Peeling of the palmar surface of the fingers

Test your diagnostic skills in our regular dermatology quiz. What is the cause of the asymptomatic skin peeling affecting this young boy’s fingers?
Case presentation
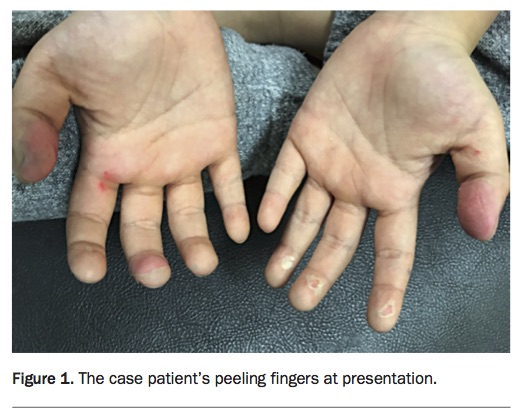
A 4-year-old boy presents with his father, who is concerned about asymptomatic peeling of the palmar surface of the tips of several fingers that started approximately one week previously (Figure 1). The boy has no previous medical history or skin pathology. On examination of his feet, peeling is evident on the plantar surface of several toes.
{kind=link}
Questioning reveals that the boy has been unwell with pharyngitis, which was resolving when the finger peeling was noticed. There are no relevant findings on examination of his throat apart from enlarged tonsils and mild lymphadenopathy.
Differential diagnoses
Conditions to consider among the differential diagnoses for a child of this age include the following.
- Allergic contact dermatitis. Allergic contact dermatitis follows sensitisation and re-exposure to an allergen and usually spreads beyond the area of contact. In acute reactions, an itchy eczematous eruption occurs characterised by erythema, blistering and oedema. In chronic cases, the skin affected is more likely to appear as lichenified and scaly. The dorsal as well as the palmar and plantar surfaces of the hands and feet are typically involved. Allergic contact dermatitis is unusual in small children, who typically have less contact with potential allergens than adults.
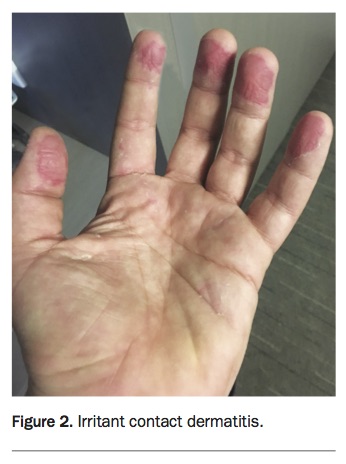
- Irritant contact dermatitis. Irritant contact dermatitis encompasses a wide range of presentations depending on the irritant and the frequency and duration of exposure. Features may include vesicles, redness, scaling, erosion and lichenification (Figure 2). Patients typically report itch, burning and sometimes pain. The dorsal and plantar surfaces are less often involved than in allergic contact dermatitis.
- Blistering digital dactylitis. Blistering digital dactylitis is an infection of the volar fat pad of the tips of the digits secondary to Staphylococcus aureus or group A streptococcus that can be cultured from the skin. The skin appears darkened before blister formation adjacent to the nail and volar surface of the fingertip. Infection typically follows trauma and is most common in 2- to 16-year-olds.
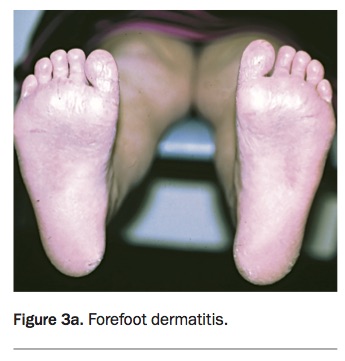
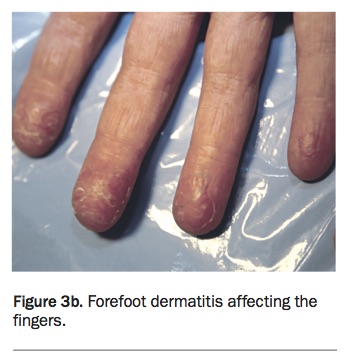
- Forefoot dermatitis. Also known as juvenile plantar dermatosis, forefoot dermatitis occurs in prepubescent children from the age of 3 years, typically on a background of atopic dermatitis or psoriasis. It is characterised by fissuring and a shiny red appearance on the plantar surface of the feet (Figure 3a). The interdigital spaces and dorsa are spared. Less commonly, a similar eruption can be present on the hands (Figure 3b).
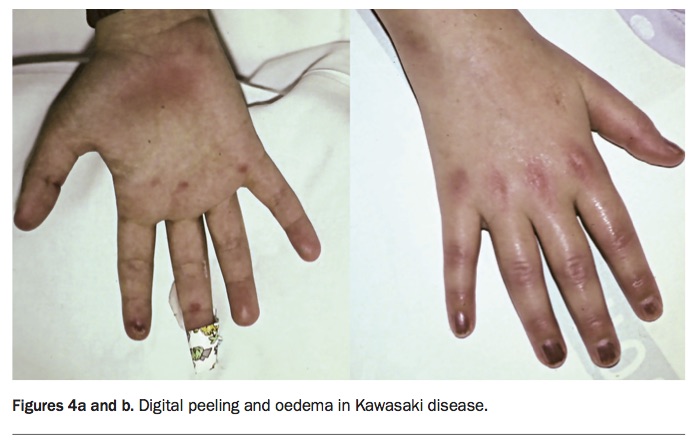
- Kawasaki disease. This condition is most important to be aware of because it has potential serious complications. An acute febrile illness with inflammation of small and medium-sized blood vessels occurs most commonly in children under the age of 5 years, with a peak incidence in 1- to 2-year-olds who tend to present as very unwell. Kawasaki disease is diagnosed on criteria of a persistent high fever (>39ºC) and four of five cardinal signs: conjunctival injection without exudate; morbilliform, target-like rash or maculopapular; oral and lip erythema; peripheral limb erythema, oedema and digital peeling (Figures 4a and b); and cervical lymphadenopathy.1 The digital peeling is a late event typically occurring about two weeks after the onset of fever. The condition resolves in four to eight weeks. However, up to 20% of untreated cases are at risk of developing dilation and/or constriction of the coronary arteries; intravenous immunoglobulin and aspirin given within 10 days of the onset of fever can greatly reduce this risk. An echocardiograph is required to exclude coronary artery involvement six to eight weeks after onset of illness. The cardinal signs of Kawasaki disease were not present in the case patient described above, but it is an important differential diagnosis.
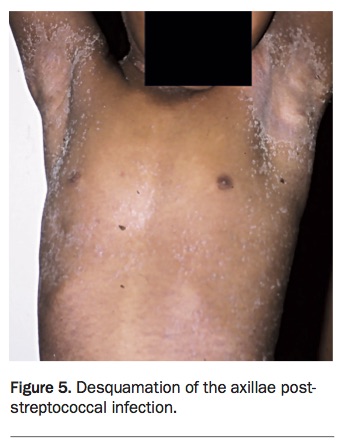
- Post-streptococcal digital desquamation. This is the correct diagnosis. Desquamation of the fingers and toes is a reactive phenomenon that can occur on approximately day six of infection with group A streptococcus. Infection with group A streptococcus can cause a wide spectrum of symptoms and skin manifestations, including pharyngitis, impetigo and scarlet fever. In cases of scarlet fever, a toxin-mediated condition, desquamation is more widespread and occurs on the fingers, toes and axillae (Figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Investigations
Diagnosis of post-streptococcal digital desquamation is clinical. A recent history of the manifestations of group A streptococcus infection, including impetigo, scarlet fever, cellulitis or pharyngitis, is necessary. To confirm group A streptococcus involvement, a swab of the infected skin or throat or serology for antistreptolysin o titre (ASOT) and DNAase B can be performed. For the case patient described above, the latter test confirmed the presence of group A streptococcus.
Management
The desquamation after infection with group A streptococcus can last two to six weeks. The priority of treatment concerns antibiotic therapy to reduce the risk of rheumatic fever and glomerulonephritis. Oral or intravenous penicillins or cephalosporins are indicated. Antibiotics have been demonstrated to reduce the risk of rheumatic fever and therefore rheumatic heart disease.2
Outcome
For the case patient, a 10-day course of oral cephalexin was prescribed and emollients were applied to his fingers. No further follow up was required. MT