Robotic head and neck surgery. A primer for GPs

Innovation and improvement in surgical technology have resulted in advances such as robot-assisted surgery. For a subset of patients with head and neck malignancies, particularly oropharyngeal carcinoma, transoral robotic surgery (TORS) offers a minimally invasive treatment option. The use of TORS has the potential to reduce morbidity and improve patients' quality of life. As more head and neck cancer patients are offered the option of robotic-assisted surgeries, patients will inevitably look to their GPs for advice and to seek answers.
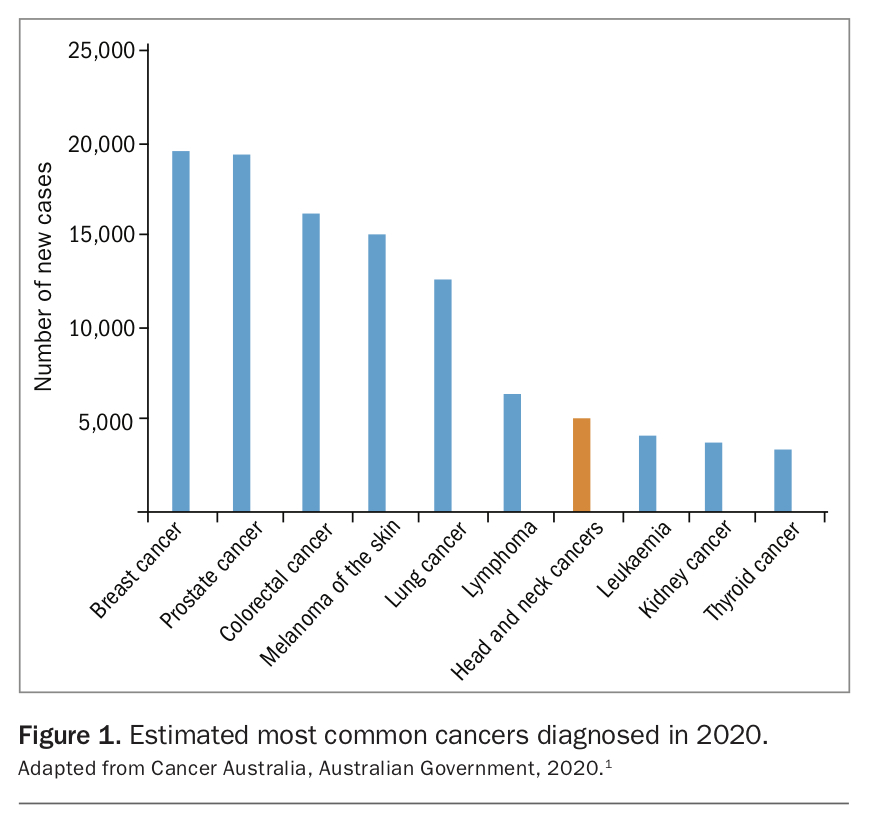
Head and neck cancer was the seventh most commonly diagnosed cancer in Australia in 2016 (Figure 1).1 An estimated 5,212 new cancer diagnoses (3.6%) in 2020 will be for head and neck cancer, with men accounting for nearly three-quarters of these cases. The five-year survival rate for patients with head and neck cancer between 2012 and 2016 was 71%.1 It is therefore important that we look at improving patients’ outcomes beyond that of survival.
{kind=link}
Although historically most cases of oropharyngeal squamous cell carcinomas were seen in older patients with a significant history of tobacco and alcohol use, the increase in human papillomavirus (HPV)-positive disease has changed the epidemiology and prognosis of this malignancy.2 The incidence of HPV-positive oropharyngeal squamous cell carcinoma has risen in recent decades. Furthermore, these patients tend to be younger, are more likely to be nonsmokers, diagnosed at an earlier stage and have a better prognosis than HPV-negative patients.2
Given that patients are younger and surviving longer, avoidance or minimisation of treatment-related toxicity is an important consideration when choosing treatment strategies. When deciding on a management plan for patients with early head and neck cancer, the multidisciplinary team aims for single-modality therapy; that is, to treat the cancer with either surgery or radiation therapy. In certain cases, neoadjuvant or adjuvant chemotherapy may also be required. By avoiding multiple modalities of treatment, morbidity is reduced and quality of life (QOL) improved. It has become clear over time that radiation therapy is associated with severe late onset toxicities, which can have a significant negative impact on the patient’s QOL. Adverse effects of this treatment modality include the need for dental extractions, xerostomia, loss of taste, radiation fibrosis, dysphagia, osteoradionecrosis and a high rate of prophylactic percutaneous endoscopic gastrostomy tube insertion. Surgery may therefore be a more viable treatment option for such patients. However, because of difficulties in obtaining access to the oropharynx and hypopharynx, surgical resection of certain head and neck carcinomas has traditionally been performed using ‘open’ methods. An example of these procedures is a mandibulotomy, which involves dividing the lower lip and mandible to expose the base of tongue, and is associated with significant morbidity with a lengthy hospital stay and recovery time. Minimally invasive options for treatment include transoral laser surgery and, more recently, transoral robotic surgery (TORS). This article outlines the two TORS systems currently used for head and neck surgery in Australia and discusses the potential benefits to patient outcomes.
What is the surgical robot?
The robotic surgical system allows the surgeon to perform minimally invasive surgery using advanced instruments. Patients may be confused when told that their surgery will be ‘robotic’ – it is therefore important to let them know that the surgery is still performed by a trained surgeon via a console in real-time, and not by a robot. There will still be a dedicated surgical team present in the room, as well as anaesthetic team among other operating theatre staff. The surgeon, surgical assistant and nurses are required to undergo mandatory comprehensive training before using the robotic surgical system.
In Australia, there are currently two surgical robots on the market that are being used by head and neck surgeons:
- da Vinci® Surgical System (Intuitive Surgical Inc., Sunnyvale, California, USA)
- Flex® Robotic System (Medrobotics Corporation, Raynham, Massachusetts, USA)
The da Vinci® surgical system
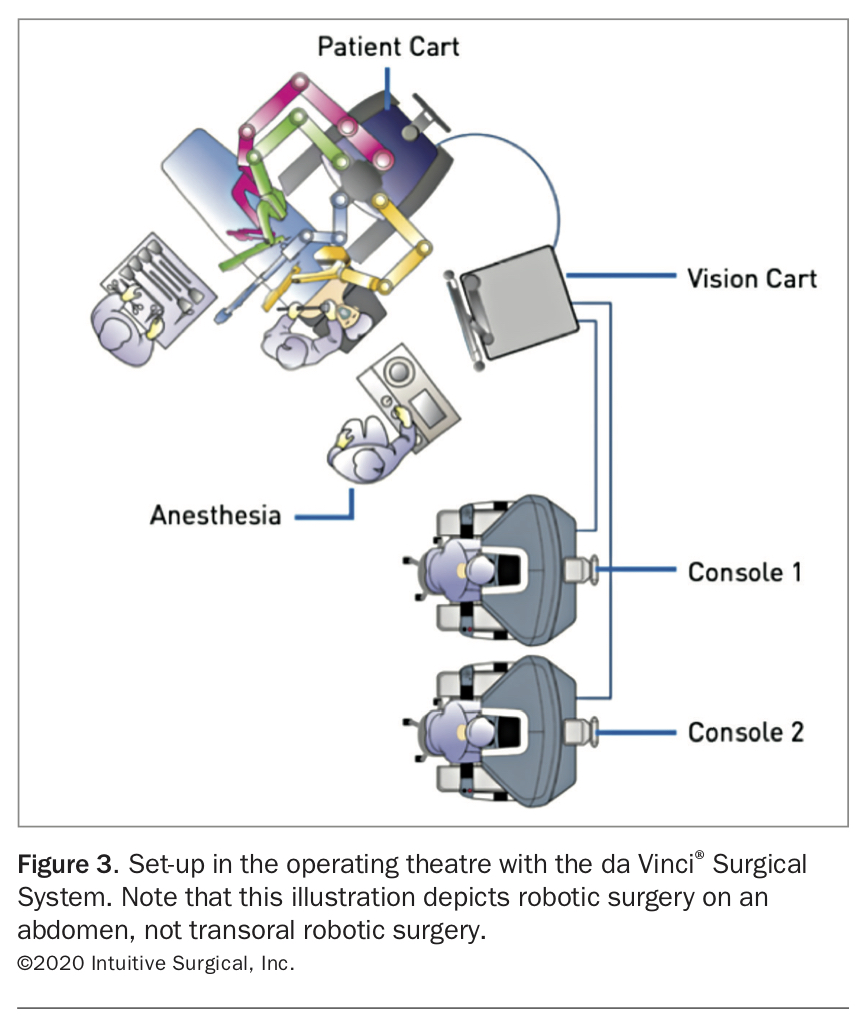
The da Vinci® Surgical System includes three major components: surgeon console; patient cart; and vision cart (Figures 2a to c, respectively). When using the da Vinci® system, the surgeon sits away from the patient at the surgeon console and uses the master controls and a foot switch to control the instruments. The patient cart is used to insert instruments into the patient via ports, and the surgical assistant adjusts the cart and changes instruments as required. The vision cart allows the surgical assistant, nursing staff and other staff in the operating theatre to visualise what the surgeon is seeing on their console (Figure 3 and Figure 4).
{kind=link}
{kind=link}
{kind=link}
Flex® robotic system
The Flex® Robotic System has a flexible robotic scope, which gives the surgeon the ability to gain access to the surgical site that may be in a nonlinear path, by manoeuvring around surrounding structures (Figure 5). This is particularly useful in transoral head and neck surgery, allowing easier access to the larynx and hypopharynx with good exposure. Unlike the da Vinci® Surgical System, with the Flex® Robotic System, the surgeon remains at the head of patient throughout the procedure.
{kind=link}
Why use the robot in head and neck cancer surgery?
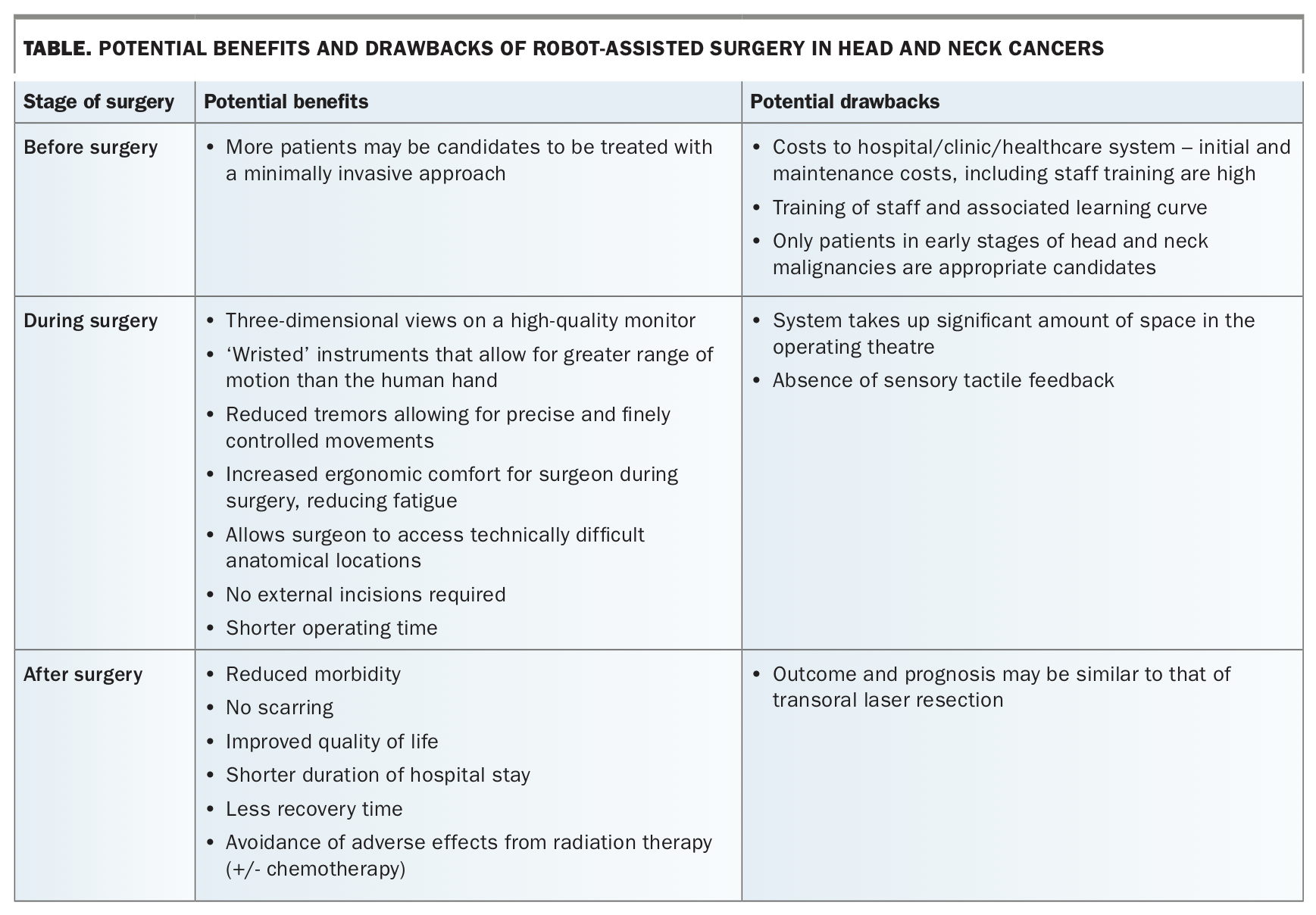
The robotic surgical system offers surgeons the ability to access anatomical locations that were previously difficult or impossible to reach without open surgery. The benefits and drawbacks of using the robotic surgical system in head and neck cancer resection are outlined in the Table.
{kind=link}
In general, TORS offers a less invasive operation with no external incisions compared with the traditional surgical approach, reduced recovery time and a shorter length of stay in hospital. Additionally, it eliminates the natural hand tremor, resulting in fine and controlled movements with the instrument tips.
The main drawbacks of robot-assisted surgery in head and neck cancers are associated with the purchase costs of the system, including ongoing maintenance of equipment, as well as the cost of training a surgical team. As with any new technique, surgeons, scrub nurses and surgical assistants must have introductory training, presenting a steep learning curve for all those involved. As such, it is not a technique that can be performed or is available widely across Australian hospitals. Moreover, although TORS itself does not result in an external scar, some patients who require an extensive TORS procedure may also need a neck dissection, which is performed via a large external neck incision.
When to use the robot
The decision to use the robot in head and neck cancers is one that is made by a multidisciplinary head and neck cancer team with consideration of patient, disease and healthcare system factors.
Patient factors
Factors that may make a patient an unsuitable candidate for TORS include anatomical characteristics that makes transoral access difficult such as reduced or limited mouth opening, narrow-arched mandible, full dentition and retrognathia.3 Additionally, patients need to be deemed fit for general anaesthesia, albeit for a shorter operating time than traditional open surgical methods, and must be able to stop anticoagulant medications before surgery.
Disease factors
The main indication for robotic-assisted surgery in the head and neck is for T1-T2 oropharyngeal carcinomas (up to 4 cm), including malignancies of the tonsils, base of tongue and supraglottis. Tumours of the hypopharynx can also be treated with TORS; however, access to this area of the upper aerodigestive tract is more challenging.
Cancers that are amenable to TORS tend to present in the younger population subset who are more likely to have HPV-positive disease. TORS has been most established in the treatment of these carcinomas, as it provides an alternative option to the more conventional treatment modality of primary radiotherapy (with or without chemotherapy). This results in the avoidance of the morbidity associated with radiotherapy and open surgery. In addition to benign and malignant tumours of the head and neck region, TORS has been used in the treatment of obstructive sleep apnoea, thyroid and parathyroid disease, and skull base pathologies.
Healthcare system factors
Despite the benefits of the surgical robot, purchasing and maintaining the robotic system comes with significant financial expense. At this stage, it is not an option that can be offered to patients in most public hospitals in Australia, particularly peripheral, regional and rural hospitals. In Australia, the cost of undergoing robotic-assisted surgery for head and neck cancers in the public healthcare system is covered by Medicare and there are therefore no out-of-pocket costs for the patient. There are also several private hospitals which have a robotic system, with trained surgeons working in these facilities. GPs who are looking to assist patients with accessing these facilities should refer to the Head and Neck Multidisciplinary Team of the patient’s local cancer centre. For those located in NSW and ACT, this can be found via the Canrefer website (www.canrefer.org.au).
Outcomes of using the robot
The outcomes of robotic-assisted head and neck surgeries have been promising thus far. A 2015 systematic review did not identify any randomised trials comparing TORS and radiotherapy for the treatment of oropharyngeal cancer.4 Based on nonrandomised studies, the review concluded that the two treatment modalities have comparable oncologic outcomes; however, functional outcomes may be superior in the TORS group.4 A 2014 systematic review concluded the two modalities differed in their toxicity and complication profiles. For those who underwent radiation therapy, adverse events included osteoradionecrosis of the mandible, oesophageal stenosis and gastrostomy tube placement. In patients who underwent TORS, adverse events included postoperative bleeding, neck haematomas, tracheostomy, gastrostomy tube insertion and pharyngocutaneous fistula formation.5
Since these reviews, there has been one completed randomised controlled trial comparing functional outcomes of radiotherapy (+/- chemotherapy) with TORS and neck dissection (+/- adjuvant therapy), published in The Lancet Oncology in 2019. The study, which included 68 patients from Canada and Australia with T1-T2, N0-2 oropharyngeal squamous cell carcinoma, found that those treated with radiotherapy demonstrated superior swallowing-related QOL scores one year after treatment compared with patients treated with TORS and neck dissection.6 However, the average differences between the two groups were below the threshold at which one would expect a clinically meaningful change.6 Furthermore, as most radiotherapy-related swallowing dysfunction occurs some years after treatment, it is difficult to draw conclusive evidence of comparative benefits from a 12-month follow-up period.
A systematic review comparing TORS with open surgery for oropharyngeal cancer found that the disease-free survival rate was significantly higher in the TORS group than the open approach group (relative risk, 1.13).7 Two of the included studies reported on disease-free survival at 3 years, while three had a 2-year follow up. There was no significant difference in complication rates between the two approaches.7 As expected, TORS resulted in significantly shorter hospital stays compared with open surgery (by 1.09 days in three concurrent studies and by 8.0 days in a fourth nonconcurrent study).7
Chemoradiation therapy remains the standard of care for comparison with TORS. To date, no randomised controlled trials have demonstrated a clear benefit of one modality over the other. Some observational studies have demonstrated QOL benefits of TORS; equally, others have highlighted that TORS can result in significant surgical complications. Therefore, a multidisciplinary team approach to treatment is essential. The potential treatment options should be discussed with the patient, who should be encouraged to be actively involved in the decision-making process. Management strategies should be individualised to each patient, taking into account their disease as well as personal factors including preferences and social situation.
Conclusion
The introduction of robotic surgical systems has given clinicians the opportunity to treat head and neck cancer patients with minimally invasive surgery instead of the traditional open surgery approach. TORS is being used more often and results in similar oncologic outcomes for patients when compared with open surgery and radiotherapy with or without chemotherapy. Patients whose cancers are amenable to TORS tend to be in the younger population subset. In these patients, there may be relative QOL benefits of TORS over the more conventional treatment strategy of radiotherapy. The decision to treat with TORS should be made by the multidisciplinary team in consultation with the patient. MT