Multiple sclerosis: the role of the GP in diagnosis and lifetime care

The diagnosis and management of multiple sclerosis (MS) are rapidly evolving areas. Although patients with MS are best managed by a multidisciplinary team, GPs have a pivotal role in their diagnosis and co-ordinating their management.
- Multiple sclerosis (MS) is the leading cause of nontraumatic neurological disability in young Australians.
- The presentation of MS is clinically heterogeneous.
- The diagnosis of MS continues to depend on proving dissemination of pathology in time and space.
- MRI has become increasingly important to both diagnosing and managing patients with MS.
- Multiple disease-modifying therapies are available in Australia for the treatment of relapsing-remitting MS, with different modes of action, efficacy, side effects and monitoring requirements.
- Symptomatic management is important in all forms of MS to treat residual neurological deficits.
Multiple sclerosis (MS) is the leading cause of nontraumatic neurological disability in young people and affects one in 1000 Australians.1 In Australia, women are three times as likely to be affected as men. Patients usually present between 20 and 40 years of age.
At some time in their career, most GPs will care for a patient with MS. This article aims to provide a practical, up-to-date resource on MS, with an emphasis on the role of the GP in patient diagnosis and management.
Pathophysiology of multiple sclerosis
Although the cause of MS is unknown, a key feature is immune dysregulation, with its effects restricted to the central nervous system (CNS), including the brain, spinal cord and optic nerves. The adaptive immune system is implicated in a complex immunological response, whereby lymphocytes in the periphery, outside the CNS, are activated and trafficked into the CNS, causing focal inflammation. Previously, MS was widely considered an exclusively T cell lymphocyte-mediated disease, but recent advances in the understanding of its pathophysiology and therapy have highlighted a crucial role for B cells, likely by activating T cells via cytokine production, co-stimulation and antigen presentation. Focal inflammation within the CNS results in demyelination and axonal transection, features of acute MS plaques.
In addition to adaptive immune mechanisms, local (innate) inflammatory responses within the CNS are activated in MS, involving microglia and macrophages. Repeated inflammatory insults and chronic local inflammation lead to gradual neurodegeneration from axonal transection and loss, which is the principal pathological substrate for accumulating disability.
Several risk factors for MS have been identified, including exposure to Epstein-Barr virus, changes in the gut microbiome, smoking, vitamin D deficiency and upbringing in higher latitude locations, possibly as a result of decreased sun exposure influencing the immune system.
In addition, over 200 genetic associations have been described for MS. Most are associated with the architecture of the immune system, such as the major histocompatibility complex. Despite this broad genetic influence, the MS concordance rate in monozygotic twins is 30%, suggesting that an environmental trigger is required. The lifetime risk of MS in first-degree relatives of patients with the condition is of the order of 2 to 4%. However, at a background population incidence of about 0.1%, most patients with MS do not have a known family member with the disease.2
Clinical presentation
In MS, focal inflammatory lesions or plaques cause focal neurological deficits if they occur in an area of the CNS that directly controls function. This is termed a relapse or attack. A relapse has a characteristic temporal evolution, usually developing over two to three days, reaching a peak of intensity or severity at one to two weeks and then remitting over another one to two weeks. The degree of improvement varies, ranging from complete resolution of symptoms to severe residual deficits. This form of MS is termed relapsing-remitting MS. Symptoms that last less than 24 hours or have an abrupt onset with fixed deficits are not typical and should lead to consideration of other aetiologies, such as vascular insults.
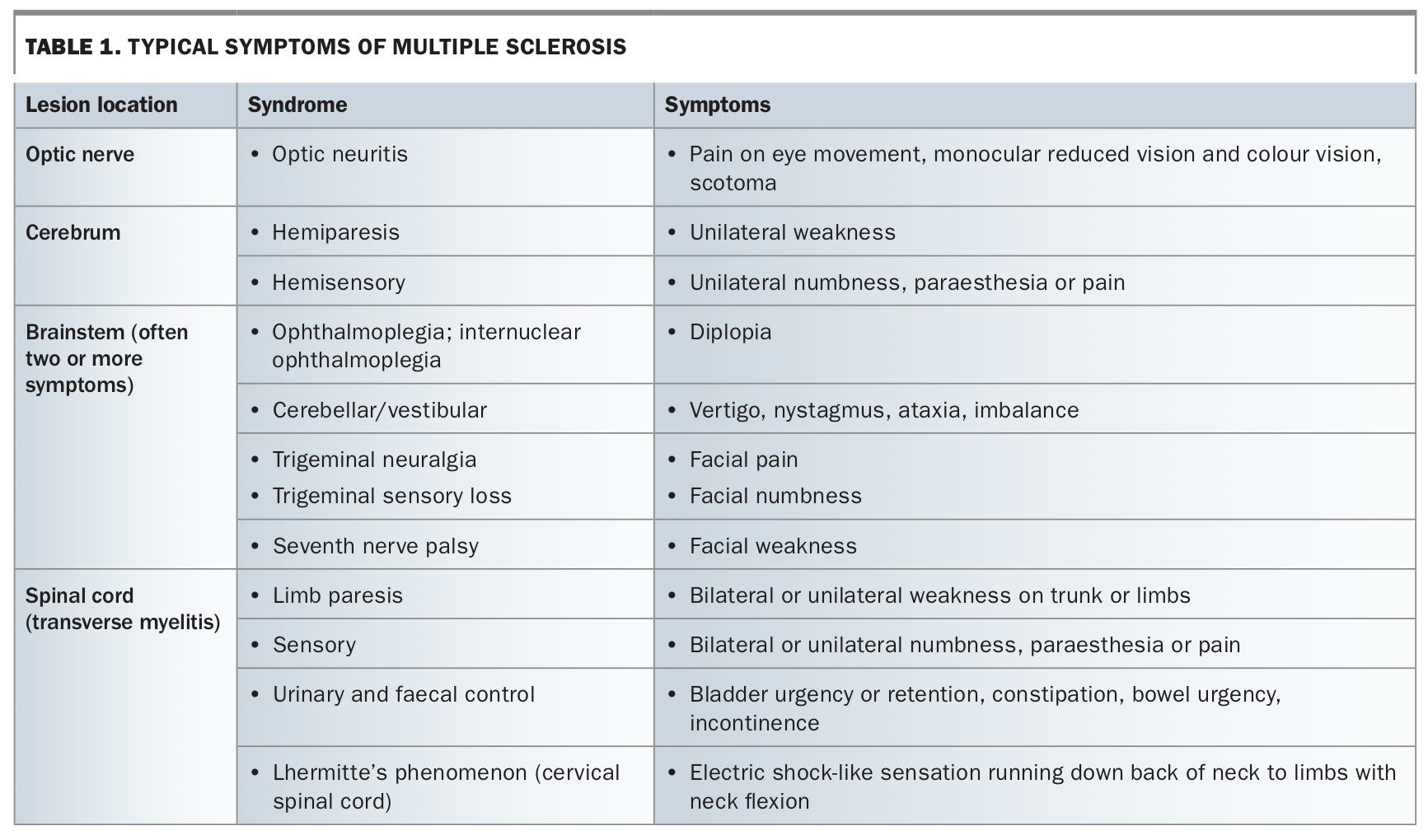
The symptoms of MS relapses are heterogeneous, reflecting the variable location of plaques within the CNS. Some of the more typical symptoms are shown in Table 1.
{kind=link}
Diagnosis of multiple sclerosis
The diagnosis of MS has been codified since 2001 with the McDonald criteria, which are regularly updated. The essence of these criteria is to prove that inflammatory/demyelinating events have occurred in more than two locations in the CNS and at more than two time points, fulfilling the requirement for there to be ‘dissemination in space and time’. It is imperative that other causes of symptoms are excluded, as described below.
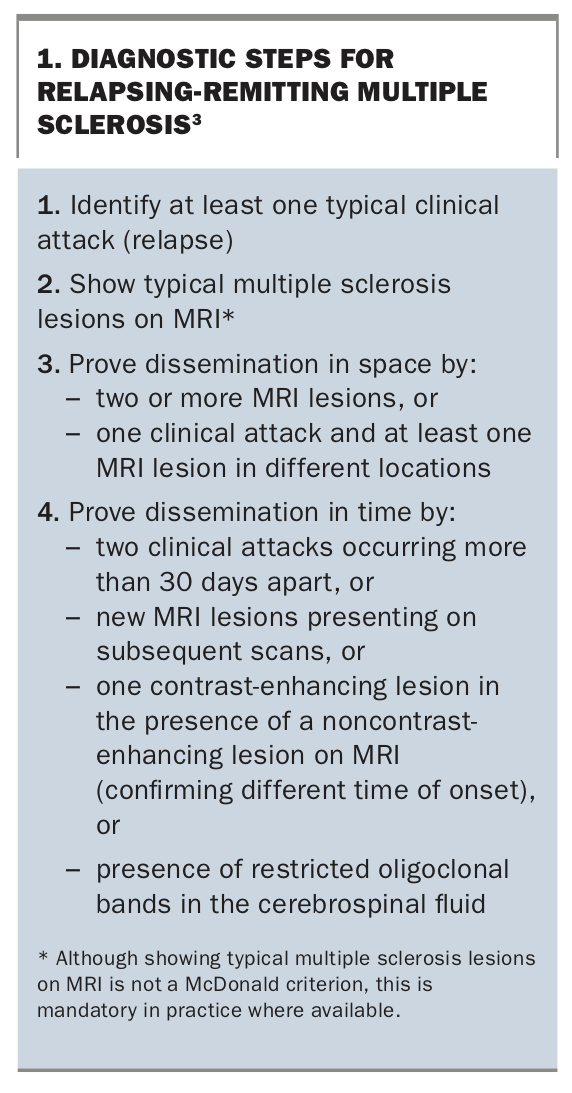
Demyelinating events can be identified by the occurrence of typical clinical attacks or their typical appearance on MRI. The McDonald criteria for MS were most recently updated in 2017, and the steps to satisfying these are shown in Box 1.3 The 2017 criteria newly allow for dissemination in time to be proven by the presence of restricted oligoclonal bands in the cerebrospinal fluid, representing specific antibody proteins, which suggest inflammation is ongoing as opposed to monophasic. In addition, at least one clinical attack (relapse) must occur to meet the diagnostic criteria for relapsing-remitting MS. Although the 2017 McDonald criteria do not require MRI, this is essentially mandatory where available as the absence of typical demyelinating lesions on MRI make the diagnosis of MS highly unlikely.
{kind=link}
Disease course
In 85% of patients with MS, the initial course of MS is relapsing-remitting. A patient presenting with their first typical demyelinating relapse that does not satisfy the McDonald criteria is classified with ‘clinically isolated syndrome’. These patients require regular monitoring to assess for any further inflammatory activity that would prove the diagnosis of MS.
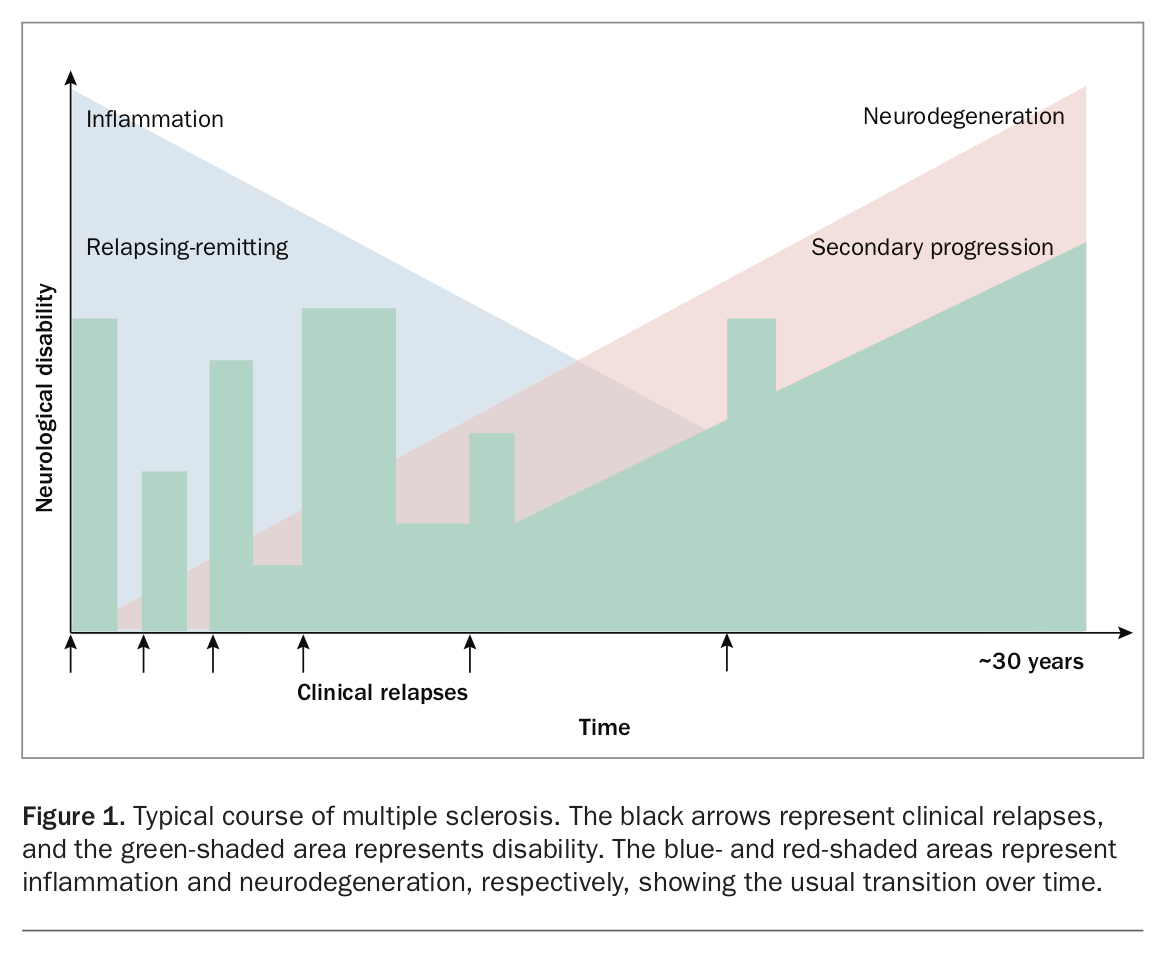
A proportion of patients with relapsing-remitting MS develop gradual progressive disability in the absence of relapses, termed secondary progressive MS (Figure 1). This typically occurs at 10 to 15 years after disease onset in untreated patients. In addition, 15% of patients present with progressive disease in the absence of relapses from disease onset, termed primary progressive MS. The pathological substrate of progressive disease is gradual neuroaxonal loss both within and outside MS plaques, leading to brain and spinal cord atrophy.
{kind=link}
Although the above disease stages and disease courses are widely accepted and applied in clinical practice, it has become evident that neurodegeneration and markers of progressive disease are present at the earliest stages of MS. Thus, the categories of relapsing and progressive disease exist on a spectrum (Figure 1).
MRI criteria for multiple sclerosis
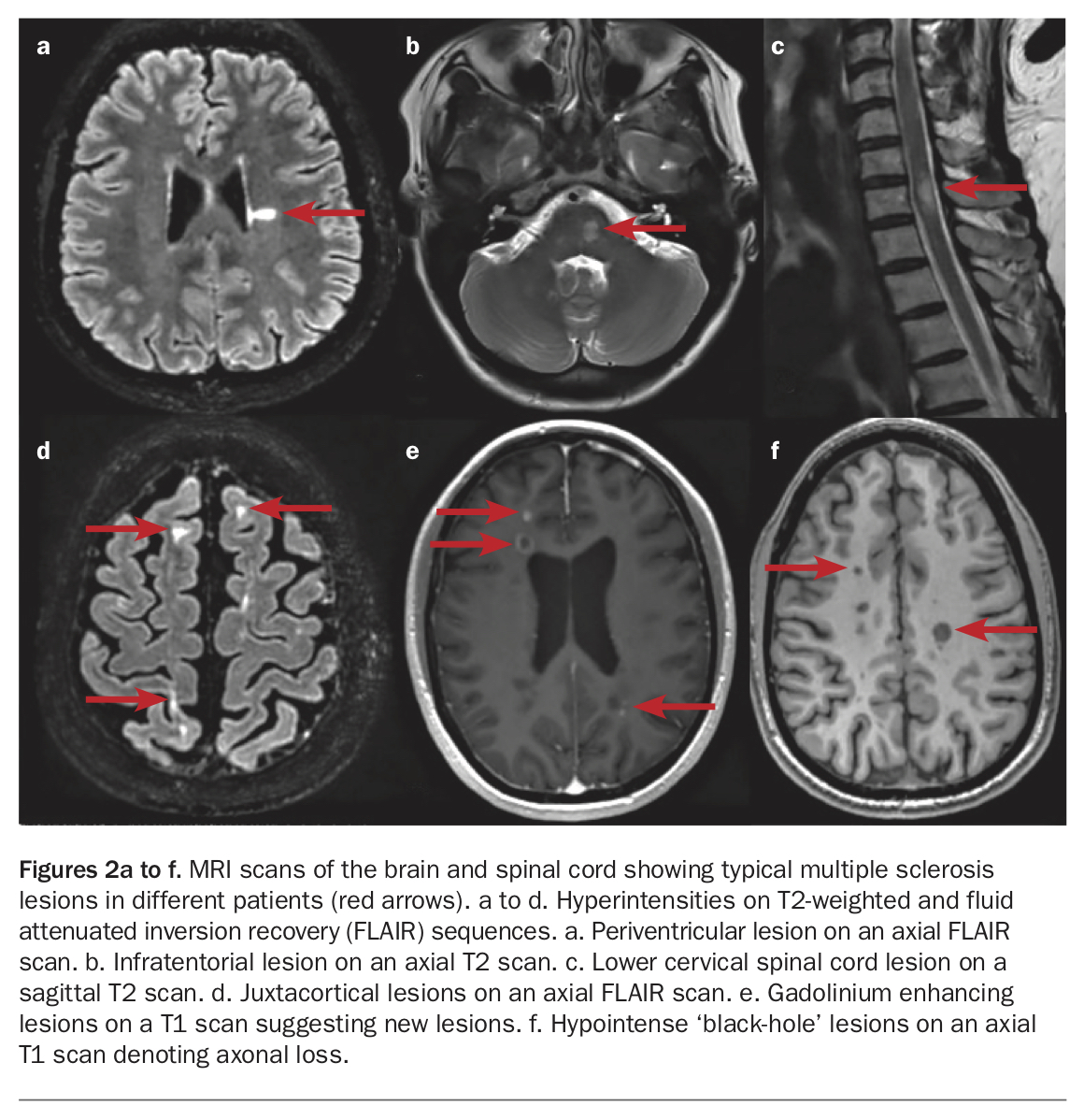
MS lesions of all ages appear as hyperintensities in the white matter on T2-weighted and fluid attenuated inversion recovery (FLAIR) MRI sequences (Figures 2a to d). Areas of hypointensity on T1-weighted MRI sequences denote loss of axons and are termed ‘black holes’ (Figure 2f). However, acute lesions may also appear hypointense owing to oedema.
{kind=link}
New lesions typically show gadolinium contrast enhancement up to eight weeks after formation, allowing their age to be determined, and thus contribute to satisfying the diagnostic criterion of dissemination in time (Figure 2e). Lesions must be present in at least two of four regions (periventricular, juxtacortical/cortical, infratentorial and spinal cord) to meet the diagnostic criteria for MS in patients with a typical clinical syndrome.
Many neurological conditions may present with white matter lesions or hyperintensities, and often the diagnosis is not clear on initial imaging, requiring follow-up imaging and other investigations. It is important that the diagnosis is clear before embarking on treatment decisions. A nonexhaustive list of differential diagnoses for MRI white matter hyperintensities is shown in Box 2.
{kind=link}
Assessment of patients with suspected multiple sclerosis
GPs who see patients with a new neurological deficit are able to assess for the likelihood that MS or inflammatory/demyelination is the underlying cause. Features to assess on history taking are shown in Table 2.
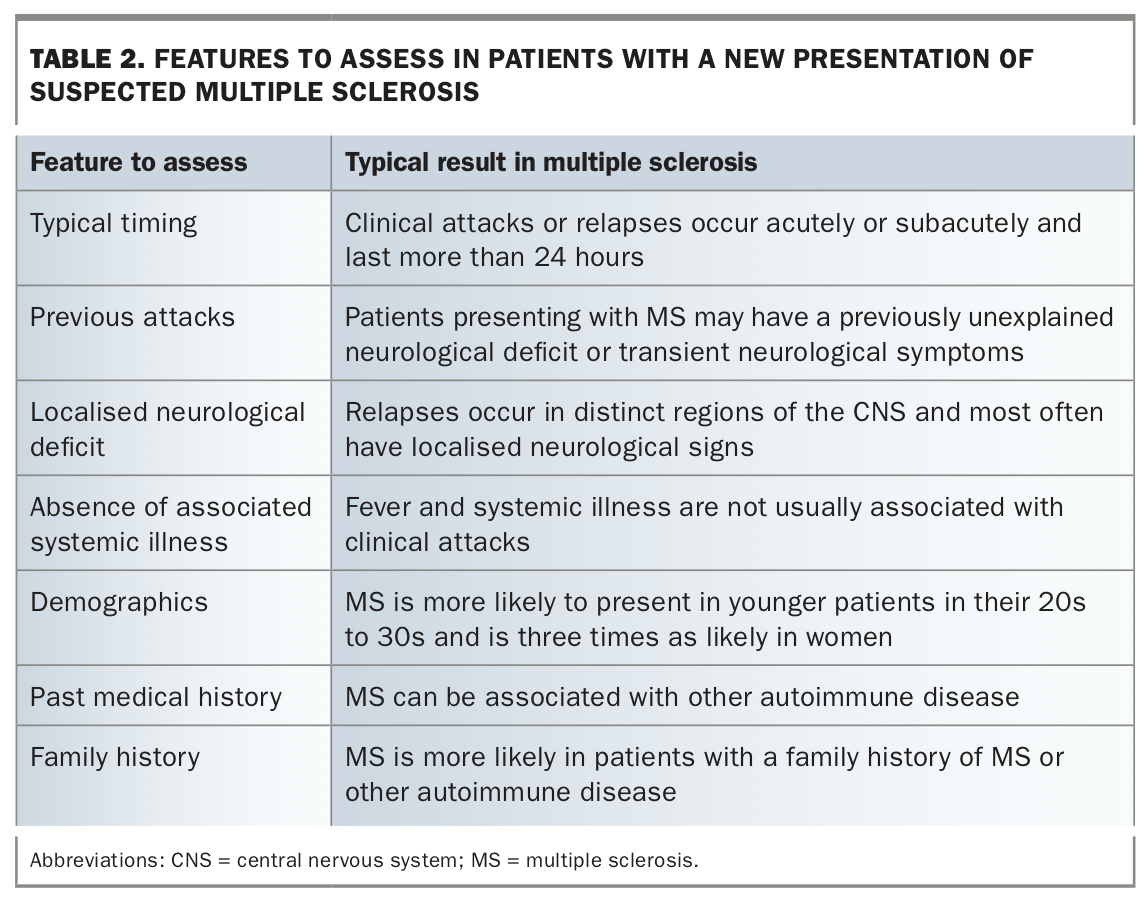{kind=link}
Diseases that can mimic MS
Essentially, any disease that causes transient or fixed neurological deficits can mimic MS.
- Stroke and transient ischaemic attack are common in older populations, due to cerebrovascular disease, but can also occur in younger patients as a complication of thrombophilic disease, drug use or comorbidities. Ischaemic strokes develop suddenly and are less likely to evolve than MS relapses.
- Migraines often have visual, brainstem or sensory effects or even weakness associated with their aura.
- Focal nonconvulsive seizures or deficits following a convulsive seizure (Todd’s paresis) may mimic MS, although seizures themselves are only rarely features of MS.
- Peripheral nerve lesions, including those resulting in foot drop or carpal tunnel syndrome, also cause focal deficits.
- Other neuroinflammatory diseases often present similarly to MS but are much rarer in prevalence.
Any transient or fixed neurological deficit that is not readily explained by a known or benign cause should be promptly investigated, or the patient referred to a neurologist for assessment.
Initial investigations
The initial investigations for patients with possible MS are likely to be started by the GP and completed by the neurologist. The aim of the investigations is to confirm demyelination and to rule out other causes of the patient’s symptoms or the MRI appearance. Potential investigations to assess for MS are listed in Table 3.
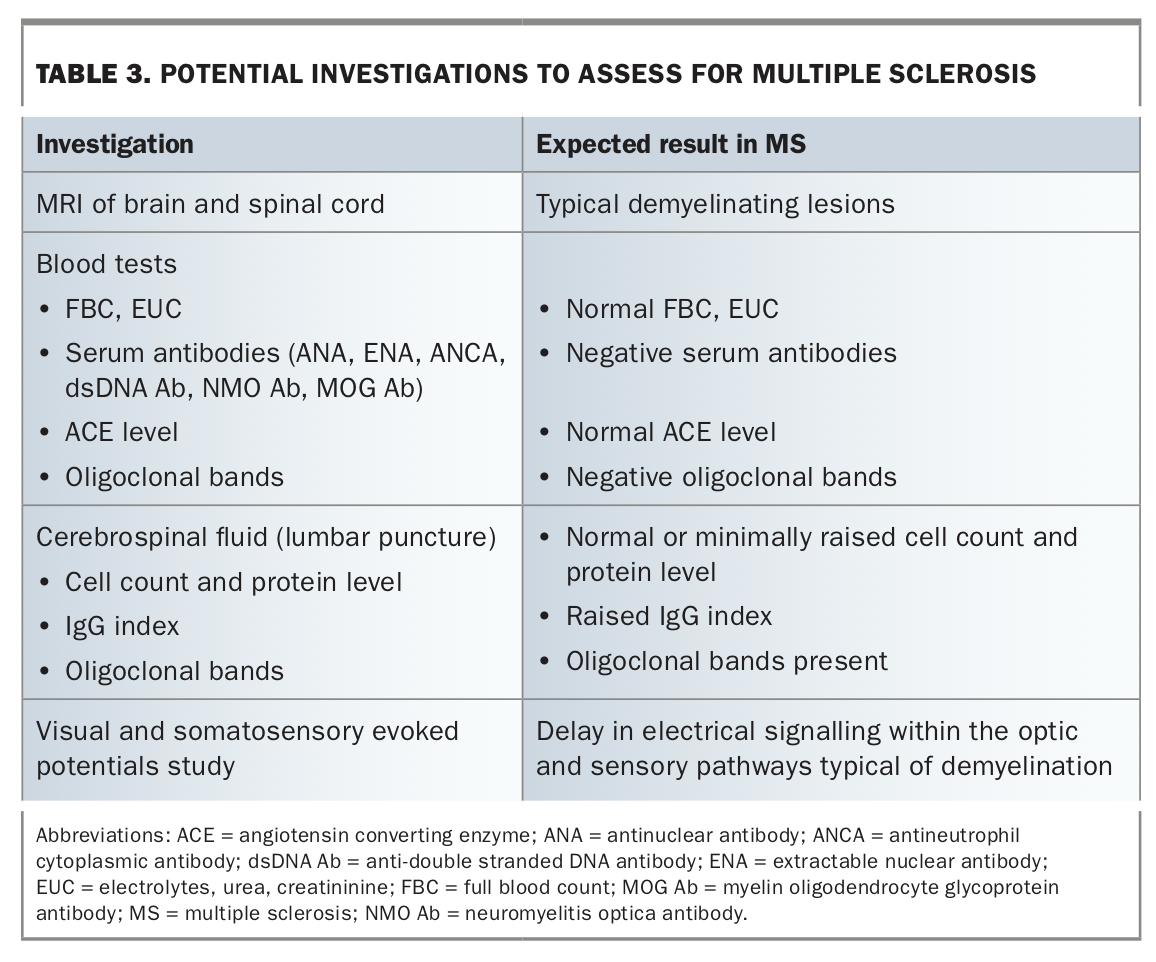{kind=link}
As evident in the modern criteria for MS, it is not necessary to assess the cerebrospinal fluid or evoked potentials in every patient. These are typically assessed when doubt remains after other investigations, and more evidence of inflammation or demyelination is wanted.
Management of multiple sclerosis
GPs have a pivotal role in co-ordinating the management of patients with MS. MS is a lifelong disorder with the potential to cause significant physical, cognitive and mental health disability. Patients are best cared for by a multidisciplinary team, of which GPs are a crucial part.
The management of MS from a GP’s perspective can be categorised into the following domains:
- evaluating and treating acute relapses
- supervising disease-modifying therapies
- managing adverse effects and risk minimisation
- implementing effective treatment of symptoms related to neurological deficits.
Acute treatment of relapses
Relapses are classified as new neurological deficits that last longer than 24 hours. It is important to differentiate a new relapse, which is related to new focal inflammation within the CNS, from fluctuating residual neurological deficits, termed ‘pseudorelapses’. Pseudorelapses occur with intercurrent illness, infection or fever, and are fully reversible after the comorbid condition subsides. They typically represent a worsening of pre-existing neurological deficits but may not necessarily be recognised as such by the patient. When a patient presents with acutely worsening neurological symptoms, it is important to appraise for intercurrent illness with a physical examination, blood tests and urine culture where appropriate.
New relapses resulting in significant disability are treated with high-dose corticosteroids, usually in the form of intravenous methylprednisolone 1 g daily for three to five days. Corticosteroid treatment hastens recovery from relapses and, although there is conjecture as to whether it ultimately alters the final natural course of the relapse, there is MRI evidence of long-term benefit.4 Most relapses are treated in the same way, although minor relapses such as mild paraesthesiae might be monitored first for evolution before committing to high-dose corticosteroids.
Forecasting problems that may arise with high-dose corticosteroid treatment is an important aspect of management. Potential problems include altered blood glucose control in patients with diabetes mellitus and insomnia and mood disturbance in certain patients. Stratifying the risk of avascular necrosis is also important.
In exceptional circumstances, when corticosteroids are contraindicated or when a severe relapse is unresponsive to corticosteroids, early treatment with plasma exchange is indicated. There is less evidence to support intravenous immunoglobulin in these settings, but it may be considered. These treatments are usually delivered in a hospital inpatient setting.
Disease-modifying therapies
The range of disease-modifying therapies (DMTs) for MS has expanded greatly in the past decade. DMTs are effective in preventing new MS lesions and relapses, but have little or no effect on past lesions or accrued disability. For these reasons there is a focus in the MS neurology community to treat patients with higher-efficacy medications earlier.
The development of effective treatments for relapsing-remitting MS is a remarkable achievement, all the more impressive considering most new medications have different mechanisms of action and are true alternatives. In Australia, most DMTs are funded by the PBS for the treatment of relapsing-remitting MS.
The choice of treatment is a complex decision that involves weighing the efficacy of treatment against its risks, as well as considering the patient’s preferences. The choice is made with the treating neurologist. DMT options for MS are shown in Table 4.
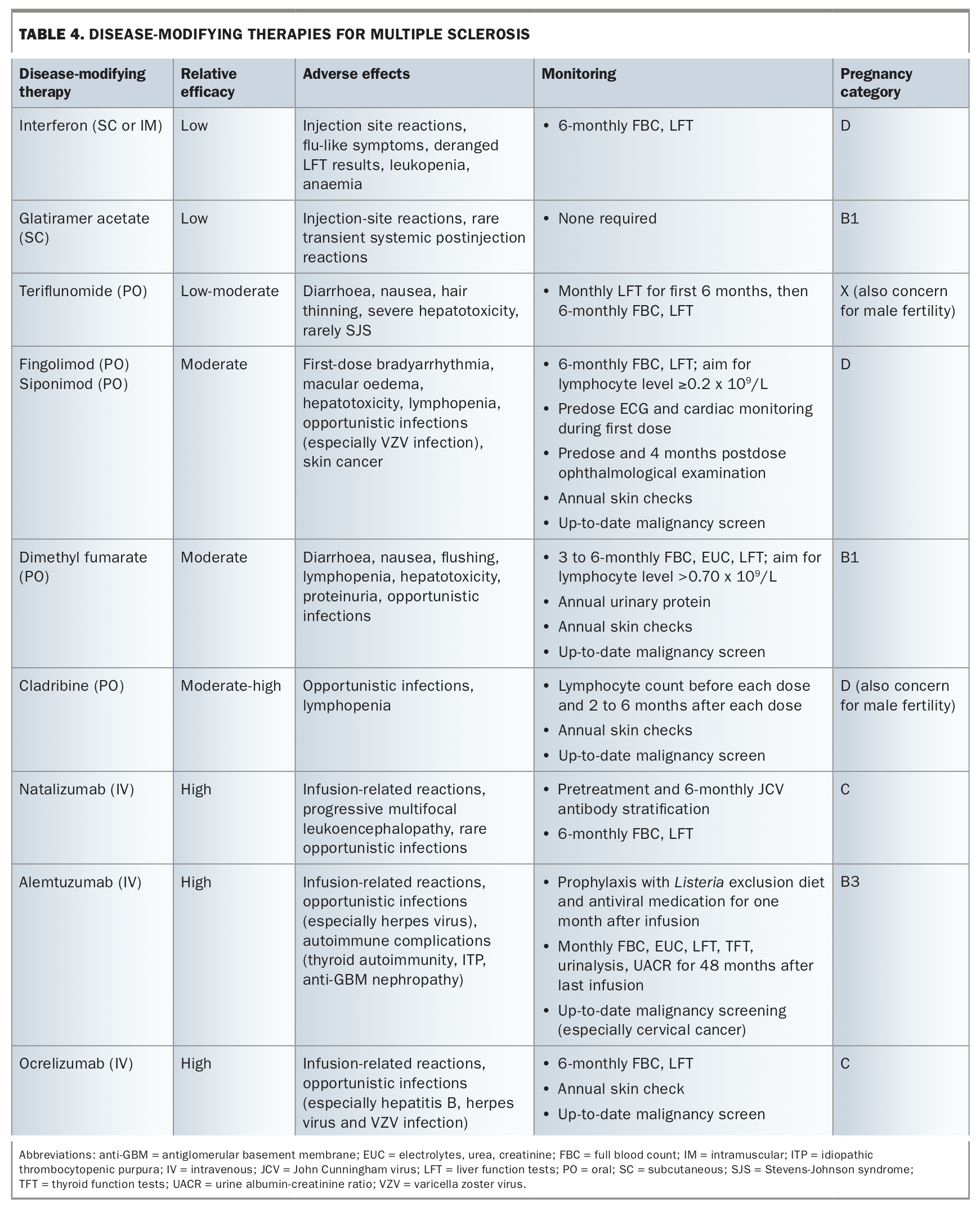{kind=link}
Screening and vaccination
It is important for the GP to be aware of the risks of DMTs and the appropriate monitoring and risk minimisation practices. In general, all DMTs for MS are immunosuppressive to some extent, except the low-efficacy injectable medications. Patients should be assessed clinically and serologically for latent infections and their immunity to preventable infections. Where indicated, they should be treated or vaccinated before commencing DMT. Live attenuated vaccines, such as varicella zoster, measles, and yellow fever vaccines, are contraindicated after immunosuppressive therapy has begun.
In addition, baseline routine screening for malignancy should be complete before commencement of immunosuppressive DMTs. This includes cervical cancer, breast cancer and bowel cancer screening for the appropriate populations. Follow-up screening is undertaken as per routine guidelines for the general population, except for the requirement for annual skin checks with some DMTs (see below).
Therapy for progressive MS
All current DMTs act by modulating or suppressing the immune system. Two of these medications have shown some effect on progressive MS: ocrelizumab for primary progressive MS, and siponimod for secondary progressive MS. The effect of these medications is modest, and they do not reverse or stop progression but potentially slow accrual of disability. The need for effective treatments for progressive forms of MS is still largely unmet.
Symptom management
GPs are often the first to institute management of symptoms related to neurological dysfunction in patients with MS. It is important to have a working management framework for common issues experienced by patients with MS.
Bladder symptoms
Bladder dysfunction is common in patients with MS. Broadly, there are two categories of dysfunction:
- failure of bladder storage, which results in symptoms of urinary urgency, frequency and urge incontinence
- failure of bladder emptying, which results in symptoms of urinary retention, hesitancy and infections.
The two forms of dysfunction may co-exist, producing complex symptoms and management problems.
Initial investigations after history taking should include urinalysis and culture to identify infection and measurement of the postvoid residual by ultrasound examination. A postvoid residual greater than 100 mL indicates failure of bladder emptying and is a risk factor for urinary tract infections, calculi and hydronephrosis.
Initial treatment of failure of bladder storage is reduction in fluid intake as appropriate and regimented toileting through the day. Anticholinergics are useful, including oral or transdermal oxybutynin (available on the PBS), or solifenacin or mirabegron, which may have fewer cognitive side effects (but are not available on the PBS). Careful monitoring for symptoms of urinary retention is required after starting these medications, and follow-up measurement of postvoid residual is often helpful. Nocturia may be treated with a reduction in afternoon and evening fluid intake, or intranasal desmopressin, which can have hyponatraemia as a side effect.
Patients with failure of bladder emptying can trial alfa-antagonists including prazosin or tamsulosin. Intermittent clean catheterisation is often necessary.
Urinary problems that persist despite these measures or have complications are often best investigated by a urologist with expertise in neurogenic bladder disorders, who can perform urodynamic studies, cystoscopy, administration of intravesical botulinum toxin and other procedures.
Bowel symptoms
Neurogenic bowel symptoms include constipation, poor evacuation, urgency and incontinence. In addition, decreased physical activity contributes to bowel dysfunction. Treatment includes increasing fluid intake and dietary fibre, and laxatives, especially bulking agents.
Pain
Pain can result directly from MS lesions, such as in trigeminal neuralgia or spinal cord lesions, or from musculoskeletal pain as a result of physical disability. Treatments for neuropathic pain such as pregabalin, gabapentin, amitriptyline and duloxetine are useful. Trigeminal neuralgia is best managed with carbamazepine.
Spasticity
Spasticity, usually of the legs, is common in patients with MS and affects comfort, sleep and walking. Physical therapy with exercise and stretching is often helpful in minimising spasticity and reducing complications of fixed contractures.
Baclofen is a muscle relaxant that eases spasticity and spasms but can cause cognitive symptoms and muscle weakness. Careful assessment for leg weakness is necessary to ensure baclofen does not impair standing or walking. Intramuscular botulinum toxin and intrathecal baclofen pumps are advanced options for severe spasticity.
In addition, the cannabinoid extract nabiximols is TGA-approved for symptomatic treatment of moderate to severe spasticity due to MS (see below). The alfa-agonist tizanidine is available through a special access scheme for treatment of spasticity where other treatments have failed. There is also evidence that the potassium-channel blocker fampridine can improve walking speed in patients with MS, possibly due to restoration of neuronal conduction in demyelinated axons within spinal cord lesions. The response varies between patients, so a short trial is often used to assess for benefit.
Fatigue
MS-related fatigue is a common symptom and generally is difficult to treat. Patients describe it as physical exhaustion and as pervasive through the day, with exacerbations often related to heat and exertion. Some patients may get relief with rest or daytime sleep. Medications that may be useful include stimulants such as modafinil (off-label), dexamphetamine (off-label) and methylphenidate (off-label), as well as amantadine (off-label) and selective serotonin reuptake inhibitors (off-label).
Depression and cognitive impairment
Depression and cognitive impairment are common symptoms of MS and often coexist and influence each other. Depression is managed similarly in patients with MS as in other patients, with exercise, psychotherapy and pharmacotherapy where appropriate. Consideration of the side-effect profile of antidepressant medications is suggested to improve tolerability.
Cognitive impairment is managed by teaching coping strategies and engaging supports. Cognitive rehabilitation techniques have had mixed results, and research is ongoing.
Advances in therapy for multiple sclerosis
Stem cell transplantation
The role and place of autologous haematopoietic stem cell transplantation (AHSCT) in the treatment of MS is still being explored and debated. AHSCT may be as effective as the highest efficacy therapies currently available for the treatment of relapsing-remitting MS, and the risks have improved in recent years with new ablative regimens. However, the long-term benefit is still unknown. AHSCT is offered in only a few centres in Australia, where the treatment is largely restricted to patients with active disease despite conventional, high-efficacy therapy.
Therapy for progressive MS
The remarkable expansion of the therapeutic armamentarium for relapsing-remitting MS has not been matched by treatment advances for progressive forms of MS. However, modest inroads have been made with ocrelizumab in primary progressive MS and siponimod in secondary progressive MS. In addition, much research is underway on treatments to promote remyelination and counter neurodegeneration, quite separate to modulating the immune system.
Role of cannabinoids in MS
Research on the use of cannabis derivatives in patients with MS has expanded in recent years. There is modest evidence supporting specific formulations in reducing MS-related spasticity, and possible evidence supporting their use in the treatment of MS-related pain. There are numerous cannabinoid formulations, which vary in their concentrations of specific cannabinoids such as tetrahydrocannabinol (THC) and cannabidiol (CBD).
In Australia, the TGA has licensed nabiximols, which contains both THC and CBD, for use in patients with MS-related spasticity. Cannabinoid use in general may be limited by low efficacy, side effects and restrictions on driving, especially for the psychoactive agent THC.
Conclusion
The diagnosis of MS can be challenging, and management advances are being made continually. Patients with MS are best cared for by a multidisciplinary team, with GPs playing a crucial role. Early recognition of a potential MS diagnosis, timely referral to a neurologist, identification of relapses, monitoring of MS disease-modifying therapies and symptom management are all key areas to be addressed in primary care. MT