Pruritic bullae on a girl’s arms and legs

Test your diagnostic skills in our regular dermatology quiz. What is the cause of these itchy bullae, which have occurred over the summer?
Case presentation
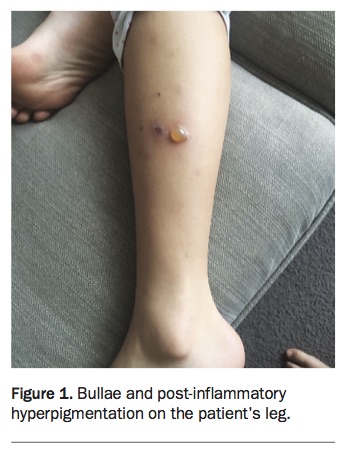
A 9-year-old girl presents with her mother, who is worried about bullae that have developed on the child’s lower and upper limbs during the recent summer (Figure 1). The lesions occur after the girl’s tennis lessons, persist for two to three days and then subside, and are followed by crusting and healing with post-inflammatory hyperpigmentation. The lesions are intensely pruritic and have tended to become infected.
{kind=link}
The girl moved to Australia from the UK a year ago. She is otherwise well.
Differential diagnoses
Conditions to consider among the differential diagnoses for a child of this age include the following.
- Bullous impetigo. Although relatively common in neonates, bullous impetigo is uncommon in older children. The blister formation is mediated by exfoliative toxins produced by Staphylococcus aureus. Small vesicles enlarge into flaccid transparent bullae. The rash has a wide possible distribution and is not intensely itchy, and there are usually no systemic symptoms. However, in neonates the condition may progress to sepsis and should be treated vigorously. Staphylococcal scalded skin syndrome is the systemic manifestation of the same pathophysiology but is mediated by a different toxin.
- Allergic contact dermatitis. Vesiculobullous, itchy reactions are not uncommon manifestations of acute reactions to allergic contact dermatitis. Common allergens in children include plants and topical antibiotics and antifungal agents. The distribution of the reaction corresponds to the area of contact (Figure 2) but may be diffuse when caused by body washes and shampoos. Although the rash in this case corresponded to specific irritant sites, the distribution was not geometric nor did it correspond to topical agents.
- Bullous pemphigoid. This is typically a condition of the elderly; the childhood variant of the disease is very rare. In the bullous phase, numerous itchy, tense bullae appear on normal and erythematous skin in an annular pattern. The blisters are filled with clear or blood-tinged fluid and erode after several days. The blisters first appear acrally (hands and feet) and then progress to involve other sites, including the mucosae and genital region.
- Linear IgA bullous disease. Also known as chronic bullous disease of childhood, linear IgA disease is a rare autoimmune dermatosis. It is most common in adults but a variant occurs in prepubertal children with acute onset of blistering of the hands, face and limbs. Blisters appear on normal skin arranged in an annular distribution or a targetoid shape. Approximately half of people with linear IgA disease develop blisters and ulcers on the mouth and lips and it may involve the conjunctivae. Itch is variable in the disease.
- Bullous drug eruption. Adverse drug reactions resulting in blisters or bullae can result from multiple different medications and can have a wide spectrum of severity: from mild and localised to life-threatening. The eruptions range from fixed drug eruptions, drug-induced linear IgA disease, to erythema multiforme and toxic epidermal necrolysis. A clinical diagnosis of a bullous drug eruption is made after excluding other reactions, such as infections, and identifying the drug involved. Examples of drugs that can cause blistering are ibuprofen (a common cause of fixed drug eruption), lamotrigine (which can result in toxic epidermal necrolysis) and vancomycin (which is implicated in linear IgA disease). Additionally, drugs that cause photosensitivity such as doxycycline can result in blistering.
- Bullous insect bite reaction. This is the correct diagnosis. Vesiculobullous reactions to insect bites are not uncommon although most reactions present as pruritic erythematous papules. The pruritic blisters are usually grouped over exposed areas. The reaction is not dependent on the insect involved but is related to the individual’s IgE and cell-mediated immunity. After a patient becomes sensitised, subsequent bites from the same insect result in progressively more severe and widespread reactions as previous bites are reactivated. Eventually, repeated bites over time lead to desensitisation. This sequela of insect bites is mostly seen in children of preschool age as they have not become desensitised to the bites. In this case, however, the child had arrived in Australia recently from a cold climate and had not been sensitised to local insects.
{kind=link}
Diagnosis
The diagnosis of bullous insect bite reactions is based on history and examination. Although patients may not remember being bitten specifically, they may suspect it based on their location when the lesions appeared. In this case, the girl’s parents strongly suspected that the child was bitten at the tennis courts, which were located next to a swampy area with many insects around.
Although rare, a severe reaction to insect bites occurs in patients with chronic lymphocytic leukaemia and other haematological malignancies.1 The reaction to the bites can precede diagnosis or indicate relapse, and therefore further evaluation or investigations for haematological malignancies should be considered, particularly if the patient is unwell or has desensitised to insect bites in the past.
Management
Management of bullous insect bites involves symptomatic relief, treatment of superinfection, and prevention of subsequent bites. The itch can be mitigated with oral antihistamines (e.g. loratidine), and a potent topical corticosteroid such as betamethasone dipropionate 0.05% ointment should be applied to the lesions. If infection is present, treatment with oral antibiotics is indicated. Prevention of insect bites can be accomplished by avoiding stagnant bodies of water, wearing clothing with long sleeves, using insect-repelling electrical devices or burning coils, and applying insect repellents. The most effective insect repellents tend to be products that contain DEET. The reactions will slowly subside as the patient is desensitised to insect bite, and the prognosis is good. MT