Updated anaphylaxis guidelines: a summary for primary care

Anaphylaxis is occurring more frequently in Australia and the rate of fatal reactions is increasing. Prompt recognition and early treatment with intramuscular adrenaline can reduce the risk of death.
- Anaphylaxis is a potentially life-threatening allergic reaction that can affect people of any age, including infants.
- Anaphylactic reactions can be unpredictable and may initially present with mild symptoms.
- Rates of hospital admission for anaphylaxis and fatalities from anaphylaxis are increasing in Australia.
- Adrenaline is the first-line treatment for anaphylaxis and should be given without delay by intramuscular injection into the outer mid-thigh; there are no contraindications for adrenaline in the management of anaphylaxis.
- Correct positioning of a patient with anaphylaxis is essential, as an upright posture is a risk factor for fatal reactions.
- Adrenaline injectors (AIs) allow easy, prompt administration of adrenaline and are designed to be used by people without medical training. There are two AI devices available in Australia on the PBS.
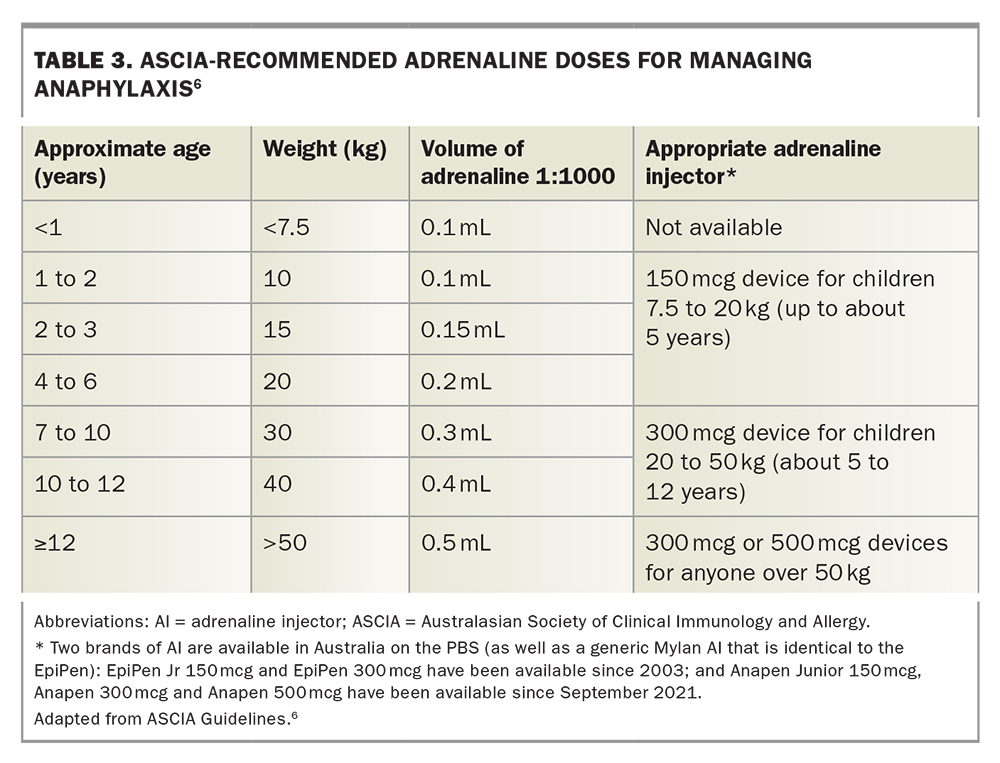
- The Australasian Society of Clinical Immunology and Allergy (ASCIA) now recommends a 150mcg AI can be prescribed for infants weighing from 7.5 to 20kg; children weighing 20kg or more should be prescribed a 300mcg AI, and from around 12 years (if weight greater than 50kg) either a 300mcg or 500mcg AI is recommended.
- ASCIA has recently updated its guidelines for the acute management of anaphylaxis and has also updated its e-learning courses and anaphylaxis resources in line with current evidence.
Anaphylaxis is a potentially life-threatening allergic reaction that can present at any age. Anaphylactic reactions are unpredictable and initial signs of fatal anaphylaxis can be mild.1-4 Allergic reactions defined as anaphylaxis are those that are potentially life threatening and require early treatment with adrenaline to reduce the risk of death.4 Common causes of anaphylaxis include foods, medications and insect venom, but rare causes such as exercise or cold temperatures need to be considered. Although anaphylaxis often has a rapid onset, certain triggers may cause anaphylaxis several hours after allergen exposure, for example galactose-alpha-1,3-galactose (alpha-gal allergy, mammalian meat allergy).5
The rate of anaphylaxis from all causes is increasing in Australia, with anaphylaxis due to foods increasing most. Prompt administration of intramuscular adrenaline is safe and should be first-line treatment for anaphylaxis. Antihistamines and corticosteroids do not treat or prevent anaphylaxis and should not be given before adrenaline. Appropriate management of patients with anaphylaxis includes ensuring they have adequate education about their triggers, how to avoid their allergen and how to recognise and treat anaphylaxis. Some online resources for doctors and patients are recommended in the Box. The Australasian Society of Clinical Immunology and Allergy (ASCIA) has recently updated its guidelines for health professionals for the acute management of anaphylaxis in line with current evidence.
{kind=link}
Presentation and diagnosis
The diagnosis of anaphylaxis is made clinically, thus it is imperative that symptoms and signs are recognised promptly. Definitions of anaphylaxis vary worldwide but ASCIA defines anaphylaxis as:
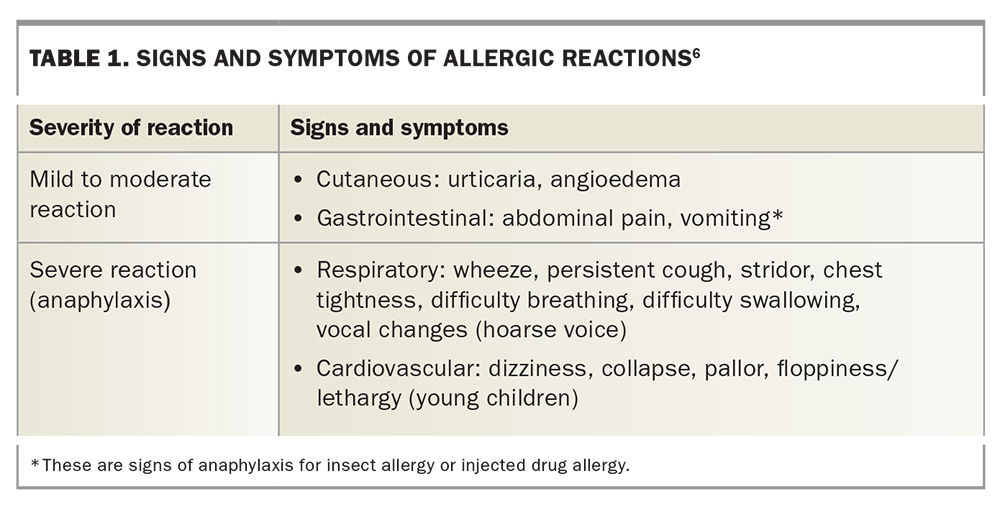
- any acute onset illness with typical skin features (urticarial rash or erythema/flushing, and/or angioedema), plus involvement of respiratory and/or cardiovascular and/or persistent severe gastrointestinal symptoms; or
- any acute onset of hypotension or bronchospasm or upper airway obstruction where anaphylaxis is considered possible, even if typical skin features are not present.6
ASCIA’s definition of anaphylaxis is consistent with criteria recently published in the World Allergy Organization’s anaphylaxis guidance 2020 position paper, which is now included in the updated ASCIA guideline.4 There are controversies regarding some definitions of anaphylaxis. Certain classifications of anaphylaxis require more than one system to be involved, for example skin and respiratory and/or gastrointestinal system involvement; however, some fatal anaphylactic reactions may present with severe involvement of the respiratory or cardiovascular system alone.4
Confusion also arises with how to classify gastrointestinal symptoms such as abdominal pain or vomiting in allergic reactions. Gastrointestinal symptoms of any severity are considered signs of anaphylaxis in allergic reactions to insect stings or injected drugs; however, vomiting and abdominal pain may occur commonly in mild to moderate allergic reactions to foods. Severe, persistent gastrointestinal symptoms may be a feature of anaphylaxis from any cause.6,7 The severity of gastrointestinal symptoms is based on clinical assessment, and if severe they usually respond well to intramuscular (IM) adrenaline.
Respiratory symptoms are more common in paediatric cases of anaphylaxis, and cardiovascular involvement occurs more commonly in adults.8 Anaphylactic reactions may be under-recognised, as up to 20% of reactions occur without cutaneous involvement.4,8 Anaphylaxis may also present solely with subjective symptoms, such as throat tightness, which may not be perceived to be severe.8
Serum tryptase level may be elevated a few hours after anaphylaxis compared with a patient’s baseline and may assist in confirming a diagnosis of anaphylaxis if there is uncertainty or symptoms are atypical.3 Treatment should not be delayed while waiting for tryptase results if anaphylaxis is suspected (Table 1).
{kind=link}
Infants
Anaphylaxis can be difficult to recognise in infants, who cannot verbalise their symptoms and may present with nonspecific signs such as irritability, drooling and sleepiness.9 A high index of suspicion is required as, although uncommon in this age group, fatalities have occurred.10 Tachycardia, which may signal hypotension, can be a sign of anaphylaxis in infants but needs to be interpreted carefully and in context, as other causes of tachycardia may include crying, fever or pain.9 Cardiovascular collapse is rare in infants with anaphylaxis and hypotension is a late sign in infants due to high peripheral vascular resistance and may represent a prearrest sign.9
Pregnancy
Anaphylaxis in pregnancy is rare, with most cases occurring in the intrapartum and postpartum period.11 Common triggers include antibiotics, latex and anaesthetic agents; however, foods and insect venom also need to be considered. In addition to the usual signs and symptoms, anaphylaxis presentation in pregnancy may also include uterine cramps, persistent low blood pressure, lower back pain and fetal distress.11
ASCIA recently published guidelines on the acute management of anaphylaxis in pregnancy.12 Management is similar to that for nonpregnant patients. Adrenaline is the cornerstone of anaphylaxis management in pregnant patients and should not be delayed due to concerns of causing reduced placental perfusion, as benefits of maintaining maternal blood pressure outweigh potential risks.11 The same dose of adrenaline is recommended in pregnant patients (adrenaline [1:1000] 0.01mg/kg IM). An adrenaline injector (AI) 300mcg or 500mcg is a reasonable option to reduce delay in administration if available.
Epidemiology
In Australia, the rate of hospital presentation for anaphylaxis from any cause is increasing. The greatest increase is seen in anaphylaxis to foods, at 10% per year in all age groups between 1997 and 2013, with the most significant rise occurring in older children and adolescents.1
Anaphylaxis fatalities are higher in Australia compared with other countries, and the cause of this is unclear. Anaphylaxis fatalities have been increasing at a rate of 6% per year, with food anaphylaxis deaths increasing at the greatest rate.1 Deaths most commonly occurred due to reactions to medications and stinging insects in men aged over 50 years with comorbidities. Risk factors for fatal anaphylaxis include upright posture after anaphylaxis, delayed administration of adrenaline (epinephrine), concomitant asthma and delayed initiation of cardiopulmonary rescuscitation after collapse.1,13
Triggers
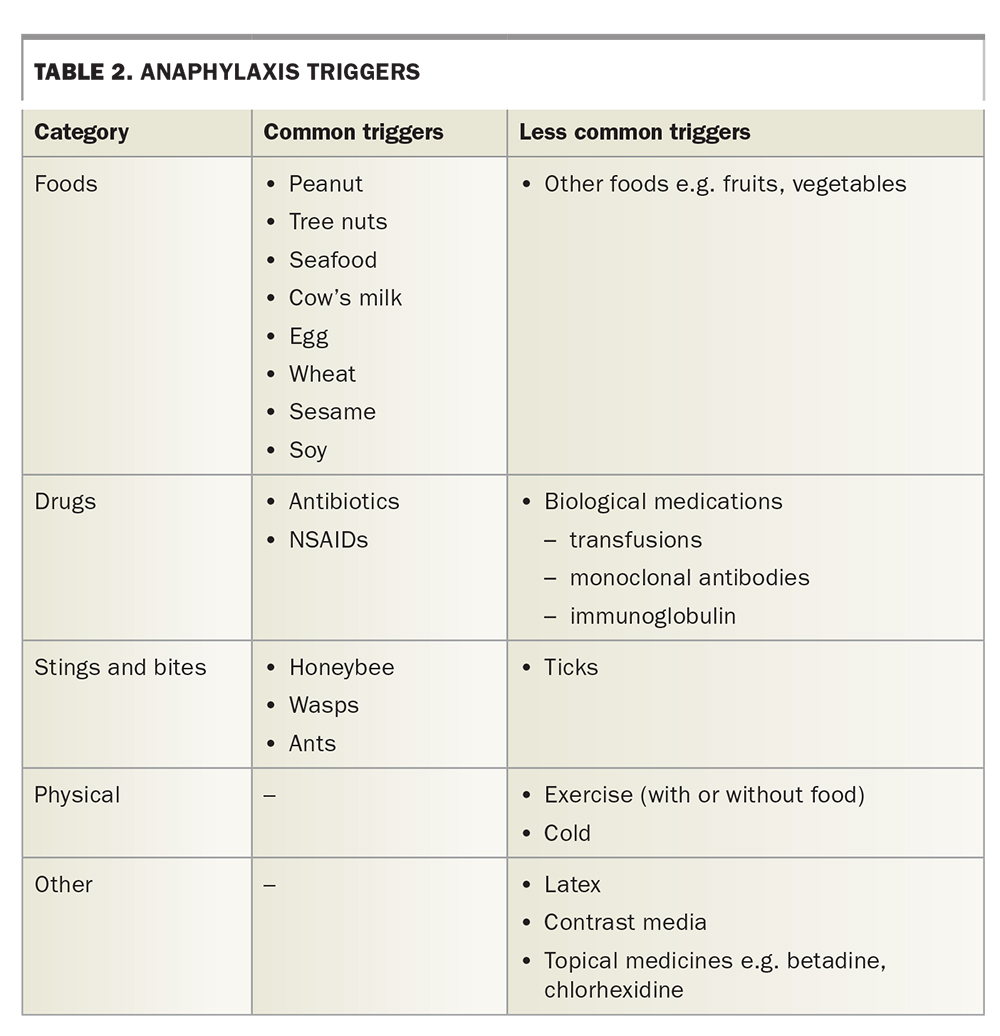
Common causes of anaphylaxis include foods, insect stings and medications (Table 2). Anaphylaxis may also be caused by physical triggers such as exercise or cold exposure. Up to 30% of anaphylaxis cases may be idiopathic, although this is a diagnosis of exclusion and may occur in patients with anaphylaxis to known causes.14 In Australia, hospital admissions for anaphylaxis from all causes are increasing in line with similar trends observed in the US and UK.1,13 In children, food triggers are the most common cause of anaphylaxis, and reactions to peanut, tree nuts, cow’s milk, egg and seafood are responsible for most presentations.15
{kind=link}
In food allergy, anaphylaxis usually occurs within one to two hours of ingestion of the allergen, and the onset may be rapid, often within 30 minutes. Mammalian meat anaphylaxis and food-dependent exercise-induced anaphylaxis are examples of conditions in which symptoms may be delayed several hours after ingesting a food allergen.5,8 Anaphylaxis to animal stings and injected medications, including radiocontrast agents and vaccines, usually occurs within five to 30 minutes but may be delayed.8
The presence of cofactors such as exercise, fever, hormonal status and acute infection may increase the likelihood of an allergic reaction or its severity.8 Alcohol and NSAIDs may potentiate some allergic reactions to foods as well as reduce a person’s capacity to recognise and manage their reaction.1,8 True biphasic reactions are estimated to occur in 3 to 20% of patients at a median of 11 hours after the initial reaction (range 0.5 to 72 hours).3,16
Management
Adrenaline
Adrenaline (epinephrine) is the first-line drug of choice for the acute management of anaphylaxis and should be administered early.3,6,8 There are no contraindications to the administration of IM adrenaline in the treatment of anaphylaxis.8 Adrenaline acts to reduce airway mucosal oedema, induce bronchodilation, induce vasoconstriction and increase cardiac contraction strength.3,8 ASCIA recommends IM adrenaline (1:1000) 0.01mg/kg, up to a maximum of 0.5mg, should be administered without delay into the outer mid-thigh if signs of anaphylaxis are present (Table 3).
{kind=link}
IM adrenaline should be administered early via an adrenaline injector or needle and syringe if there are signs of anaphylaxis. Further doses of IM adrenaline can be given after five minutes if symptoms of anaphylaxis persist or recur.6,8 Owing to an increased risk of adverse effects, boluses of intravenous (IV) adrenaline are not recommended as a first-line treatment for anaphylaxis outside of the operating theatre.3,17,18 Similarly, subcutaneous adrenaline is not recommended, as absorption is not as reliable as IM administration.3,8,19
If symptoms of anaphylaxis persist despite two or more doses of IM adrenaline, an IV infusion of adrenaline can be considered if a health professional with the required skills and equipment is available.3,6,8,20 Cardiopulmonary resuscitation (CPR) should be commenced if despite adrenaline administration the patient is unresponsive and not breathing effectively.1,6,8
Adrenaline injectors
Adrenaline injectors (AIs) allow easy, reliable administration of adrenaline to treat anaphylaxis and are designed to be used by people without medical training. AIs can also be used in medical settings to reduce delays in administering adrenaline. Up to two adrenaline injectors may be prescribed on the PBS for a person considered to be at risk of anaphylaxis. Current prescribing guidelines require a patient to have been discharged from the emergency department or hospital after receiving adrenaline to treat anaphylaxis, or consultation with a clinical immunologist or allergy specialist, paediatrician or respiratory physician. Currently, there are two brands of adrenaline injectors available on the PBS, Anapen (150 mcg, 300 mcg and 500 mcg) and EpiPen (150 mcg and 300 mcg). A generic version from the same manufacturer as EpiPen is also PBS listed (Adrenaline Mylan 150 mcg and 300 mcg).
ASCIA has recently updated its recommendation for AIs for infants and young children in line with expert consensus.3,8,9,21 ASCIA now recommends the AI 150 mcg for infants and young children weighing 7.5 to 20 kg, which was previously only recommended from 10 kg (Table 3). Although using a 150 mcg AI theoretically delivers up to 200% of the recommended adrenaline dose to an infant weighing 7.5 kg, use of the AI reduces delay and dosing errors compared with use of an ampoule and syringe when managing infants with anaphylaxis, and this is considered safe.9,21,22 There is a theoretical risk of bone injury due to AI needles in infants less than 10 kg, but the risk may be reduced by only injecting into the thigh area, bunching the skin and muscle on the thigh before AI use and only holding the AI in place for the recommended time (three seconds for EpiPen, and 10 seconds for Anapen).3,21,23
In the absence of national referral pathways, we suggest that if the patient’s primary care physician believes their patient requires an initial AI prescription, the doctor could contact either their local immunologist or the on-call service at their nearest teaching hospital for further advice.
Practical tips for AI prescribing
Weight recommendations
ASCIA weight recommendations for use of AIs differ from the product information for all sizes of Anapen and EpiPen (Table 3). There are very limited data on efficacy and safety of adrenaline doses in anaphylaxis.21 ASCIA’s recommendations are based on current evidence and expert consensus. The ASCIA weight recommendations for AI reduce the risk of underdosing and have an excellent safety record.
Brand substitution
The Pharmaceutical Benefits Advisory Committee (PBAC) allows brand substitution by pharmacists for AIs for the 150 mcg and 300 mcg devices. Although the PBAC reiterates that different devices should not be prescribed for the same patient without training from the prescriber on a practical level, it is important to tick ‘no brand substitution’ or write the specific device you want to prescribe on electronic prescriptions to prevent substitution. The risk with substitution is patients being inadequately prepared to use their device and subsequent unnecessary delays in administration of adrenaline.
ASCIA action plans for anaphylaxis
ASCIA’s action plans for anaphylaxis clearly outline the management of anaphylaxis and should be provided with an AI in all age groups. They are free to download and are available in Anapen, EpiPen and generic versions. The free AllergyPal app was developed by the Murdoch Children’s Research Institute and allows patients to store an electronic copy of their signed action plan on their phone.
Supportive management
Allergen removal
Additional supportive management includes removal of the allergen, if present. For tick bites it is important to not forcibly remove ticks. The safest way to remove a tick is to kill it using an ether-containing solution and allow it to drop off (‘freeze don’t squeeze’).1,5 For patients with known tick anaphylaxis, the tick should only be removed under medical supervision.5 For bee stings, flick out the sting as soon as possible using a fingernail or the edge of a credit card.
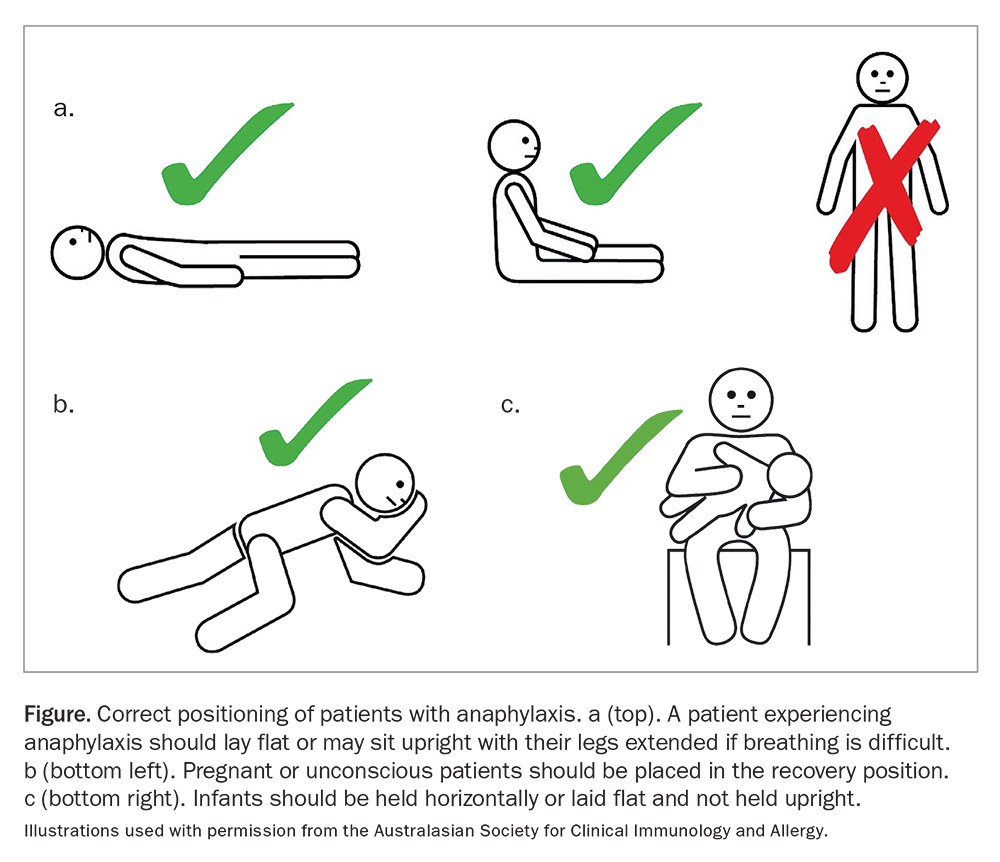
Positioning of the patient
Correct positioning of a patient with anaphylaxis is crucial and often overlooked. A patient may die if they sit or stand suddenly, as upright posture during anaphylaxis is associated with an increased risk of death.1 A patient experiencing anaphylaxis should lay flat or may sit upright with their legs extended if breathing is difficult (Figure). Pregnant or unconscious patients should be placed in a left lateral (recovery) position and infants should be held horizontally and not upright over the shoulder.6,9,10
{kind=link}
Patients should not be allowed to stand or sit for at least one hour after receiving adrenaline and four hours if they have received two or more doses, even if they appear to have recovered.3,4,8 Patients should be transported to and from the ambulance on a stretcher or wheelchair even after adrenaline has been administered.
Oxygen administration
If available, high-flow oxygen should be given to all patients with anaphylaxis. Airway support should also be provided if needed.
Intravenous fluids
For hypotensive patients, give IV normal saline 20 mL/kg rapidly and consider additional wide-bore IV access. Tachycardia or floppiness may be signs of hypotension in infants.6,10 Patients with cold-induced anaphylaxis should only receive warmed IV fluids.
Additional pharmacological treatments after IM adrenaline
Antihistamines and corticosteroids do not treat or prevent the cardiovascular or respiratory signs of anaphylaxis.3,6,8 Nonsedating oral antihistamines may be given to help relieve urticaria and angioedema. Injected promethazine should not be used in anaphylaxis because it can cause hypotension and muscle necrosis.
Corticosteroids have no place in the initial treatment of anaphylaxis, but they may be given after adrenaline in people with a history of reactive airways, or potentially to help prevent biphasic reactions (with minimal evidence).5,8,12
Salbutamol may be given for relief of bronchoconstriction in addition to adrenaline but should not be used in place of adrenaline. There is some evidence that high-dose inhaled salbutamol may help to relieve severe abdominal pain in food allergic reactions.24
Nebulised adrenaline (one nebule 1:1000) may be given to relieve upper airway obstruction in addition to IM adrenaline.
Duration of monitoring
ASCIA recommends that after administration of adrenaline a patient should be transported by ambulance to hospital for a minimum of four hours.3,6 In remote areas where access to a hospital may not be feasible, a patient should be transported to a medical facility equipped for resuscitation.
ASCIA also recommends patients should be considered for overnight admission if they meet the following criteria:
- severe or protracted anaphylaxis (e.g. required repeated adrenaline doses or IV fluid resuscitation)
- a history of severe or protracted anaphylaxis
- concomitant illness (e.g. severe asthma, history of arrhythmia, systemic mastocytosis)
- live alone or are remote from medical care
- present for medical care late in the evening.
Minimal requirements on discharge
All patients at risk of re-exposure to their allergen, or for whom the allergen has not been identified, should be discharged with an AI or an authority prescription that should be filled immediately. Instructions regarding the recognition of anaphylaxis and the correct technique for the adrenaline injector should be provided. Each patient should have an appropriate ASCIA action plan for anaphylaxis.5 ASCIA action plans for anaphylaxis, drug allergy and management of allergic reactions are available online (www.allergy.org.au/hp/anaphylaxis/ascia-action-plan-for-anaphylaxis/).
Arrangements should be made for a consultation with a specialist allergist/immunologist and the patient should see their primary healthcare provider within a week of discharge. Patients with anaphylaxis usually see their primary healthcare provider annually for renewal of their AI authority prescription in between reviews with their allergy specialist. This is an excellent opportunity to refresh AI technique, revise signs and symptoms of anaphylaxis and discuss any reactions that have occurred since their last review. It is also important to optimise management of other conditions, such as asthma, to minimise the risk of fatal reactions.
Referral to a reputable national patient support organisation (see Box) is also recommended.
The need for a national minimum standard for the management of anaphylaxis
Minimum and evidence-based standards for the management of anaphylaxis are needed nationally across all healthcare sectors. Work is in progress towards implementing such standards in Australia with the hope of reducing fatalities, improving patient outcomes and providing clear guidance for healthcare professionals.
Conclusion
With increasing hospital admissions for anaphylaxis in Australia, it is likely that there is a parallel increase in patients with anaphylaxis presenting to primary practice with acute reactions as well as for follow-up care. Diagnosis is made on clinical grounds, and early recognition and appropriate prompt treatment reduce the risk of adverse outcomes. Adrenaline is the first-line treatment for anaphylaxis and should be given without delay by IM injection in the outer mid-thigh. There are no contraindications to giving adrenaline if anaphylaxis is suspected. ASCIA has recently updated its guidelines for the acute management of anaphylaxis in line with current evidence and provides online access to anaphylaxis resources to help health professionals provide both acute care and ongoing management for patients with anaphylaxis. MT