Treating family, friends and colleagues: ‘It’s just not appropriate’
Articles in this series highlight common medicolegal issues in general practice. Written by the claims and advocacy team at medical defence organisation Avant, the series is based on actual cases, with some details changed for privacy. The case of a GP whose de facto partner died after being treated by the GP for severe headaches illustrates some of the risks of treating individuals with whom you have a close personal relationship.
As a medical practitioner, you may be asked for your medical opinion or a prescription by a family member, friend or someone you work with. It may be difficult to refuse. However, if a doctor writes even a one-off prescription or referral for such a person then an inherent conflict of interest arises between the doctor-patient therapeutic relationship and the doctor’s personal relationship with the person.
In October 2020, the Medical Board of Australia’s new code of conduct for doctors in Australia came into effect, including revised guidance on treating people with whom the doctor has a close personal relationship.1 The following scenario of a GP who prescribes medications for her de facto partner illustrates some of the risks in this situation.
Case scenario
Dr Smith is a GP whose de facto partner, Mr Wilson, develops severe debilitating headaches. Dr Smith gradually becomes Mr Wilson’s primary medical provider and soon after diagnoses him with ‘cluster headaches’. Over the next two years, Dr Smith prescribes medications, including morphine, pethidine, other injectable pain relief and psychotropic medications, writes referrals and accompanies Mr Wilson to medical appointments. During this period, two specialists raise their concerns with Dr Smith about her being Mr Wilson’s treating practitioner as well as his partner.
Mr Wilson subsequently dies from a self-administered overdose of amitriptyline. Following an inquest into Mr Wilson’s death, the Health Care Complaints Commission undertakes an investigation into Dr Smith’s conduct. The findings of the investigation ultimately lead to Dr Smith appearing before the Medical Tribunal of NSW.
Discussion
The latest version of Good medical practice: a code of conduct for doctors in Australia from the Medical Board of Australia came into effect on 1 October 2020 and includes revised guidance about treating anyone with whom the doctor is in a close personal relationship. The Code states, ‘Whenever possible, avoid providing medical care to anyone with whom you have a close personal relationship. In most cases, providing care to close friends, those you work with and family members is inappropriate …’.1
In particular, the Code states that doctors must not prescribe certain medications or perform elective surgery on any individual with whom they have a close personal relationship. However, the Code recognises that it may sometimes be unavoidable to provide care, such as in an emergency.1
Risks when treating family, friends and colleagues
Lack of objectivity and professional distance
Medical practitioners will find it difficult to maintain objectivity and an appropriate professional distance when treating family, friends and staff or colleagues because of the conflict between the personal relationship and the doctor’s professional obligations. For example, it may be difficult for a doctor to avoid being pressured into providing treatment they would not normally consider to be in the patient’s best interests. In the case of Dr Smith and Mr Wilson, the close personal relationship between the doctor and patient meant that the patient was denied objective medical treatment. Two specialists expressed their concerns about this, and one commented specifically on Dr Smith’s lack of objectivity.
Further, the nature of the doctor-patient relationship may be influenced by what the doctor knows about the patient from outside the consultation. The personal relationship may influence both what the doctor asks or does and what the patient tells the doctor. This may mean the doctor does not assess the patient adequately.
Formulating a treatment plan usually requires taking a complete history from a patient and full physical examination. If there is a personal relationship between the doctor and patient, this process may be uncomfortable for both parties, especially when sensitive questions or examination are needed.
There is also a risk that crucial information could be missed, impacting on patient management. Gaps in information may mean a failure to arrange or follow up in appropriate investigations and referrals, potentially leading to a missed or delayed diagnosis.
Patients may also feel more inclined to proceed with treatment recommended by a doctor with whom they have a personal relationship. This could compromise patient autonomy and bring into question whether proper informed consent was obtained.2
Discontinuity of care
Ensuring continuity of care is crucial to patient management. Continuity of care may be affected when medical practitioners do not keep accurate records, for example of informal discussions or one-off prescriptions or referrals. This may mean other practitioners do not have the complete clinical picture, potentially compromising patient care.
The Code states that ‘maintaining clear and accurate medical records is essential for the continuing good care of patients’.1 Records should include sufficient information to facilitate continuity of patient care.1 Record keeping is also covered by legislation in some states and territories.
In the case of Dr Smith, the Tribunal held that she failed to maintain adequate records regarding consultations with and services to Mr Wilson, including records of prescriptions. Further, she arranged referrals to seven different specialists, none of whom had sufficient accurate information to enable them to conduct a comprehensive assessment. It was found that Dr Smith withheld crucial information from most of Mr Wilson’s specialists.
Inappropriate prescribing
The Code states that doctors must not prescribe Schedule 8, psychotropic medication and/or drugs of dependence to anyone with whom they have a close personal relationship.1 Although in most states and territories in Australia there is no legislation that specifically prohibits prescribing for family and friends, South Australia prohibits the prescription of Schedule 8 drugs for family members, except in a verifiable emergency.
In the above case, Dr Smith was heavily criticised for inappropriately prescribing medication to her partner, including morphine, pethidine, other injectable pain relief and psychotropic medications. Not only did she prescribe the medication without specialist advice, she acted contrary to specialist advice when it was provided to her. Dr Smith was found to have failed to recognise Mr Wilson’s drug dependence and to have prescribed the medication without the proper authority.
It is important to consider carefully before prescribing for family and friends. This applies to even seemingly ‘simple’ prescriptions. There may be significant risks of harm to the patient, especially if the prescription is provided without the appropriate assessment and follow up. Any doctor who prescribes without assessment and follow up may be asked to explain and justify their conduct before a disciplinary body.
Damage to personal relationships
Circumstances may arise where the doctor-patient relationship breaks down, and the personal relationship can make it difficult for either party to address this. The decision to terminate the therapeutic relationship can also lead to conflict within family and other relationships. This uncomfortable situation can be avoided by just saying ‘no’ at the outset.
When might it be appropriate to treat family, friends or colleagues?
The Medical Board recognises that there may be situations where practitioners need to treat someone close to them, such as in an emergency or when other medical care is not accessible. For example, in some rural areas, the number of doctors is often limited, and it may be unavoidable to treat friends and family.
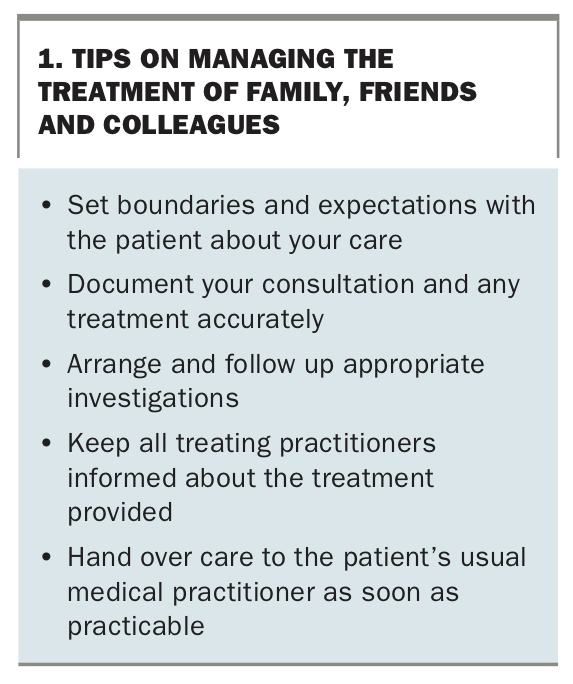
If providing care is unavoidable, ‘good medical practice requires recognition and careful management of [the above] issues’.1 It is important to establish clear boundaries and only provide treatment during a formal consultation. It is also important to document these consultations as you would any other consultation, as well as to include brief notes about the reason that treatment is unavoidable in the circumstances of your personal relationship.
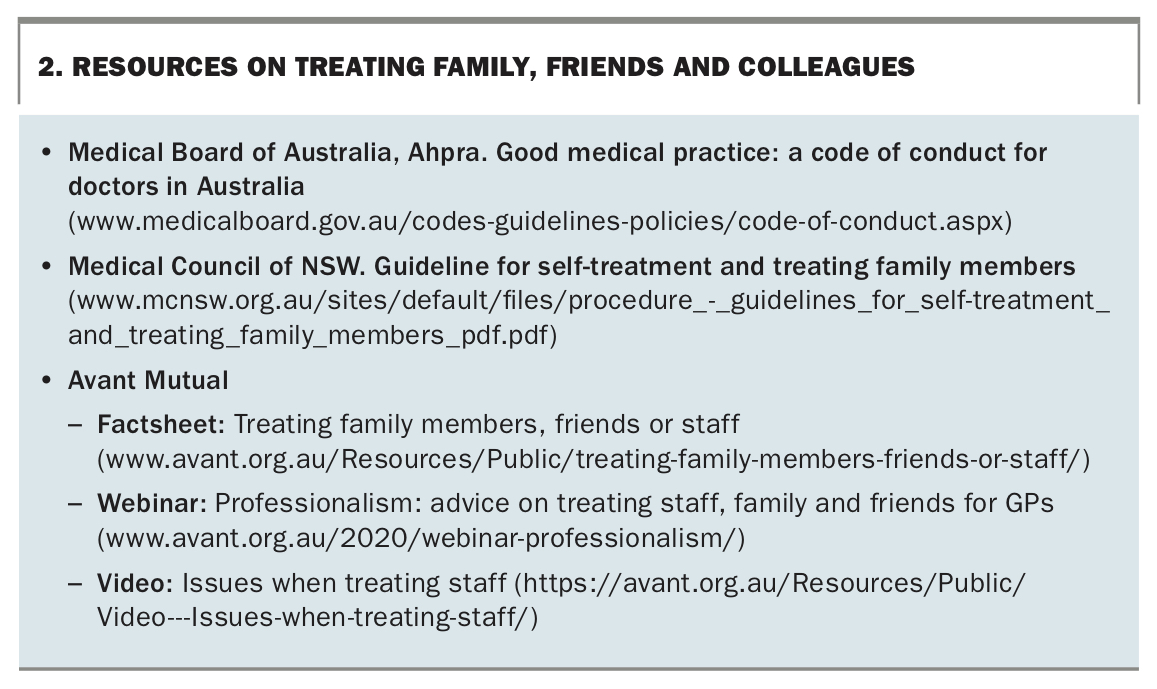
Tips on managing the treatment of family, friends and coworkers are shown in Box 1. Resources for medical practitioners are listed in Box 2.
{kind=link}
{kind=link}
Outcome of the case
The Tribunal finds that Dr Smith’s knowledge, skill and judgement is significantly below the standard reasonably expected of a medical practitioner. The Tribunal also rules that Dr Smith’s conduct constitutes professional misconduct. She is disqualified from being registered as a medical practitioner for a period of 18 months.
Conclusion
Most medical practitioners will be asked for a prescription or opinion by a family member, friend or co-worker at some time. For medical practitioners who practise in isolated or rural communities, their professional and personal lives are likely to intersect. Not every request for a prescription is going to lead to such a complex scenario as the case scenario described above. In emergency settings, you should not hesitate to treat family members or friends until another doctor becomes available.
Outside an emergency, it is important to avoid the situation where you become a primary or regular treating practitioner for someone close to you. If it is unavoidable to provide care in certain circumstances, ensure it is limited and that appropriate handover and documentation occur promptly. This includes providing the relevant information to the patient’s usual treating doctor. MT