A woman with worsening fatigue and menorrhagia

Fatigue is a common nonspecific symptom with a wide range of causes that are most often work and life stresses, but which may be underlying serious disorders. Assessing patients with fatigue should therefore feature careful evaluation of the costs and benefits of possible investigations.
Generalised lethargy or fatigue is a common presenting symptom in general practice, reported in 1 to 7% of general practice encounters. It can pose diagnostic challenges.1,2 Lethargy may be defined as extreme fatigue or drowsiness in the absence of increased physical activity, unrelieved by rest. Although the most common causes tend to be psychosocial or lifestyle related, serious abnormalities may underpin its presentation. The prevalence of underlying pathology ranges from less than 10% up to 50% of patients presenting with lethargy.2 This wide range may reflect a wide variation in study methods.2
Patients are sometimes referred to multiple specialists, including endocrinologists, and extensively investigated in an attempt to assuage patient concern and rule out serious pathophysiology (Box 1). It is therefore important that GPs develop a consistent and confident approach to managing such patients, as extensive blanket investigation can lead to false-positive results, generate unwarranted healthcare costs, exacerbate patient anxiety and expose patients to unnecessary risk.2,3 It is important to take a thorough history, perform a systematic physical examination and order appropriate targeted investigations to rule out significant reversible conditions. In the absence of identifiable pathology, diagnoses such as chronic fatigue syndrome, psychosocial stressors or lifestyle causes should be considered.4 Among 167 patients in Canada who presented with lethargy, psychosocial diagnoses were made in 24%, with depressive disorders and anxiety disorders diagnosed more often in women.5 Lifestyle causes include diet (particularly caffeine intake), shift work, sleep disruption, age and environmental stresses such as recent reports related to coronavirus disease 2019 (COVID-19).
{kind=link}
Chronic fatigue syndrome should be considered as a diagnosis of exclusion in patients presenting with persistent fatigue for over six months and associated severe impairment in occupational, educational, social and personal activities, in the absence of other identifiable conditions.6 Acute physical or psychological stress may precipitate chronic fatigue syndrome.6 An assessment of the patient’s psychosocial state and current stressors is important and management requires ongoing lifestyle advice and counselling with regular supportive follow up. Cognitive behavioural therapy (CBT) has been shown to benefit patients with chronic fatigue syndrome, with 40% of patients undergoing CBT showing a clinical response compared with 26% with usual care.7 A systematic review found similar benefits from exercise therapy compared with CBT for levels of fatigue, physical functioning and sleep; however, no evidence of improvement in chronic pain, anxiety, depression or quality of life was shown, and the optimal type and intensity of exercise remains unclear.8
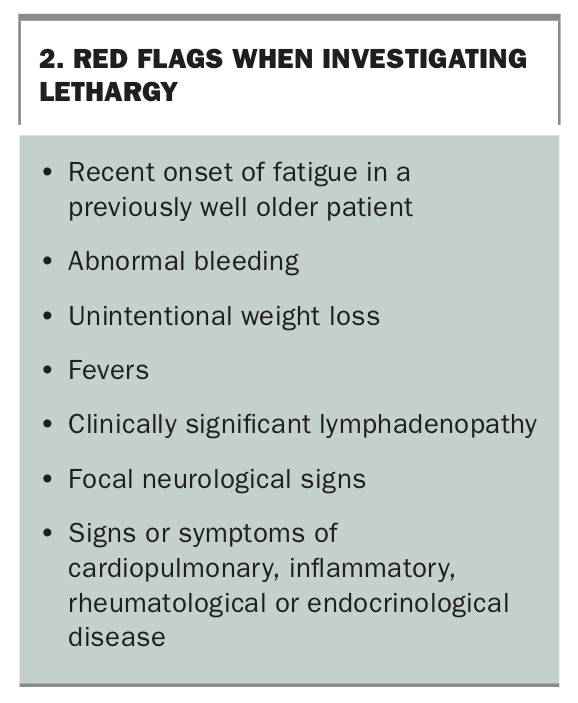
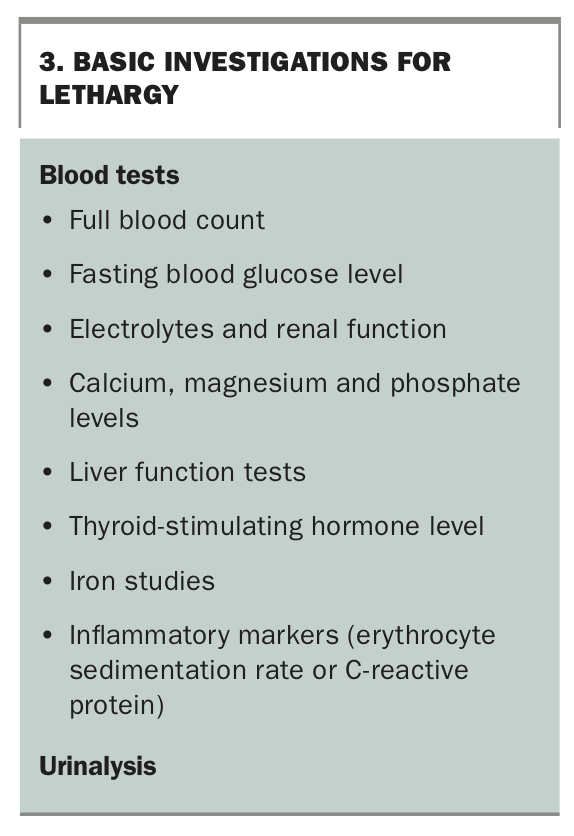
Guidelines on the approach to investigating and managing fatigue have been published but vary between countries.4,9 A diagnostic approach to fatigue outlined in the Australian Therapeutic Guidelines considers pretest probability based on patient demographics and potential associated red flags, weighing the costs and benefits of investigations.9 Red flags are shown in Box 2. In the absence of red flags, it is reasonable to monitor patients for a four-week period before initiating investigation.2,9 Screening questionnaires for depression and obstructive sleep apnoea, such as the K10 checklist and the Epworth Sleepiness Scale, can assess reversible factors. On examination, the patient’s weight, body habitus, body mass index (BMI) and mental state should be recorded. Any signs of anaemia, cardiopulmonary disease, focal neurological deficits, thyroid disease, organomegaly or lymphadenopathy should be assessed. Investigations should be ordered based on the history and clinical assessment. Basic investigations for lethargy are shown in Box 3.
{kind=link}
{kind=link}
Case scenario
A 35-year-old woman presents with a two-year history of worsening fatigue on a background of menorrhagia. She has three children aged between two and eight years. She is an administrative assistant for a financial services company and currently works from home due to COVID-19 restrictions. In the past four months she reports significant stress and anxiety from the COVID-19 situation, home-schooling and her husband’s job instability.
She has gained weight (10 kg) since her last pregnancy two years ago, and more recently due to reduced physical activity (BMI is now 31 kg/m2). Since her pregnancy, she has had reflux symptoms requiring regular proton pump inhibitor (PPI) therapy. Menstruation recommenced 12 months ago but her menses have been irregular, with four- to eight-week cycles and bleeding that lasts for up to seven days with pain and passage of clots. She and her husband use barrier contraception only. She sleeps well and has a healthy appetite. She minimises red meat intake for personal health reasons. She does not smoke and only drinks alcohol occasionally. There is no significant family history of diabetes or malignancy. She reports occasional dizziness and palpitations on standing but there are no other cardiopulmonary symptoms and no syncopal episodes. Bowel motions are regular with no change in colour or consistency. Blood pressure is 110/60 mmHg (supine) with no postural drop. Results of cardiac, respiratory, abdominal and pelvic examination are normal. There is no lymphadenopathy. She has no hirsutism or alopecia.
Commentary
What initial investigations should be ordered?
This patient’s symptoms and history suggest possible iron deficiency and/or anaemia caused by menstrual blood loss and insufficient dietary iron intake. A full blood count and comprehensive metabolic panel should be ordered, and urea, electrolyte, creatinine and fasting blood glucose levels should be measured. Liver function tests and iron studies should also be performed. Measurement of thyroid-stimulating hormone levels may also be part of an initial screen.
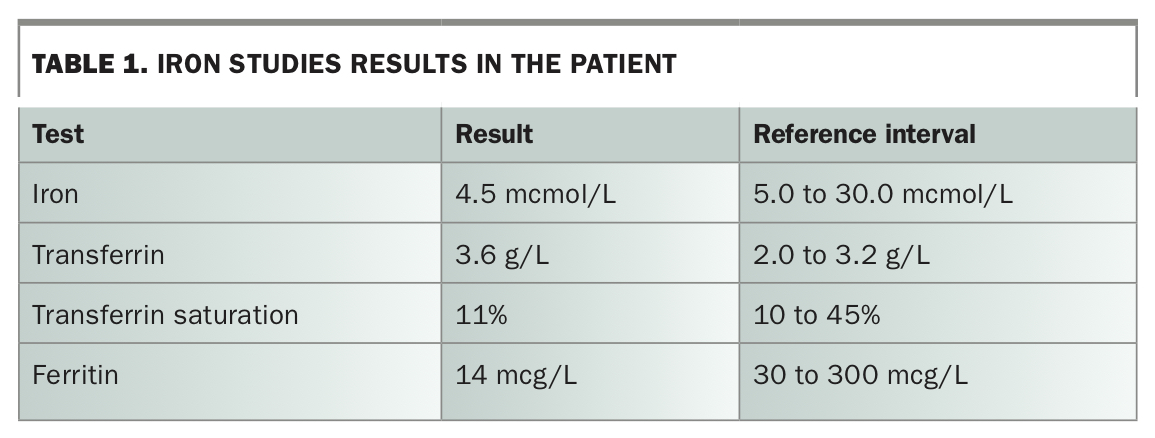
Investigations reveal a microcytic anaemia with a haemoglobin level of 106 g/L (normal range, 110 to 145 g/L) and mean cell volume of 78 fL (normal range, 80 to 96 fL). Iron studies show low iron and ferritin levels, low transferrin saturation and a high transferrin level consistent with iron deficiency (Table 1). Pelvic ultrasound findings are consistent with polycystic ovary syndrome (PCOS) with no evidence of uterine fibroid disease or endometrial thickening.
{kind=link}
What further investigations should be ordered?
Although menstrual blood loss is the most likely explanation for the patient's anaemia, differential diagnoses including menorrhagia due to underlying PCOS and impaired oral iron absorption due to gastrointestinal disorders should be considered. The patient meets the Rotterdam criteria for PCOS diagnosis. Coeliac serological testing (including immunoglobulin A and transglutaminase antibodies) may be carried out because it may be positive in the absence of symptoms and is recommended by some bodies as part of a lethargy screen. In this case, coeliac serology is negative. PPIs have been associated with decreased iron absorption due to inhibition of gastric acid secretion, as nonhaem iron requires gastric acid for absorption.10 A recent study showed PPIs also directly affect iron metabolism by suppressing iron absorption through upregulation of hepcidin.11
What is the diagnosis?
The diagnosis is iron deficiency anaemia due to PCOS-related menorrhagia, insufficient dietary iron intake and impaired iron absorption from long-term PPI use. The aetiology of her fatigue is likely to be multifactorial, based on the identified medical causes and further exacerbated by recent psychosocial stress.
How should this patient be managed?
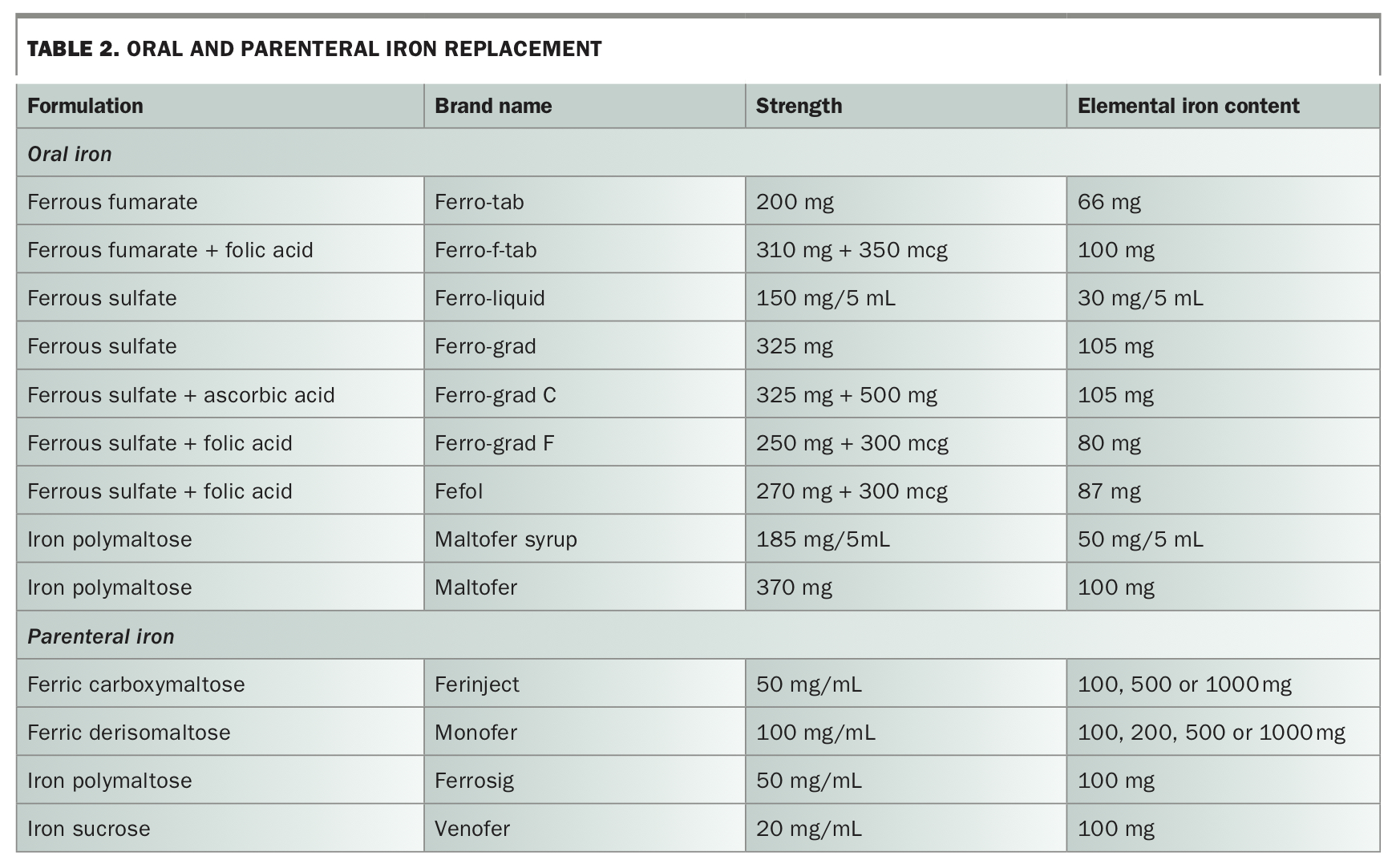
Oral iron replacement therapy (Table 2) for three months with repeat full blood count and iron studies one month after cessation of iron supplementation should be first-line therapy for this patient’s iron deficiency anaemia. The recommended dose in adults is 100 to 200 mg of elemental iron daily (in two to three divided doses).12 Gastrointestinal disturbance is the main adverse effect of oral iron therapy, which can be minimised by either using a lowered dose or taking the medication with food or at night.
{kind=link}
Parenteral replacement is indicated when oral iron therapy has failed or if rapid replenishment is required. A range of iron formulations for intravenous infusion (Table 2) are listed on the PBS. They vary in the ease and time required for administration, with some allowing up to 1000 mg elemental iron to be delivered over 15 to 20 minutes. Intramuscular iron therapy is painful and may cause permanent skin staining so is not recommended.12 Emergence of underlying bowel symptoms or failure to respond to either oral or parenteral iron replacement should prompt referral of the patient to exclude other causes of iron deficiency or loss.
Regarding the patient’s menorrhagia, gynaecological review may be considered to further investigate and alleviate patient concern over more serious causes. A multifaceted approach to the management of her PCOS is required. Lifestyle modification for the prevention and treatment of weight gain is key in management of PCOS.13 Beyond lifestyle modifications, treatment depends on specific symptoms such as menstrual irregularity, weight gain, hirsutism, acne and alopecia.13 Screening for emotional wellbeing is important as women with PCOS have increased rates of anxiety and depression.13 Management options include counselling, psychological treatments (particularly CBT) and pharmacological treatments.
It would be reasonable to consider replacing the PPI with nonpharmacological treatment to manage gastro-oesophageal reflux disease, or to reduce use to only intermittent use for symptoms. Modest weight loss (reduction in BMI of 3.5 kg/m2) has been shown to reduce reflux symptoms by nearly 40%.14 Long-term use (for two years or more) of both PPIs and histamine-2 receptor antagonists (H2RAs) is associated with increased risk of iron deficiency. The risk of developing iron deficiency is reduced after cessation of PPIs and H2RAs.10
Conclusion
Lethargy is a common presenting condition in general practice. Although some patients have reversible underlying pathology, careful history taking, examination and judicious use of investigations are important for identifying potential red flags that may indicate serious underlying medical or psychological pathology, as well as reassuring patients in whom lethargy may be a manifestation of nonpathological work-life pressures and stresses (i.e. most patients).15 It is important that GPs are familiar with the range of potential presenting features and underlying causes of lethargy, appropriate use of investigations and appropriate referral pathways. MT