective for preventing UTI in patients without renal tract abnormalities, particularly when used for short-term (one week or less) prophylaxis. Many clinicians and their patients have found methenamine hippurate useful in the longer term. However, more prospective comparative studies are needed to establish the long-term efficacy of methenamine hippurate. Methenamine hippurate has been reported to be ineffective in women with neuropathic bladder or who have renal tract abnormalities.24
Cranberry products
Cranberry products are available in the form of juice, syrup, tablets and capsules. They are sold as over-the-counter medications and not listed on the PBS. The likely mechanism by which cranberry works is by inhibiting the adherence of the uropathogens to urothelial cells which specifically applies to E. coli. This feature is facilitated by a substance called proanthocyanidin.25
A 2012 Cochrane review including 24 studies with more than 4400 participants showed that, compared with placebo, water or no treatment, cranberry products did not significantly reduce the occurrence of symptomatic UTI overall or in any of the subgroups including women with rUTI or pregnant women.26
Probiotics
Probiotics are beneficial microorganisms that have been used in women with rUTIs. They are widely available in stores as over-the-counter medication and not listed on the PBS. Some suggested mechanisms of action is by the blockage of bacterial attachment to epithelial lining, producing hydrogen peroxide (microbicidal), reducing pH, and inducing an anti-inflammatory cytokine response in epithelial cells; or simply increasing vaginal lactobacilli.27
A 2015 Cochrane review of nine studies and 735 participants found the studies to be of small size with poor methodology. No significant reduction was found in the risk of recurrent symptomatic bacterial UTI between patients treated with probiotics and placebo (six studies, unclear or high risk of bias) or between patients treated with probiotics and antibiotics (one study, unclear or high risk of bias).28
Immunoprophylaxis
This is an evolving field with no high-level evidence currently to support use of vaccines. However, some small early studies show promising outcomes. There is no vaccine available on the PBS for prevention of rUTI.29
When to refer?
GPs play an important role in the work-up and management of women with recurrent urinary tract infection. However, women should be referred for specialist review in complicated cases.
Patients with a pelvic mass, vaginal prolapse beyond the hymen, rectal prolapse, kidney stones, chronic catheterisation, immunosuppression, atypical symptoms (e.g. gross haematuria, pneumaturia following pelvic procedure, incomplete voiding following incontinence surgery), rapid progression to sepsis, presence of multidrug-resistant pathogens, or a history of complicated UTIs.30 Treatment of aggravating factors should always be considered if found. For instance, removal of the intraurethral sling in the Figure cured the patient of her rUTI.
UTI in pregnancy
Pregnancy induces changes in the urinary system such as urine stasis, smooth muscle relaxation, reduced peristalsis and pressure effect of gravid uterus on ureters, which predispose to urinary tract infections. Furthermore, differences in pH and osmolality as well as pregnancy-induced glycosuria and aminoaciduria may contribute to bacterial growth. Asymptomatic bacteriuria (ASB) occurs in 2 to 15% of pregnancies and, if not treated in pregnancy, up to 20 to 30% of these women will develop pyelonephritis.31-33
There is no clear definition of rUTI in pregnancy. A Cochrane review has included one or more UTIs in its review claiming one infection in pregnancy can be an indication for prophylactic antibiotics in practice and some research trials.34
Screening for ASB should be performed at 12 to 16 weeks of pregnancy with a quantitative urine culture. If confirmed, treat the infection as per local guidelines. Women should be routinely screened after treatment of ASB. Antibiotic prophylaxis should be prescribed for pregnant women with recurrent bacteriuria or bacteriuria and risk factors for pyelonephritis (e.g. immune compromise, diabetes, neurogenic bladder).35
Conclusion
Recurrent UTI is a common condition in women across all ages. It has significant socio-economic burden and can result in days lost from work.
Women need to be properly assessed with a thorough history and physical examination followed by a urine culture to ascertain the uropathogen and its susceptibility. A renal tract ultrasound and measurement of postvoid residue are readily available and accessible first-line investigations.
Acute UTI should be appropriately treated with antibiotic therapy, and prophylaxis may be by maintenance antibiotics or postcoital therapy. However, because of the risk of antibiotic resistance associated with long-term and recurrent use, many women seek alternative strategies. The evidence for the efficacy of these alternative therapies is conflicting but the search should go on.
Women who have complicated UTIs or any other underlying pathology and those with warning signs should be referred for specialist review and assessment. MT