Polycystic ovary syndrome: optimal management in general practice

Polycystic ovary syndrome
Women's health
Diagnosis of polycystic ovary syndrome (PCOS) is often delayed, partially due to the diversity of presenting symptoms, resulting in frustration for patients. GPs play a vital role in the early diagnosis of PCOS and timely referral of patients, and in the prevention and management of long-term complications.
Polycystic ovary syndrome (PCOS) is a heterogeneous condition. Its prevalence depends on the study population and ethnicity and varies from 12% to 21% in women of reproductive age.1,2 Women with PCOS are at increased risk of reproductive and metabolic abnormalities, which can have a significant impact on mental health and quality of life. This review aims to help GPs diagnose and manage PCOS, screen for and manage complications, recognise the need for a multidisciplinary approach and identify indications for specialist referral.
Pathophysiology
PCOS is characterised by insulin resistance which is independent of, but exacerbated by, obesity.3 Women with PCOS may have increased androgen secretion from the ovaries (and adrenals), decreased sex hormone-binding globulin (SHBG) synthesis in the liver and, subsequently, increased free testosterone levels.
Diagnosis
A timely diagnosis is a key area in which PCOS care can be improved. Many women report seeing multiple healthcare professionals before a diagnosis of PCOS is established, with up to one in three women reporting that it took more than two years to establish a diagnosis from first presenting to a healthcare professional about their symptoms.4,5 Research shows that receiving a diagnosis of PCOS is important and that many women feel relief when a diagnosis is established.6,7 Delayed diagnosis is associated with dissatisfaction with the diagnosis experience and with symptoms of anxiety and depression.5,8 Delay in a diagnosis of PCOS is a lost opportunity for symptom management, for counselling regarding future fertility, to improve quality of life and for early engagement in preventive strategies for metabolic complications.5
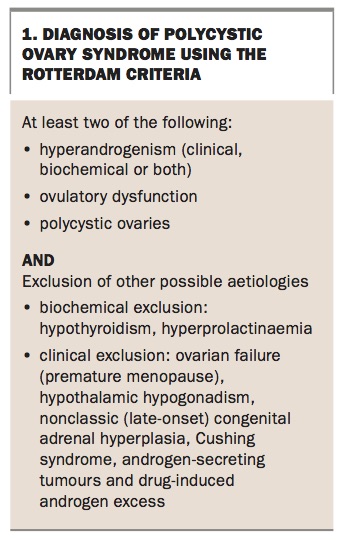
The Rotterdam Criteria (European Society of Human Reproduction and Embryology [ESHRE] and American Society for Human Reproductive Medicine [ASRM]) are the internationally accepted diagnostic criteria for PCOS.9 At least two of the following three features are required:
- hyperandrogenism (clinical, biochemical or both)
- ovulatory dysfunction
- polycystic ovaries.
Other possible underlying causes must also be ruled out.10
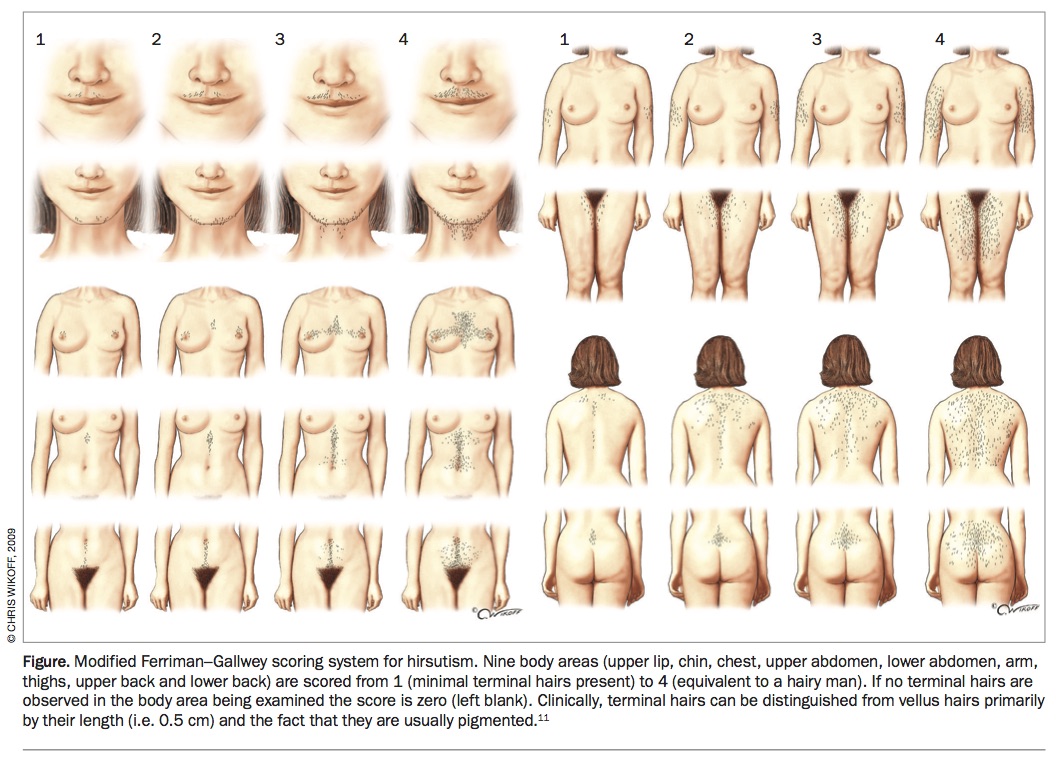
Hyperandrogenism
Clinical manifestations of PCOS include hirsutism, acne and alopecia. Hirsutism can be quantified by the modified Ferriman–Gallwey (mFG) scoring tool (Figure) with differing cut-off values based on ethnicity.11 An mFG score of 3 or more indicates excessive hair in women of Asian descent, whereas a score of 6 to 8 is used to diagnose hirsutism in women of most other ethnicities.12 Biochemical diagnosis of hyperandrogenism is best made through measurement of free androgen index or calculated free testosterone levels (based on total testosterone and SHBG) because the assays used to measure total testosterone levels are often inaccurate at the low levels present in women. Other androgens need not be measured, unless a secondary cause is suspected (Box 1).
{kind=link}
{kind=link}
Ovulatory dysfunction
Irregular menstruation (cycles more than 35 days or less than 21 days) and reduced fertility are the clinical manifestations of ovulatory dysfunction. Infrequent menstruation due to anovulation and reduced uterine progesterone exposure may result in endometrial hyperplasia and risk of endometrial cancer.13
Polycystic ovary morphology
Ultrasound is not required for a diagnosis of PCOS if hyperandrogenism and oligomenorrhoea are both present and secondary causes are excluded (Box 1). Ultrasound should be performed in postadolescent women where only one of these features is present. Ultrasonographic features of PCOS are 25 or more follicles (2 to 9 mm) per ovary or an ovarian volume of more than 10 mm (unilateral or bilateral) when using high-resolution transvaginal ultrasound. Transabdominal ultrasound can be performed in women who have not been sexually active; however, this may be less accurate, especially in those with abdominal obesity.
Diagnosis in adolescents
Diagnosis is often challenging in adolescent girls and requires both features of hyperandrogenism and oligomenorrhoea. Pelvic ultrasound is not recommended for diagnosis in this cohort, particularly before the age of 17 years, as large-volume ovaries with multiple cysts are often seen in normal puberty. Furthermore, irregular menses, particularly up to two or three years postmenarche is not considered abnormal.10 National and international guidelines recommend following up adolescent girls with features suggestive of PCOS.10,14 Annual follow up may also be appropriate to ensure early diagnosis and to provide education to prevent weight gain.
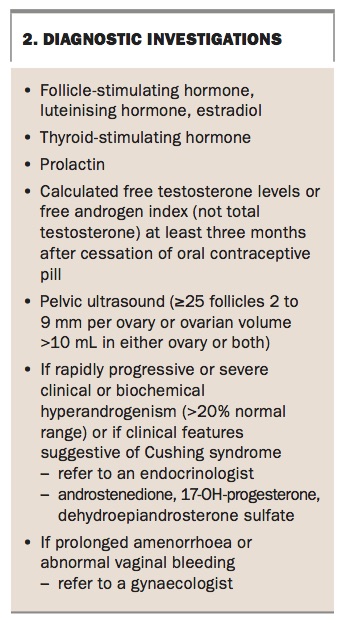
Diagnostic investigations
PCOS is a diagnosis of exclusion. Box 2 lists the required investigations to exclude other causes for presenting symptoms. For women taking the oral contraceptive pill (OCP), it is important to request the blood test at least three months after cessation of the OCP. At OCP cessation, appropriate advice about barrier contraception should be given if pregnancy is not desired. Referral to an endocrinologist is recommended for patients with rapidly progressive or severe hirsutism and/or severe biochemical hyperandrogenism or those with characteristic features of Cushing syndrome. Women with prolonged amenorrhoea (more than three months) need a referral to an endocrinologist or gynaecologist. Abnormal vaginal bleeding warrants referral to a gynaecologist for further assessment. Measurement of insulin levels is not reliable due to assay inaccuracy and therefore is not recommended.
{kind=link}
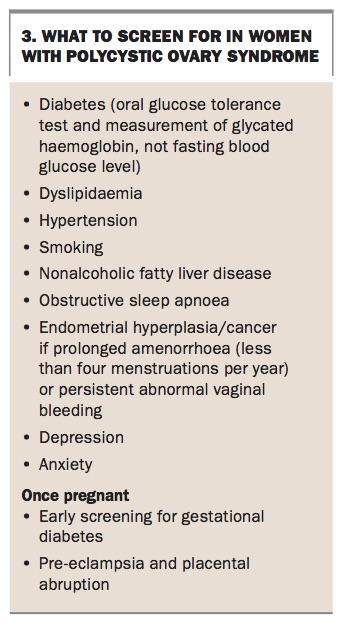
Screening for PCOS-associated conditions
Screening for diabetes should be done using a two-hour oral glucose tolerance test (OGTT) rather than fasting glucose level as impaired fasting glucose is a poor predictor of impaired glucose tolerance (IGT) in PCOS.15,16 Measurement of glycated haemoglobin (HbA1c) may also be a helpful screening tool. An OGTT needs to be repeated annually for women with IGT and every two to five years for those with normal results based on diabetes risk assessment of body mass index (BMI), family history and history of gestational diabetes. Women should also be screened for hypertension, dyslipidaemia and nonalcoholic fatty liver disease (Box 3).
{kind=link}
Management
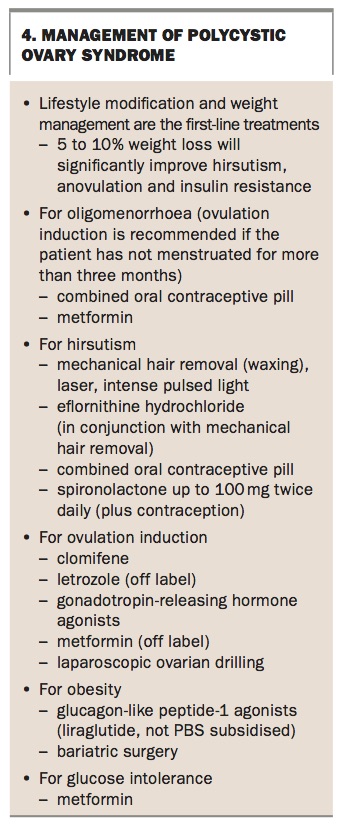
PCOS affects the reproductive, metabolic and psychological aspects of a woman’s health. Ideally, a multidisciplinary team consisting of a GP, endocrinologist, gynaecologist, dietitian, exercise physiologist and psychologist is needed for optimal management. A management strategy is outlined in Box 4.
{kind=link}
Weight
Lifestyle modification and weight management are first-line treatments for PCOS, with preventing weight gain the primary aim. Weight loss of 5% has been shown to reduce androgen levels, improve ovulation, re-establish menses, increase the success rate with fertility treatments and decrease cardiometabolic risk factors.10 However, engaging women in lifestyle modification can be difficult, and long-term sustainability is low. Medical therapy can be considered in some patients; however, there is limited evidence regarding its efficacy in women with PCOS. Women with a BMI of more than 35 kg/m2 may benefit from referral for bariatric surgery, particularly if planning pregnancy.17
Oligomenorrhoea and amenorrhoea
A minimum of four menstrual cycles per year is recommended to provide endometrial protection. Use of the OCP is recommended if amenorrhoea persists for more than three months.18 When the OCP is contraindicated or not desired, other options include oral progesterone for 10 days every three months or insertion of an intrauterine device. Women with PCOS have a 1.5 times higher risk of venous thromboembolism compared with women without PCOS, and therefore they need to be informed that this risk is further increased by taking the OCP.19 The OCP may also increase blood pressure and worsen dyslipidaemia in women with PCOS.20,21 However, current evidence does not show an increased risk of impaired glucose metabolism with the OCP.22 Low-dose OCP preparations are preferable, with similar efficacy and reduced cardiometabolic effects.23
Hirsutism
Mechanical hair removal by waxing or plucking, or by laser, is the primary intervention for hirsutism. Eflornithine hydrochloride can also be prescribed for use in conjunction with hair removal techniques to reduce the frequency of hair removal. In cases where oral pharmacotherapy is needed, the OCP is the first-line treatment as it reduces androgen secretion from the ovaries. No particular formulation of OCP is shown to be superior in treating hirsutism in PCOS,19 and it may take up to six months for a noticeable effect. Spironolactone, an androgen receptor antagonist, used alone or in combination with the OCP, can also reduce the growth of terminal hair. It is important to advise the patient to use contraception while taking spironolactone as it affects the development of fetal male genitalia if taken during pregnancy.2 Metformin is also shown to reduce androgen levels but its beneficial effect on hirsutism is limited.14
Subfertility
GPs can play a major role in counselling their patients with PCOS on the importance of age in family planning. Research has shown a similar number of children born to women with PCOS and those without. However, more women with PCOS use fertility treatments.24 Weight loss improves ovulation and fertility and should be encouraged in all women with a BMI of 25 kg/m2 or more. In general practice, lifestyle modification, and potentially metformin use, can be considered for six months in overweight women aged less than 35 years before referring to a fertility specialist.10 Women with PCOS and a BMI of 35 kg/m2 or more may benefit from referral to a bariatric surgeon. Pregnancy should be delayed until the acute postoperative phase has passed and weight has stabilised. Once other causes of infertility are excluded, clomifene (selective oestrogen receptor modulator) or letrozole (off label) (aromatase inhibitor) are used as first-line therapy for ovulation induction in both lean and overweight women with PCOS.10,25 Other available fertility treatments include gonadotropins, laparoscopic ovarian drilling and in vitro fertilisation if other interventions fail. It is important not to delay referral to a fertility specialist, particularly for women aged more than 35 years.
Metabolic syndrome
Screening and treatment for components of metabolic syndrome are recommended at the time of diagnosis. Weight loss is the primary treatment. Statins are shown to decrease testosterone in addition to improving the lipid profile, but this has not been associated with improvement in acne, hirsutism or regularity of menses.14 There are no long-term trials that examine the long-term effects of statins on cardiovascular events in women with PCOS.
PCOS in lean women
This group of women often present with milder physical characteristics of PCOS compared with obese women. However, they still have a higher prevalence of metabolic syndrome, insulin resistance and IGT compared with lean women without PCOS.19 Apart from strategies for weight loss, management of PCOS is similar to that for affected overweight or obese women but with a focus on preventing weight gain. Exercise should be encouraged as it improves insulin resistance and ovulation, regardless of its effect on weight.26 It is important to distinguish PCOS from oligomenorrhoea and amenorrhoea associated with oestrogen deficiency (due to hypogonadotropic hypogonadism or premature ovarian failure), particularly in women with a low BMI.
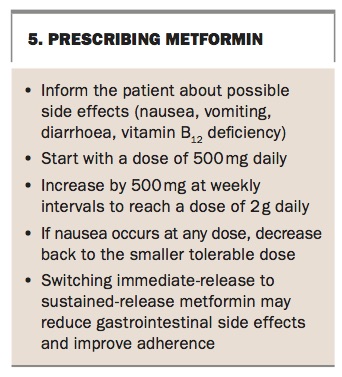
Prescribing metformin
Metformin reduces hyperinsulinaemia by improving insulin resistance. In both obese and lean women with PCOS, metformin is shown to also reduce androgen levels, increase ovulation rates and restore regularity of menses.14 Prescribing metformin is recommended for all women with PCOS who have IGT.10,14 Metformin can prevent the progression of IGT to diabetes.27 Guidance to prescribing metformin is shown in Box 5.
{kind=link}
Psychological health
Women with PCOS are at increased risk of depression and anxiety symptoms, which are at least partially due to delayed diagnosis as well as features associated with the syndrome.10 Guidelines recommend routine assessment of mental health and screening for anxiety, depression, eating disorders, negative body image and psychosexual disorders. A tool for assessment of emotional health can be found at The Jean Hailes for Women’s Health website.28
Information provision and shared decision-making
Lifestyle management and preventive strategies rely on engagement. Therefore it is important to equip women with PCOS to make informed decisions about their health by providing high-quality information. Research shows that at the time of diagnosis, women want specific and practical information about lifestyle management and medical therapy, the potential long-term consequences of PCOS and emotional support and counselling. Yet this information is not often provided or does not meet the woman’s needs.4,5 Improving women’s knowledge of PCOS and providing better quality information are associated with increased engagement with lifestyle management and improved quality of life.6,29 Research often identifies weight, menstrual irregularity, fertility and hirsutism as key concerns among women with PCOS.5,6,30,31 However, these differ with life-stage and personal background, highlighting the need to elicit and prioritise women’s individual concerns to guide comprehensive care. Utilising chronic disease management plans and referring patients to a dietitian, exercise physiologist and psychologist are important options to consider.
Conclusion
PCOS affects multiple aspects of a woman’s physical and mental health. A timely diagnosis is important to reduce anxiety and frustration and to manage the associated short- and long-term complications of this condition. Education and a multidisciplinary approach will improve the patient’s engagement and outcomes. MT