Folliculitis: diagnosis and management of subtypes

Folliculitis is a common disorder, although the exact prevalence is unknown. It presents as erythematous pustules surrounding hair follicles. It may be due to a superficial or deep infection of the follicle, or may be secondary to trauma. Deeper infections present as sycosis and folliculitis decalvans. Good grooming and hygiene are key to treatment and long-term resolution, alongside pharmacological therapies.
- Folliculitis is characterised by inflammation of the hair follicle, with formation of a pustule.
- Superficial folliculitis may arise from mechanical or chemical irritants, such as during hair removal and grooming, or infection with Staphylococcus aureus. It is usually self-limiting and requires little pharmacological intervention.
- However, deeper infections can result in more persistent and recurrent subtypes of folliculitis such as sycosis or folliculitis decalvans.
- The mainstays of treatment are hygiene and grooming, alongside antibiotics or antifungals depending on the causative agent and subtype.
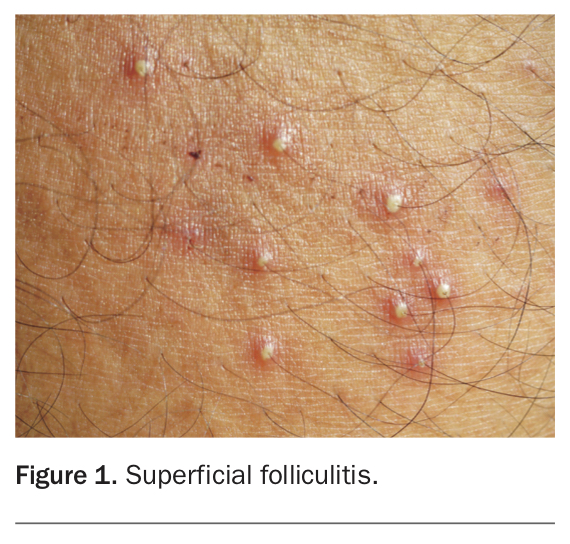
Folliculitis is characterised by inflammation of the hair follicle.1 The result is a tender red papule or nodule, often with a surface pustule (Figure 1) that may be superficial or deep, which may occur in any location where there is a hair follicle.1 The exact incidence of folliculitis is unknown as most patients do not seek medical attention. However, superficial folliculitis caused by Staphylococcus aureus is most common in childhood and usually occurs on the scalp or limbs.2
{kind=link}
Pathophysiology
Superficial folliculitis is not always primarily infective in origin. Physical or chemical injury to the skin can cause folliculitis, which results in the formation of sterile pustules or papules that contain coagulase-negative staphylococci. S. aureus superficial folliculitis is an infection of the follicular ostium.1
Occupational contact with mineral oils or tar products can cause folliculitis. A traumatic folliculitis may develop after epilation, and a sterile folliculitis may develop beneath adhesive dressings.1,3 Other forms of folliculitis are triggered by medications or underlying disease, with a postulated mechanism of a hypersensitivity reaction.
Presentation and prognosis
Follicular lesions present as papules or pustules, and more persistent lesions can occur on the thighs and buttocks of adolescent males.2 Pustules develop in crops and heal within seven to 10 days, but can become more chronic. Deeper infections may develop as furuncles or sycosis. Recurrent or chronic staphylococcal folliculitis may develop into folliculitis decalvans. Patients who come into close contact with other people may spread the condition, for example athletes competing in team sports, military personnel and prisoners.4
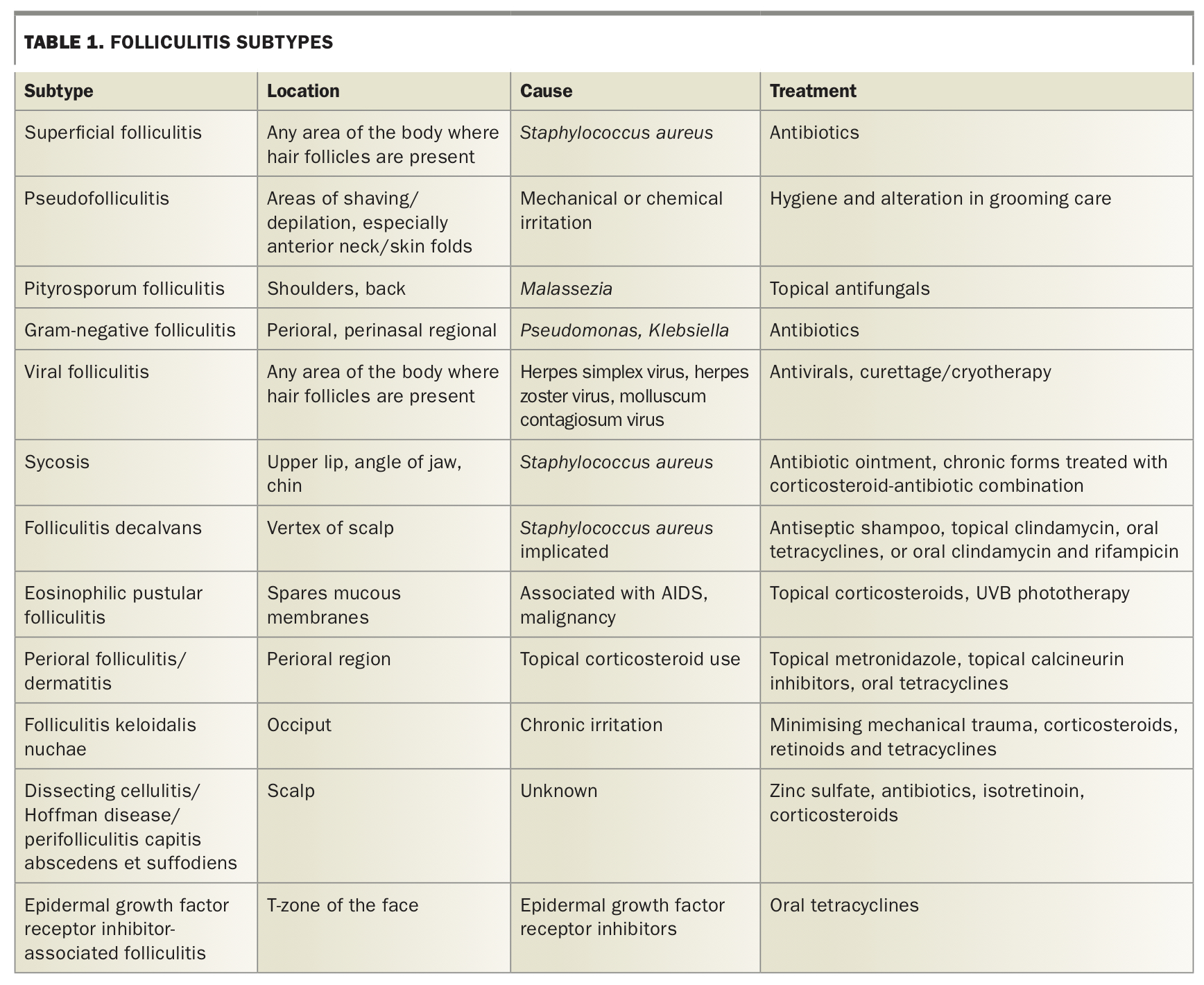
Folliculitis is usually self-limiting and settles within a few days. However, some folliculitis subtypes can be recurrent and persistent, as will be discussed in more depth below and summarised in Table 1.1
{kind=link}
Differential diagnosis
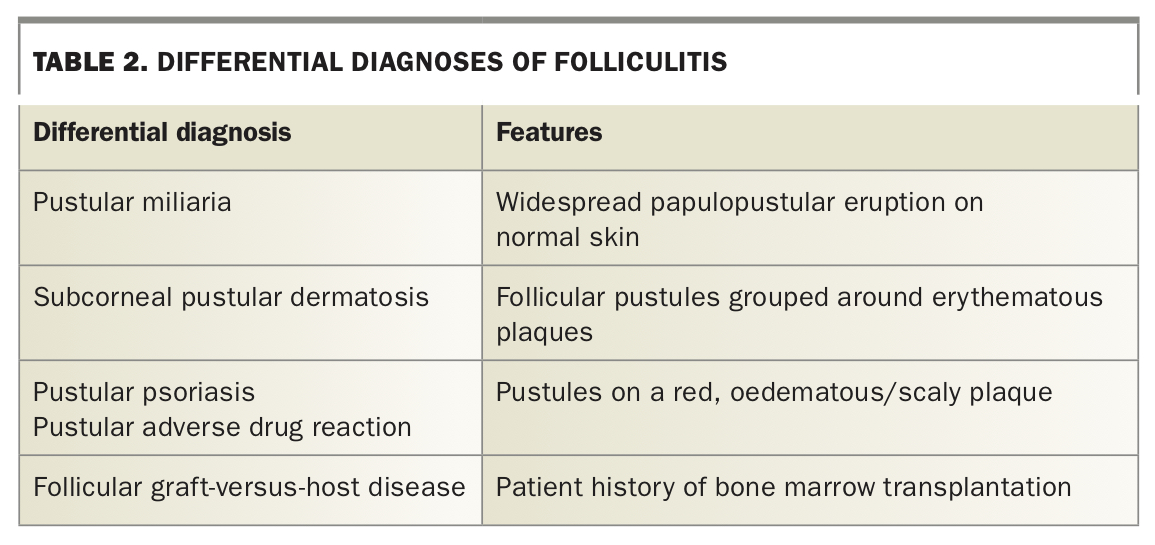
Differential diagnoses are summarised in Table 2. Pustular miliaria presents as a widespread papulopustular eruption on normal skin in hot and humid conditions and may be confused with folliculitis.
{kind=link}
Subcorneal pustular dermatosis develops as follicular pustules grouped around the margins of plaques of erythema and scaling.
Pustular psoriasis or a pustular adverse reaction to medications (such as to epidermal growth factor receptor inhibitors) presents as pustules on a circumscribed red and oedematous or scaling plaque. Follicular graft-versus-host disease can be considered in the context of bone marrow transplantation.
Investigations and management
Investigations are usually not required, although swabs can be taken to assess sensitivity of the causative organism. Most cases of folliculitis can be managed through avoidance of irritants and good hygiene; however, some patients may also benefit from pharmacological treatment. Superficial folliculitis of chemical or physical origin will settle with removal of the irritant. Mild staphylococcal folliculitis is usually self-limiting and may respond to topical antiseptics or cleansing.1 Hand washing and hygiene are critical in preventing transmission of community-acquired methicillin-resistant S. aureus infections.1
Subtypes
Pityrosporum folliculitis
Also known as Malassezia folliculitis, pityrosporum folliculitis results from the growth of the yeast Malassezia within hair follicles and is the most common cause of fungal folliculitis.5,6 It presents as an itchy monomorphic acneiform eruption with many papules or pustules (Figure 2).5 Sometimes the rash will settle in a matter of days, but usually it will become chronic unless treated.6 There is a predisposition to Malassezia folliculitis in adolescence due to increased activity of sebaceous glands. The rash is distributed over the shoulders, neck and back. Diagnosis can be confirmed via a potassium hydroxide stain.6 Treatment with topical antifungals is helpful.5,7 Some patients require oral antiyeast agents to settle inflammation.6,7 In this setting itraconazole works well.7
{kind=link}
Viral folliculitis
This subtype is most commonly caused by the herpes viruses (simplex and zoster), but may also be triggered by the pox virus molluscum contagiosum.6 A clinical clue to a viral cause of folliculitis is the presence of papulovesicles or plaques rather than pustules. Another clue is that lesions appear in clusters and are often preceded by a burning sensation.6 Molluscum contagiosum-induced folliculitis more commonly occurs on the face, and is often preceded by hair removal or shaving.6
Treatment is via oral aciclovir, valaciclovir and famciclovir.6 Molluscum contagiosum-induced folliculitis can be treated with curettage or cryotherapy, although it often resolves spontaneously.6
Gram-negative folliculitis
Gram-negative folliculitis has the moniker of ‘hot tub folliculitis’ as it infamously arises from the bacteria Pseudomonas aeruginosa after exposure to an improperly treated swimming pool or hot tub.6,8 Other implicated organisms include Klebsiella, Proteus, Citrobacter and Enterobacter species, as well as Escherichia coli.6 Patients taking long-term oral antibiotics that inhibit Gram-positive organisms, such as for the treatment of acne, are predisposed to this folliculitis.1,9
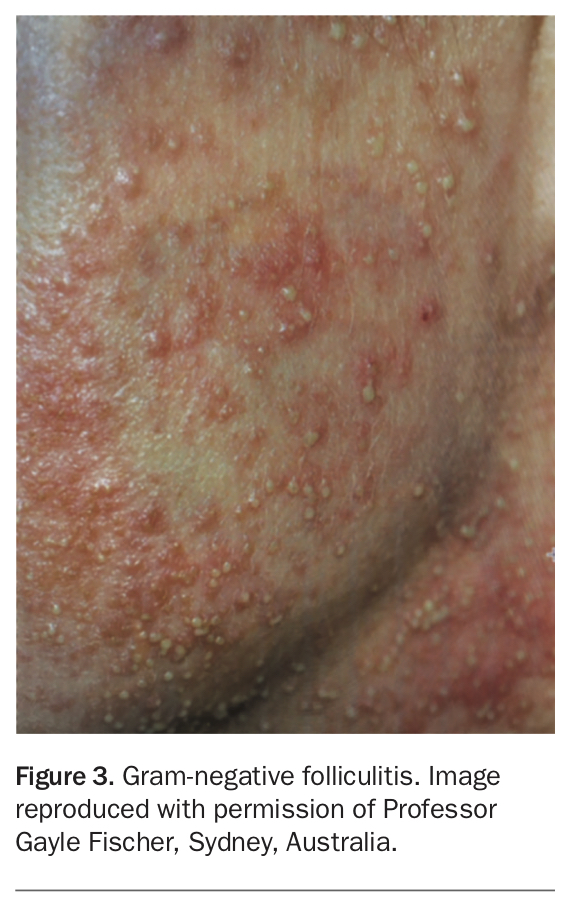
Clinically, an eruption of multiple small follicular pustules localised to the perioral or perinasal skin occurs (Figure 3), and sometimes these appear on the trunk, mimicking pityrosporum folliculitis.1,9 Antibiotics that target Gram-negative organisms may clear the folliculitis over a few weeks. Isotretinoin can be used in cases of recalcitrant Gram-negative folliculitis, especially in patients with acne or rosacea, and has a lower relapse rate than other treatment options.7,10
{kind=link}
Pseudofolliculitis
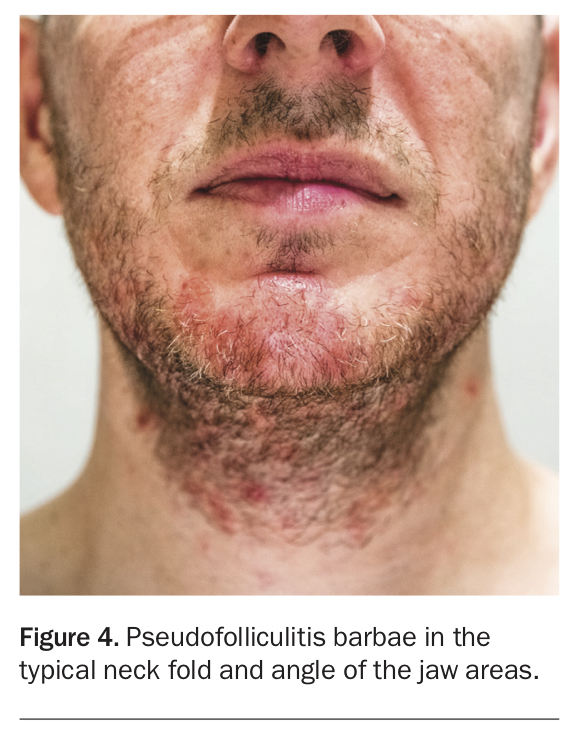
Pseudofolliculitis is a foreign-body inflammatory follicular and perifollicular reaction.1,11,12 The described process is of curved hair emerging from the skin surface and then re-entering the skin to form an in-growing hair (extra-follicular penetration).11,12 Alternatively, closely shaven hair may retract into the hair follicle and then grow into the sides of the follicle (transfollicular penetration).11,12 Pseudofolliculitis more commonly occurs in people with curly hair and those with Asian and African ancestry.1,11,12 A genetic defect (a single nucleotide substitution in the hair follicle companion layer-specific keratin gene K6hf) has also been implicated, with these patients having six times the risk of developing this condition.11,12
It presents as multiple small papules and pustules on shaven skin (Figure 4). It classically affects the beard area (pseudofolliculitis barbae), especially the neck, which may scar with keloid formation and hyperpigmentation, as well as the lower legs and groin.1,11,12 Differential diagnoses include bacterial folliculitis such as sycosis barbae and dermatophytosis.
{kind=link}
Pseudofolliculitis tends to be a chronic condition with a relapsing and remitting course. Stopping shaving for four to six weeks allows inflammation to settle; however, resumption of shaving or waxing will often lead to relapse. Alternative methods of grooming to avoid pseudofolliculitis include shaving or clipping hair to a length of 1mm, or performing hair removal with chemical depilatories or lasers.11 Chemical depilatories lyse the disulfide bonds in the hair shaft, thus weakening them and making them less likely to cause extra or transfollicular penetration and thus a foreign-body reaction.11 Other treatments include topical and oral antibiotics, topical retinoids, chemical peels and electrolysis.12 The mainstay of treatment traditionally is either to shave the affected area with preshave hair hydration sufficiently close to the skin to prevent extrafollicular penetration and use postshave moisturisation, or to allow the hair to grow out.12
Sycosis
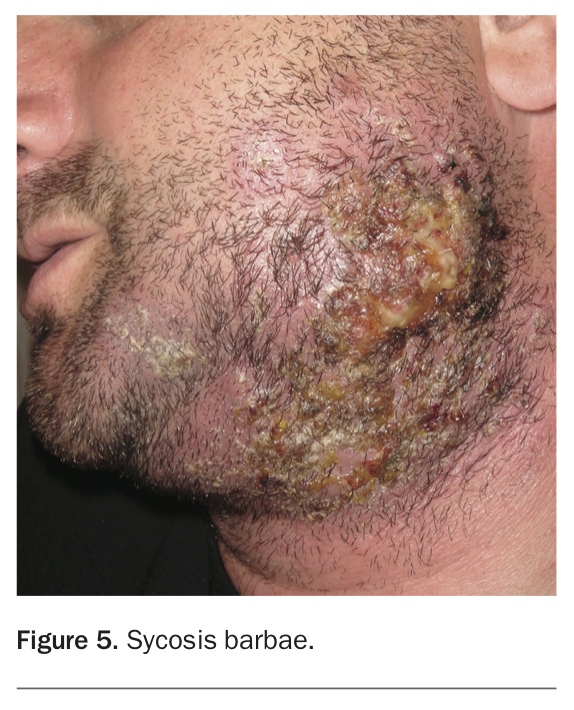
Sycosis is a subacute or chronic pyogenic infection involving the whole depth of the follicle.1 It most commonly affects men in the third or fourth decade of life and usually refers to disease in the beard area (sycosis barbae). The most common infecting organism is S. aureus, although infection with other Gram-positive or Gram-negative bacteria (including Treponema pallidum, which causes syphilis), as well as fungi, yeasts, parasites and viruses have been reported.13 Indoor workers are affected more often than outdoor workers.
The affected follicle is packed with polymorphonuclear leukocytes that infiltrate the follicular wall. Around the follicle is chronic granulomatous infiltrate in which lymphocytes, plasma cells, histiocytes and foreign-body giant cells aggregate. The sebaceous gland or whole follicle may be destroyed and replaced by scar tissue.2
The primary lesion is an oedematous erythematous follicular papule or pustule centred on a hair. If neighbouring follicles are involved, the perifollicular oedema may coalesce to produce raised plaques studded with pustules (Figure 5). In subacute forms, the lesions are grouped or scattered around the upper lip and below the angles of the jaw. Chronic lesions cluster into plaques, especially on the upper lip and chin. There is often some crusting and scaling but the hairs are retained and there is no evident scarring.2
{kind=link}
In lupoid sycosis, the follicles are destroyed by scarring and are surrounded by active papules and pustules. Granulomatous inflammatory changes give the papules a lupoid appearance. Lupoid sycosis tends to begin under one ear or under the chin and extend irregularly in any direction. It may extensively involve the scalp. Lupoid sycosis tends to persist indefinitely.2
Differential diagnoses include pseudofolliculitis, although pseudofolliculitis tends to be irregularly scattered over the neck and angles of the jaw and within skin folds. Tinea barbae usually occurs on the chin, mandible or upper lip as an oedematous plaque of grouped pustules.
Bacterial swabs may confirm the presence of S. aureus and treatment with antibiotic ointments is typically effective. Chronic forms of sycosis may require a combination of corticosteroids and systemic antibiotics. Other treatment includes fractional radiofrequency microneedle treatment.13
Folliculitis decalvans
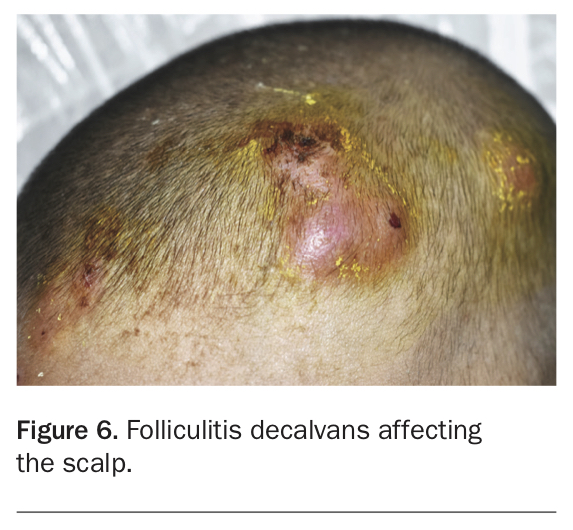
Although uncommon, folliculitis decalvans is the most common form of neutrophilic scarring alopecia.14 It causes painful, recurrent exudative folliculitis that most commonly involves the vertex of the scalp.14,15 Its pathogenesis is not fully understood, although S. aureus has been isolated from the pustules.15,16 The folliculitis penetrates more deeply within the follicle and produces a scarring alopecia that spreads to neighbouring follicles.15
Early onset is associated with a more severe form of the disease.16 Folliculitis decalvans initially presents as painful follicular pustules that become crusted (Figure 6). Tufted hairs are also identified (more than five hairs exiting from the same follicular opening). It expands outwards with a central area of scarring.15,16 Men are affected from adolescence onwards and women from their thirties.
{kind=link}
Treatment is mainly aimed at eradicating S. aureus. Antiseptic shampoos and topical clindamycin are sufficient to treat mild cases. One systematic review of the efficacy of folliculitis decalvans treatments across 20 studies suggested that the most commonly used treatment is a 10-week course of clindamycin and rifampicin.14 There is some evidence, however, that maximal treatment effect is obtained through rifampicin and clindamycin, tetracyclines and intralesional corticosteroids, although individual clinician treatment choices vary widely.14,16 Some patients require long-term treatment with oral tetracyclines to control this disease.17
Eosinophilic pustular folliculitis
Eosinophilic pustular folliculitis was first described in the 1960s as a case of a woman with recurrent follicular pustules on her face and back, with a peripheral eosinophilia noted on her blood test results and an infiltrate of eosinophils on histology.18 A syndrome was later defined as pruritic sterile follicular papulopustules with central clearing and peripheral extension and resolution, with residual pigmentation followed by recurrence.18 The syndrome was also required to be chronic, have an absence of systemic symptoms, and spare the hands, feet and mucous membranes.18 However, subsequent data suggested that around 20% of cases involve the hands and feet.18 Associated diseases include AIDS and malignancy (lymphoma, leukaemia and naevoid basal cell carcinoma syndrome).18 However, some researchers advocate for AIDS-associated folliculitis to be considered a distinct entity.
Eosinophilic pustular folliculitis tends to affect males more than females (4.8:1), with a peak incidence in the third and fourth decades of life. The pathogenesis is thought to relate to an aberrant T helper-2-type immune response to follicular antigens such as contact dermatitis, infections or medications.18
There is no strong evidence for any single treatment type, but typical first-line therapy is topical corticosteroids.18 The optimal treatment might be UVB phototherapy with no reported treatment failures.18 Other treatments include indomethacin, itraconazole, metronidazole, topical calcineurin inhibitors and oral antihistamines.18 In cases where HIV AIDS is implicated, antiretroviral therapy has been noted to improve the associated folliculitis.
Perioral dermatitis
A perioral folliculitis or dermatitis is primarily induced by topical corticosteroids.19,20 Other causes include infections, toothpaste and cosmetic preparations.20 Perioral dermatitis presents with crops of pruritic, erythematous papules that are usually grouped around the mouth, but can also occur around the eyes and nostrils.
Topical corticosteroids will initially control the disease, with rebound disease when the corticosteroid is ceased. Thus, treatment with corticosteroids should be avoided. Long-term corticosteroid use will result in more severe perioral dermatitis.19,20
This condition can be managed through anti-inflammatory antibiotics including topical metronidazole, erythromycin or clindamycin, topical sulfur preparations, or azelaic acid gel.19,20 Topical calcineurin inhibitors including tacrolimus ointment or pimecrolimus cream have also been used.19,20 Oral tetracyclines can be used in more moderate and severe disease and taken for up to two to three months.20 The important point to remember is that although topical corticosteroids provide initial benefit, they lead to rebound flaring and worsening of disease.
Folliculitis keloidalis nuchae
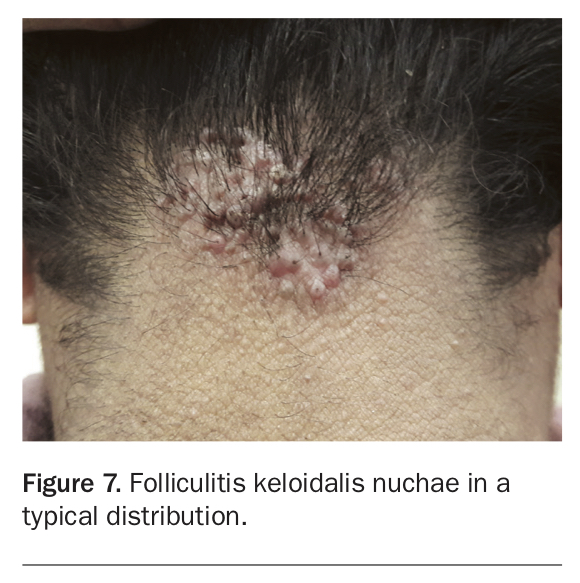
Folliculitis keloidalis nuchae, also known as acne keloidalis nuchae, is a chronic inflammatory condition that leads to fibrotic plaques and alopecia over the occiput.21,22 It is worth noting that, although the term ‘keloidalis’ is used to describe the condition, there are no keloids associated with it and affected individuals do not have a greater chance of developing keloids.22 It is also worth noting that the term ‘acne keloidalis nuchae’ is sometimes preferred, as the condition can extend beyond the occipital area.22 It is typically seen in postpubertal men of African descent and is rare in women and those aged over 55 years.21,22 The cause is unknown but is thought to be an aberrant immune response to predisposing factors including androgens, chronic inflammation (such as from shirt collars, helmets and combs), infection, trauma and ingrowing hair.21,22
Folliculitis keloidalis nuchae presents as papules, pustules and tumourous masses in the nuchal or occipital regions of the scalp (Figure 7).21,22 Often these arise within days after a haircut or other irritation. Pruritis, pain and bleeding are associated with active lesions and secondary bacterial infection is common.21,22 Chronic inflammation leads to fibrosis and large plaques and nodules.21
{kind=link}
The overall goal of management is to prevent the development of further lesions and subsequent alopecia. Nonpharmacological measures include avoidance of close shaving, helmets and tight collars.21,22 Haircuts should be avoided when lesions are active and bleed easily, because of the risk of blood-borne disease transmission.21 Antiseptic shampoos may have a role in preventing secondary infections.21,22 Mild disease can be treated with topical corticosteroids and topical retinoids, whereas moderate disease may require intralesional triamcinolone or systemic corticosteroids.21,22 More severe or chronic disease will benefit from long-term oral tetracyclines and retinoids. Surgical excision of affected areas can work well, although recovery time is longer and lesions may recur.21,22 It is thus better used in chronic and refractory disease.21 Ablative laser therapy is an emerging treatment that has been reported to work well in treating folliculitis keloidalis nuchae, although it is typically less available in Australia.21
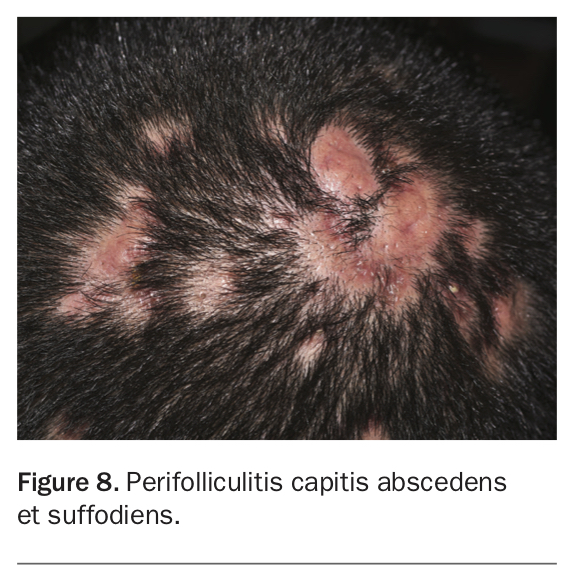
Perifolliculitis capitis abscedens et suffodiens
Also known as dissecting cellulitis or Hoffman disease, this condition presents with perifollicular pustules, nodules, abscesses and sinuses (Figure 8).23 The end result is a scarring alopecia.23 It predominantly affects men of African descent aged 20 to 40 years, and has been associated with arthritis, keratitis, Crohn’s disease, pyoderma gangrenosum and keratitis-ichthyosis-deafness syndrome.23 The aetiology is unknown, although it is classed within the follicular occlusion tetrad, along with acne conglobata, pilonidal cysts and hidradenitis suppurativa.23
{kind=link}
Treatment includes zinc sulfate or isotretinoin in combination with oral antibiotics for three to 12 months. Oral prednisone can be helpful as an adjunctive agent.23 Newer therapies include adalimumab and infliximab, and ablative lasers targeting the hair follicle.23 Surgery can achieve cure, but is not always successful and has higher morbidity than pharmacological treatments.23 Often bacteria can be isolated on culture of the lesions, but targeting them for treatment has an unclear effect on disease resolution.23
Folliculitis secondary to medications
It is well-recognised that certain drugs including protein kinase inhibitors or epidermal growth factor receptor inhibitors (EGFRIs) as well as vemurafenib and dabrafenib for metastatic melanoma, cause a folliculitis. EGFRIs are used for colonic, rectal and pulmonary cancers, and include the monoclonal antibodies cetuximab and panitumumab, and the tyrosine kinase inhibitors erlotinib and gefitinib.24 More than 50% of patients on EGFRI treatment experience a folliculitis, and this is the most common dermatological side effect.24 It tends to occur between one and four weeks after commencement of treatment and then slowly resolves. Exacerbating factors include sun exposure, radiotherapy and xerosis.24 Management is mainly via oral tetracyclines and usually achieves a good result.24 Starting the tetracycline antibiotic before the development of the folliculitis often reduces the incidence and severity.
Conclusion
Folliculitis is a common dermatological disorder that typically involves inflammation of the hair follicle; however, there are numerous subtypes that vary in their aetiology, presentation and prevalence. In most cases of folliculitis, resolution of disease can be achieved through good grooming and hygiene, and treatment with appropriate antibiotic or antifungal agents. MT
COMPETING INTERESTS: None.