Contraception choice dilemma. A woman with migraine with aura

The onset of migraine with aura in a 43-year-old woman impacts her contraceptive options, the condition being a contraindication to combined hormonal contraception. The evidence-based UK Medical Eligibility Criteria for Contraceptive Use (UKMEC) system is a useful framework for considering contraindications to contraceptives.
Case scenario
Rene, a 43-year-old woman, has been taking the combined oral contraceptive (COC) for around five years. She says ‘it changed my life’ as she has been skipping the hormone-free break, resulting in absent withdrawal bleeding, and she feels it has been helpful for her mood after previously experiencing negative mood changes with other hormonal contraception.
Rene has 5-year-old twins and does not want to become pregnant again. She has never smoked, her body mass index (BMI) is 27 kg/m2 and she is normotensive. Recent blood tests, including fasting lipid profile, liver function, renal function and electrolytes, were normal. She has no significant family history. Rene does not take any other medication and has no significant past medical history, although she tells you that during the past four months she has been experiencing episodes of blurred vision followed by a unilateral headache. These episodes are happening about every six weeks. On closer questioning, Rene indicates that these symptoms are accompanied by unilateral loss of vision that develops gradually and lasts around 20 minutes, after which she becomes nauseous and develops a left-sided headache. These headaches respond well to a rizatriptan 10 mg wafer, which she was given by an after-hours GP a few weeks ago. You explain to Rene that you believe these episodes are consistent with migraine with aura.
What is concerning about Rene’s history of migraines in combination with her use of the COC pill?
Commentary
Rene’s history has revealed a series of clinically relevant areas that can impact on her contraceptive options. As Rene is 43 years of age, she has a higher background risk of cardiovascular disease and venous thromboembolism than younger women, although in the absence of other risk factors the COC can be a suitable choice for women up to the age of 50 years.1,2
Of primary importance, however, Rene’s history is consistent with a diagnosis of new onset migraine with aura, which is an absolute contraindication (United Kingdom Medical Eligibility Criteria for Contraceptive Use [UKMEC] category 4) for use of a combined hormonal method of contraception.3 The Faculty of Sexual and Reproductive Healthcare, the publishers of UKMEC, also provides useful resources for making a migraine diagnosis and distinguishing migraines with aura from those without (http://ukmec.pagelizard.com/2016#sectionc/
diagnosis_of_migraine_with_or_without_aura). Rene should cease combined hormonal contraception and be recommended alternative contraception methods.
Given that Rene liked the COC because she could use it continuously to avoid withdrawal bleeds and because she felt that the COC has improved her mood, it will be important to address both of these issues when discussing alternatives. Progestogen-only methods can be associated with irregular bleeding or can result in amenorrhoea so it would be important to explore these options with her. In relation to mood changes, it is useful to remember that many factors can impact on mood and that these may change over time, and that all hormonal contraceptive options can potentially affect mood but a causal association has not been proven.4,5 Head-to-head trials are lacking for a benefit of one contraceptive pill, or even one method compared to another, in relation to an impact on mood.
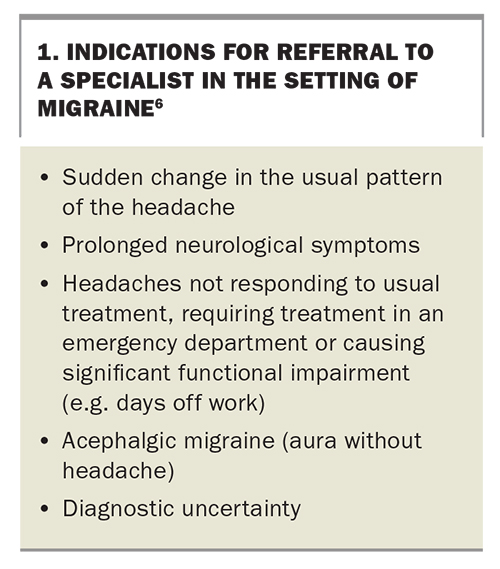
Rene’s headaches may also require investigation. Transient ischaemic attack needs to be considered among differential diagnoses when a patient presents with migraine with aura, or an aura without a migraine (acephalgic migraine), especially in the setting of risk factors for cerebrovascular disease.6 A detailed history and examination can be valuable in differentiating between the differential diagnoses. The indications for referral to a specialist in the setting of migraines are summarised in Box 1.6
{kind=link}
UKMEC as a guide for safe contraceptive choices
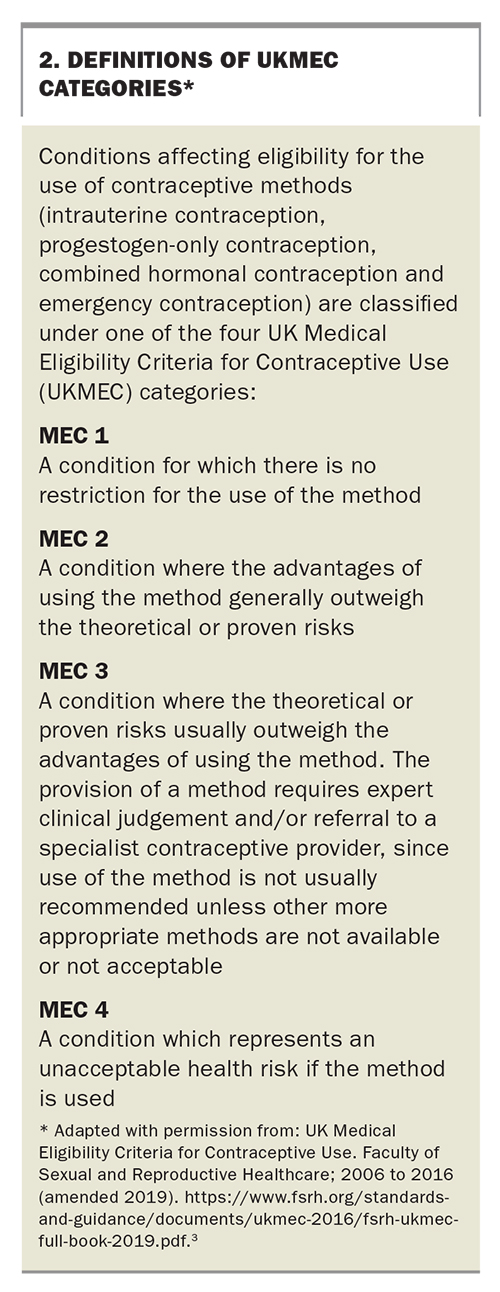
The evidence-based UKMEC system supports the safe provision of contraception and is a useful framework within which to consider contraindications to contraceptives. Conditions affecting eligibility for the use of each contraceptive method are classified under one of four categories; a MEC 1 condition is one for which no restrictions exist, and a MEC 4 condition represents an absolute contraindication (Box 2).3 Categories are listed for both initiation and continuation of using contraception options in the setting of various conditions. ‘Initiate’ indicates starting a method with an existing condition, and ‘continue’ indicates ongoing use of a method when a condition develops after initiation of the contraceptive method.
{kind=link}
Contraception options for women with a history of migraines
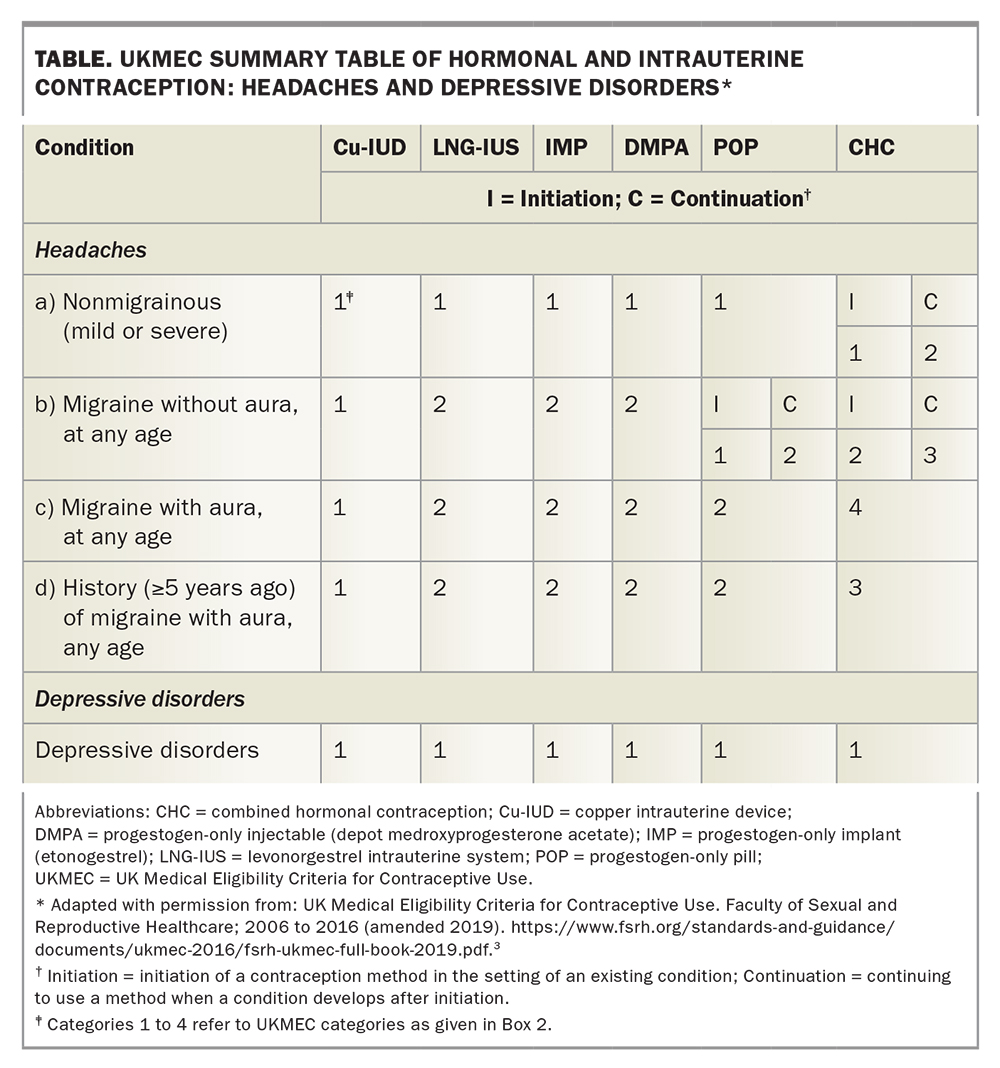
The use of combined hormonal contraception (COCs or the vaginal ring) in women with a history of migraine with aura is associated with an increased risk of stroke, and each risk factor may contribute to a synergistic effect.7,8 There is insufficient evidence to rule out an association between migraine without aura (or ‘simple migraine’) and an increased risk of stroke.8 UKMEC has accordingly classified a history of migraine without aura as category MEC 2 for initiation of combined hormonal contraception, and as MEC 3 for its continuation, and a history of migraines with aura as MEC 4 for any use of combined hormonal contraception (Table).3 A history of migraine with aura that was at least five years ago is classified as MEC 3.
{kind=link}
The safest options for contraception for those with a history of migraine, especially migraine with aura, are therefore nonhormonal and progestogen-only options. Nonhormonal contraceptive options are MEC 1 for migraine and include the copper intrauterine device (IUD), permanent female or male partner methods (tubal sterilisation or vasectomy) and the less effective barrier methods or fertility awareness methods. Progestogen-only options are all classified as MEC 2 for all types of migraine. These include the 52 mg and 19.5 mg levonorgestrel (LNG) IUDs (Mirena and Kyleena, respectively), the etonogestrel contraceptive implant (Implanon NXT), depot medroxyprogesterone injections and the progestogen-only pills (POPs), either the newer drospirenone 4 mg POP (Slinda) or the traditional low-dose levonorgestrel or norethisterone minipills (Microlut and Noriday, respectively).
Contraception decisions in women with a history of mood disorder
Change in mood is a common complaint in users of hormonal contraception.9 A causal effect is difficult to prove. The COC containing drospirenone 3 mg and ethinylestradiol 20 mcg has been shown to be of benefit in the very severe form of premenstrual syndrome known as premenstrual dysphoric disorder, compared with placebo. However, its efficacy has not been studied beyond three months of use and it is unknown whether other combined hormonal methods would have a similar effect.10 Use of any hormonal contraception is MEC 1 in those diagnosed with a depressive disorder (Table).
There is no evidence to guide choice of alternative methods of hormonal contraception for women concerned their method is contributing to poor mood. Logically, however, a lower hormone dose could be beneficial. For those using a COC, consider switching to a lower dose if possible (although this is not an option in Rene’s case as all COCs are contraindicated). Hormonal IUD use is associated with low systemic exposure, with the 19.5 mg LNG IUD having a 50% lower level of LNG systemic exposure than the 52 mg LNG IUD.11 Many women also choose the copper IUD to avoid hormonal side effects.
Hormonal contraception and bleeding patterns
Combined hormonal contraception results in a regular withdrawal bleed in the hormone-free break and reduces menstrual blood loss. Users may choose to eliminate bleeding by skipping the hormone-free periods for three months at a time (tricycling) or for longer through extended use. This may improve efficacy, reduce bleeding and has the advantage of minimising the oestrogen withdrawal symptoms of headache and pelvic pain.12
From a medical perspective, expert consensus indicates there is no upper limit for the length of time combined hormonal methods can be used continuously, although extended regimens can be associated with troublesome breakthrough bleeding.13 This can be managed by using a flexible regimen: hormones are used on consecutive days until there are four or more days of breakthrough bleeding, contraception is then stopped for four days, provided the ring or active pills have been used for the previous 21 days.14
Progestogen-only methods can result in unscheduled irregular bleeding or even amenorrhoea, depending on their type and mechanism of action. Amenorrhoea occurs in around 20% of implant users, while 40% of those using a 52 mg LNG IUD and 23% of 19.5 mg LNG IUD users become amenorrhoeic.15-17 Traditional POPs can result in unscheduled bleeding because they do not have a reliable effect on ovulation.18 However, the newer drospirenone 4 mg POP works by preventing ovulation, and although irregular bleeding can be common in the first few months of use, around 45% of users are amenorrhoeic by nine months of use.19
Efficacy
The efficacy of contraceptive methods varies between perfect and typical use. The long-acting reversible methods are largely independent of user input and have very high efficacy. User-dependent methods have a much lower typical use efficacy. The typical and perfect use efficacy is the same for all oral methods, although the narrow three-hour missed pill window for the traditional POPs may make them less effective in practice than the COCs and the drospirenone 4 mg POP, which have a 24-hour missed pill window.
Practice points
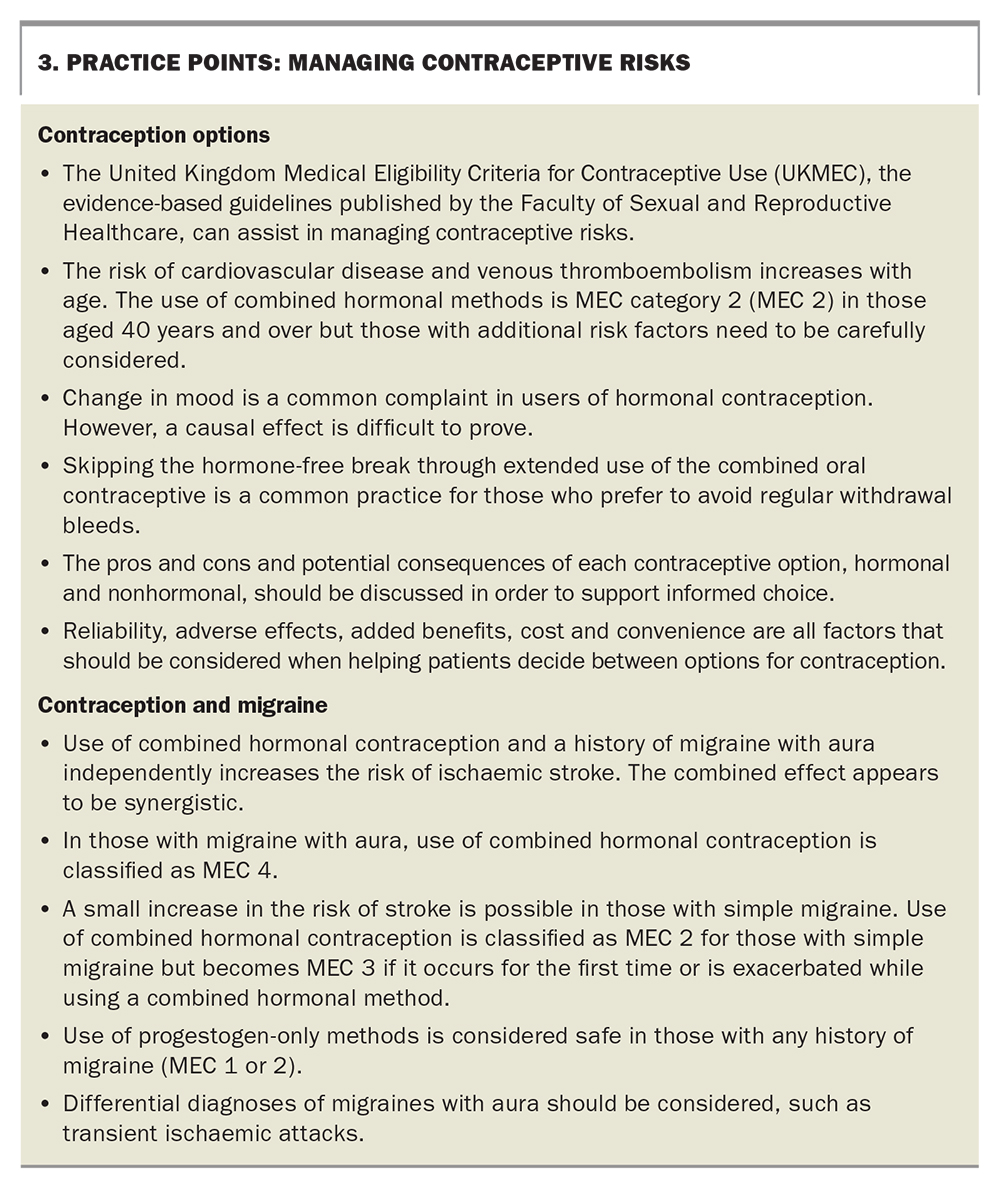
Practice points regarding managing the risks of using contraceptives generally and in women with migraine are listed in Box 3.
{kind=link}
Rene's progress
You discuss with Rene the need to cease the COC because of the enhanced risk of stroke, and although she worries about finding a method that will suit her as well as the pill, she is willing to learn about safe alternatives. Rene likes the idea of a method with a lower dose of hormones or no hormones and she would also like a method that will result in reduced or no menstrual bleeding. You discuss the pros and cons of all potentially suitable methods and inform her that a hormonal IUD would be unaffected by interactions if she were to be prescribed a liver enzyme-inducing medication for treatment of migraine in the future (e.g. topiramate).20,21
Rene is quite keen on the idea of an IUD and prefers a hormonal to a copper IUD, as it will have the added benefit of reducing menstrual bleeding, but she would like time to think about it. In the meantime, she decides to switch to a POP and chooses the new drospirenone 4 mg POP as she worries she may forget to take a traditional POP on time. You schedule a follow up appointment in three months’ time, with advice to come back sooner if she would like to proceed with a hormonal IUD or if her migraines are not improving.
Rene returns to see you for review after three months. Her migraines continue to respond well to rizatriptan and became much less frequent after stopping the COC. You decide no further investigations are required. Rene is happy taking the drospirenone 4 mg POP as she has had no significant adverse effects and has decided she would like to continue this method in the immediate future. MT