Migraine in children and adolescents

Managing chronic headache in children and adolescents can be challenging because of the wide range of differential diagnoses and often high levels of parental anxiety about the cause. A thorough history and awareness of red flags will aid with accurate diagnosis, while effective family counselling and a systematic approach to management enable the best outcomes.
Chronic headache is a common presentation in children, and as many as 30% of adolescents experience recurrent headache.1 It can be a challenging presentation because the yield of investigations is often low, while patient and parental anxiety about aetiology may be extremely high. Rare anecdotes of the child who complained of a headache and was ultimately found to have a brain tumour cause understandable and persistent concerns for many parents.
Diagnostic accuracy and effective patient and family counselling are generally best achieved with a thorough approach to history, awareness of the red flags in paediatric headache, and a systematic approach to management that acknowledges the burden of symptoms while conveying optimism about the outcome. Most prepubescent children, and many adolescents, will find that their migraines decrease over time.
History and examination
The diagnosis of migraine is primarily based on the history. Children will generally complain of a recurrent headache, and those who are able to describe its character will often describe a banging or throbbing sensation. As clinicians attempt to gain a more detailed description of the headache, it is helpful not to lead the child into descriptors. Open-ended questions, such as ‘What does the headache feel like?’, may be better than ‘Is your headache throbbing?’. Although migraine is typically unilateral in adolescents and adults, children are more likely to experience migraine in a bitemporal location. Children often have shorter migraines than adults, with some as brief as one hour in duration. The upper limit of migraine duration may be several days.2
It can be useful to ask how the child behaves when they have a headache. Some children will experience an aura, complain of nausea or become extremely pale. Although a child with a mild headache may watch a movie or play on their computer, children with migraines, who are often affected by photophobia and phonophobia, tend to seek a quiet and dark place with minimal stimulation. Parents will frequently say that the child goes to their room with the blinds closed. Resolution with sleep is another supportive feature of migraine.
One of the challenging factors in diagnosing recurrent headaches in children is the broad array of differential diagnoses, including the commonly occurring tension headache. Most secondary causes of headaches can be excluded on the basis of history. Common causes of chronic or recurrent secondary headaches include recurrent viral illness and local infections, such as otitis media or sinusitis. However, the latter tends to be overattributed to headache and should not be diagnosed unless there is a strong overall clinical impression or purulent secretions in the middle meatus.3 A space-occupying lesion is the sinister diagnosis most feared by parents. Vasculitis, other autoimmune conditions, hydrocephalus and idiopathic intracranial hypertension are other diagnoses to consider.
Most of the differential diagnoses can be discounted based on a thorough history. The positive signs of migraine are a temporal or bitemporal throbbing, possibly preceded by an aura, often associated with phonophobia, photophobia and nausea and resolved with sleep; however, not all patients present with this clear list. Family history can be a helpful diagnostic marker, as about 75% of patients with true migraine have a relative with migraine.
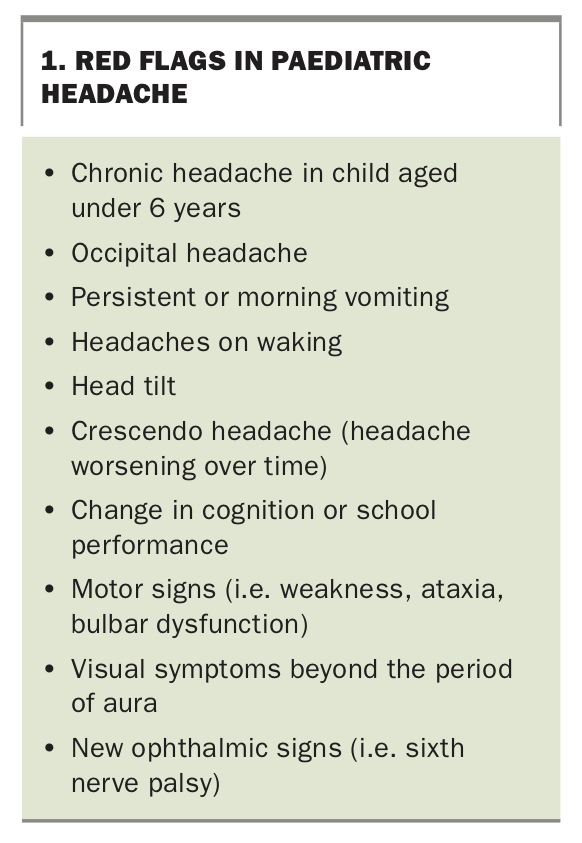
Red flags that should prompt further investigation include headaches that are present on waking or that wake a child from sleep (Box 1). Migraines in a child who has not previously had them, or whose headaches have changed in character or severity, should also prompt careful assessment. Occipital headaches, headaches that worsen over time, headaches accompanied by early-morning vomiting and chronic headaches before 6 years of age warrant cautious evaluation.4
{kind=link}
Headaches associated with confusion or a decline in school performance should be carefully assessed. New motor symptoms – such as weakness, inco-ordination or swallowing difficulties – or ophthalmological changes warrant consideration of imaging, as should a head tilt, which is one of the most common presenting signs of a space-occupying lesion.
The other aspect of history that is usually important is the child’s broader psychosocial context. This is important in ascertaining both the impact of stress as a factor in the child’s headache and the impact of the chronic headache on the child. As with most paediatric presentations, symptoms causing frequent absences from school or other activities require intervention.
In the acute setting, evaluation of headache requires an observation of the child’s pain and mental state, assessment of vital signs (including blood pressure) and a detailed neurological and systemic investigation. Most primary carers and paediatricians review patients with headache in the nonacute setting. The patient with migraine should have an essentially normal examination. Aspects to include are head circumference and blood pressure measurement. Visual acuity and visual fields should be checked, and fundoscopy should exclude papilloedema. Cranial nerves should be normal, and the patient’s tone, power, reflexes and co-ordination should be symmetrical and within normal limits. Gait and cerebellar examinations should be performed.
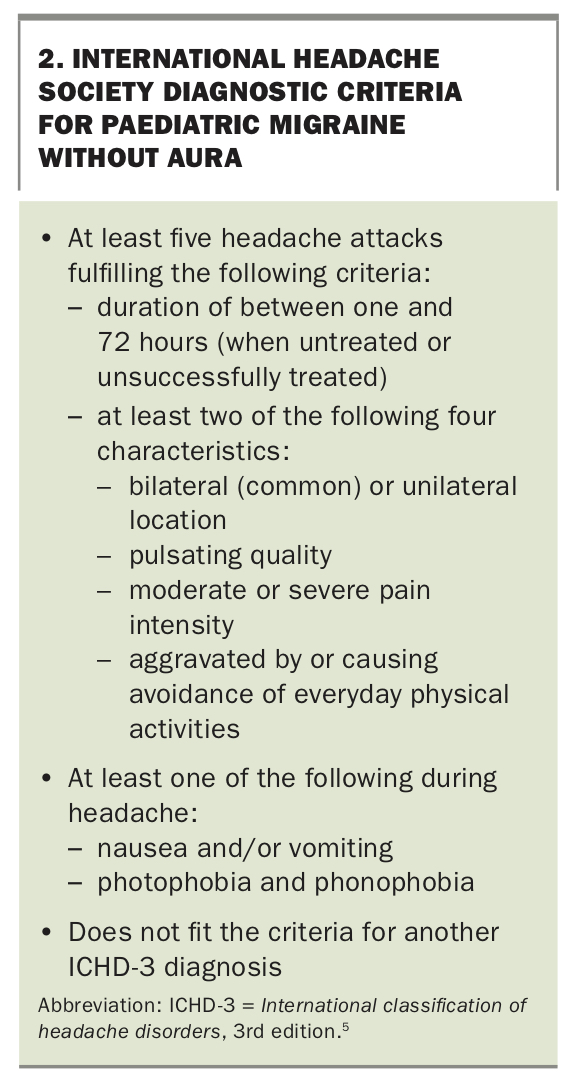
The International Headache Society provides clear criteria for the diagnosis of migraine (Box 2).5 When the patient’s symptoms are consistent with these criteria, the diagnosis is typically straightforward. Other patients present with several features without clearly satisfying all criteria. Provided the red flags for sinister causes have been exhausted, it is often reasonable to diagnose these patients with a migraine variant and adopt a migraine management approach. However, the threshold for investigations tends to decrease when there is diagnostic uncertainty.
{kind=link}
Investigations
Patients who clearly satisfy the International Headache Society criteria for migraines and who do not present with red flags do not routinely require further investigations. However, when there is diagnostic doubt, or in the presence of red flags, MRI of the brain, with magnetic resonance angiography and magnetic resonance venography to examine cerebral vasculature, may be indicated.
Sometimes the level of parental anxiety is such that medical imaging becomes important to show a lack of sinister abnormalities and to engage the patient and family in the patient’s longer-term management. Patients who are undergoing neuroimaging primarily for reassurance should be counselled as to the likelihood of incidental findings, such as the 5% chance of finding an incidental arachnoid cyst, as this is more easily communicated before an abnormal scan generates anxiety.
Blood tests are not usually required for patients with migraine symptoms. However, routine serological testing, including full blood count, electrolyte levels, vitamin B12 levels, iron levels and thyroid function, is often performed to look for contributing factors to fatigue and chronic pain. If there are atypical features to the headache, especially when there is a strong family history of autoimmune disease, autoimmune serological testing (including antinuclear antibodies [ANA], extractable nuclear antigen antibodies, antineutrophil cytoplasmic antibodies, double-stranded DNA, C-reactive protein and erythrocyte sedimentation rate) may be indicated to look for uncommon inflammatory causes of headache. However, many adolescents, particularly young women, will have mildly raised ANA titres without obvious cause, and performing such serological testing without an indication may simply confound the clinical picture.
Patients with signs of raised intracranial pressure (headaches or vomiting on waking, diplopia or papilloedema) who have normal imaging should be referred for a lumbar puncture with opening pressure to investigate for the possibility of idiopathic intracranial hypertension.
Management
Nonpharmacological management
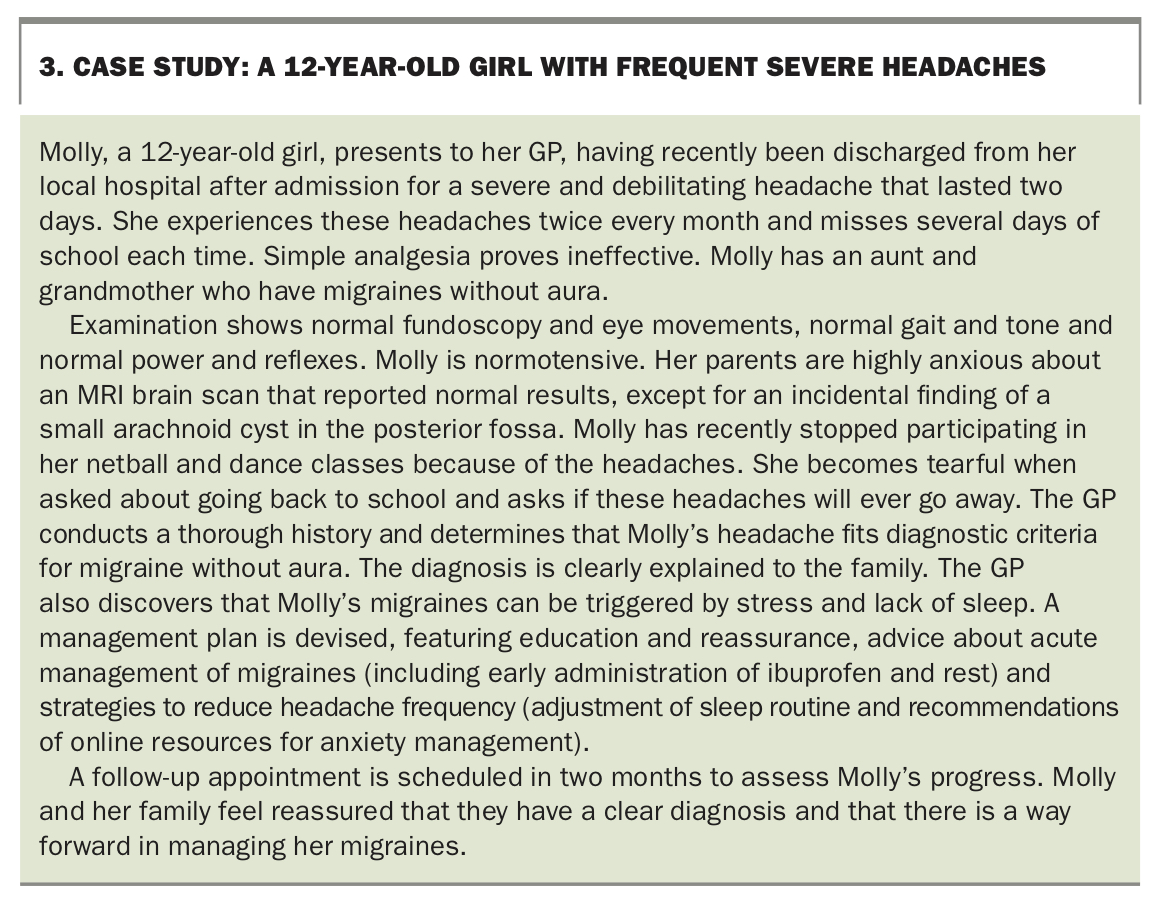
One of the priorities in managing young patients with migraine is providing reassurance and alleviating anxiety among their families. This can be achieved by showing that a thorough clinical history and examination have been done and offering a clear diagnosis of migraine (see case study in Box 3). It can be useful to reiterate the common prevalence of migraine in children and adolescents (about 10% in school-aged children and 20% in adolescents) and to explicitly counsel families that migraines do not herald sinister causes.1,2
{kind=link}
A headache management plan can be useful for people with migraine, covering nonpharmacological strategies (including awareness of triggers), acute headache treatment and, when indicated, preventive medication.
About half of children with migraine will have clear precipitants. Triggers may include physical exercise, heat, fatigue or specific foods. It may be advisable for patients to keep a headache diary to notice patterns related to possible precipitating factors. When there is an obvious trigger, avoidance, if practical, can be beneficial. Strict nontargeted elimination diets often add unnecessary stress and are seldom effective.
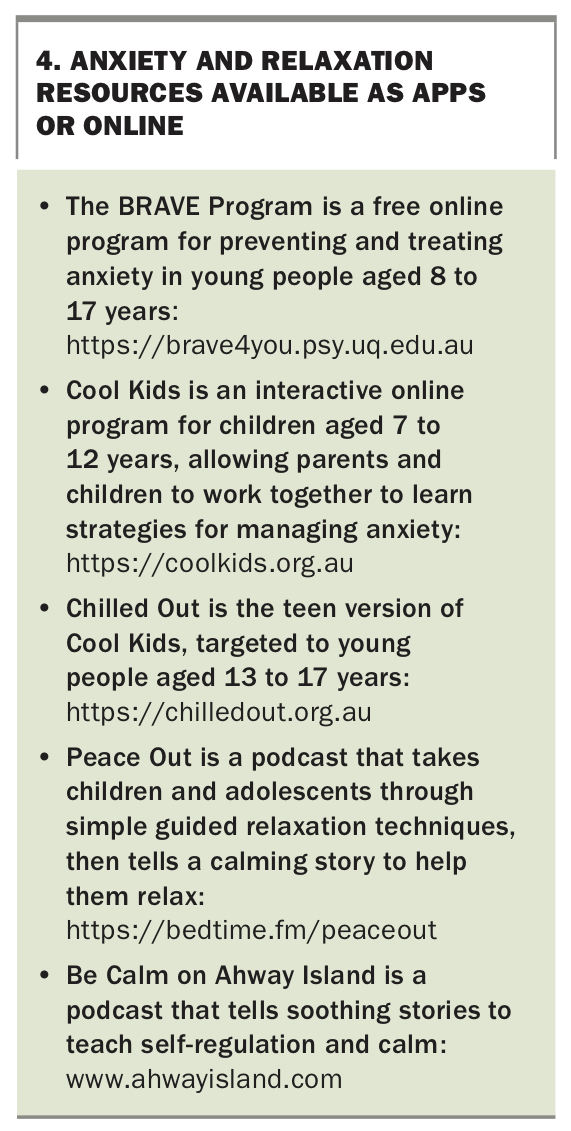
Good sleep hygiene is a sensible recommendation, as is general adherence to a balanced diet and regular physical activity. For many children and particularly adolescents with migraine, emotional stress is an important factor. Discussing the child’s propensity to worry and communicating the common association between migraine and anxiety can be useful. There are several online resources and podcasts that teach mindfulness and meditation or provide strategies to aid in regulating anxiety (Box 4). On a practical level, it can be helpful to discuss the child or adolescent’s weekly schedule, as they may be stretched across several hours of extracurricular activity, and to acknowledge the importance of rest. Conversely, a gentle rehabilitation approach may be necessary for patients who have ceased all regular activity and school attendance because of their migraines. When anxiety is more impairing or plays a greater role in their migraines, referral to a psychologist for anxiety regulation and chronic pain management can be beneficial.
{kind=link}
Families often ask about complementary therapy approaches, including acupuncture. There is a lack of robust scientific evidence for these, but there are anecdotal reports of patients benefiting from complementary therapies. Given the lack of evidence for their efficacy, it is worth advising families not to invest in approaches that cause significant financial or practical stress. If chiropractic treatment is considered, cervical spine manipulation should not be attempted in children. Tension headaches that may have a muscular component (generating from the neck) can respond to massage and adjustments in posture.
Pharmacological management
Administration of an NSAID at the onset of headache or aura, rather than waiting for the more severe headache, can be effective. Patients should be encouraged to rest in a dark and quiet environment. Many patients find that sleep is the most effective treatment.
For severe acute migraines that do not respond to NSAIDs, triptans may be effective. One of the most prescribed triptans is sumatriptan, which can be administered orally or intranasally. This is best administered early in the migraine onset, and the dose can be repeated two hours later if found to be partially effective.
Before determining whether an acute treatment is effective, it should be administered in at least two discrete migraine episodes.6 It is not generally recommended to use acute symptomatic treatments more than twice a week, and migraines requiring more than two acute treatments on a weekly basis should suggest a prophylactic approach. There are different schools of thought as to the frequency of migraines that warrant prophylactic treatment; however, in general, children experiencing migraines that are having a significant impact on their life may benefit from prophylactic treatment. From the outset, it is important to counsel patients and their families that prophylaxis will often not result in complete resolution of the migraines, but that the aim is to reduce the frequency and severity of the attacks.
Riboflavin (vitamin B2) has been shown in some studies to be effective in preventing migraine, and the recommended dose is 400 mg daily.7 A second-line therapy is the beta blocker propranolol, although this is relatively contraindicated in children with asthma. Blood pressure should be monitored in patients taking propranolol.
Third-line options include antiepileptic medications, such as topiramate. Side effects include decreased appetite and increased sweating, resulting in a reduced threshold of dehydration, such that additional hydration, especially in warm weather, is recommended. Amitriptyline is most likely to be effective in patients whose migraine overlaps with tension headache or chronic persistent daily headache.
Challenging types of migraines
Migraines are, by definition, episodic in nature, but some patients report migraine-type headaches in a constant or daily pattern. This description may represent a transformed migraine, in which patients who typically have a history of migraine find that their headache has transformed to a chronic daily headache. Once the diagnosis of transformed migraine is established, the management approach is generally consistent with that for general migraines.
As outlined above, acute medications, including triptans and analgesics, should be limited to twice-weekly use to avoid medication overuse. Overuse of medication can result in medication overuse headaches, and a detailed history of analgesic usage is important in recognising this complication. An emphasis on nonpharmacological approaches, explicit indications for analgesia and a maximum frequency of use may be required, as well as withdrawal of the overused medication.
Most migraines can be managed in the primary care setting, but those occurring in young children (aged under 6 years) or very refractory migraines may require referral to a paediatrician or paediatric neurologist. Complicated forms of migraines, including hemiplegic or confusional migraines, should also prompt specialist opinion. When there is diagnostic doubt or significant familial anxiety, referral can be beneficial. Finally, children with significant school absenteeism resulting from migraine or chronic headache should also be referred to a specialist to deal with any contributing factors and reformulate a management plan.
Conclusion
The chronic and disruptive nature of migraines can cause frustration for patients and their families. This can, in part, be alleviated by a clear and thorough discussion at the time of diagnosis to clarify expectations. The approach to managing migraine will be slightly different for each patient and it may require a trial of more than one prophylactic agent. Few patients, if any, will find their migraines are entirely cured with one prescription. However, with a systematic approach to management that includes both pharmacological and nonpharmacological aspects, most patients will experience a reduction in their symptoms over time. MT