Malaria. How global advances in control and treatment have changed the game

Significant progress in the global fight against malaria means that overseas travellers are now much less likely to acquire this potentially fatal disease. Improved treatments also allow a simpler ‘one-size-fits-all’ approach for treating the diminishing number of cases of malaria in Australia.
- Renewed efforts to control and eliminate malaria throughout the world have been outstandingly successful. This has ‘shrunk’ the global malaria map, meaning that at least for the time being, risk to travellers has diminished and is now concentrated in fewer geographical areas.
- More than 90% of imported malaria cases in Australia are now acquired in Africa, Papua New Guinea, India or Indonesia. Risk has been eliminated or is close to being eliminated in many popular tourist destinations such as Sri Lanka, Vanuatu, Thailand, China, Malaysia, the Philippines, Nepal and Vietnam.
- An increasing proportion of imported malaria is now seen in recent migrants, either on arrival to Australia or following travel back to their home country.
- New treatments based on the artemisinin derivative class of drugs are much safer, better tolerated and more effective; artemether-lumefantrine can almost always be used as initial treatment.
- Drug choices for prophylaxis remain doxycycline, atovaquone-proguanil and mefloquine, but all have risks and costs.
- Mosquito avoidance measures will become more important, as they protect not only against malaria but other emergent viruses such as dengue, zika and chikungunya.
Malaria is one of the most important diseases of mankind, thought to be responsible for more than 300 million deaths throughout human history. Tuberculosis and smallpox may be the only two infectious diseases to have taken a greater toll on human life through the ages.1 Malaria is therefore justifiably feared as a health threat to Australian travellers venturing to tropical and subtropical countries. However, its global reach has diminished in recent times as renewed global efforts to control this disease continue to take effect.
Malaria is caused by parasites known as Plasmodia, of which two species – Plasmodium falciparum and P. vivax – are responsible (in about equal numbers) for more than 90% of all cases seen in Australia. P. falciparum, considered the most dangerous species, can be acquired in both the Asia-Pacific and Africa, but P. vivax comes mostly from the Asia-Pacific region. Two other species – P. ovale and P. malariae – contribute less than 10% of Australia’s remaining malaria cases. Recently, additional species of ‘monkey’ malaria, including P. knowlesi, have been discovered in humans, but these seem confined to fairly remote jungle areas of Asia and South America and probably do not constitute major risks to Australian travellers.
This article addresses how changing global malaria control impacts on treatment and prevention of malaria in Australia by examining three key issues: the epidemiology of imported malaria within Australia; the implications of improved new treatments; and how these two factors impact on the risk-benefit balance when treating and preventing malaria in overseas travellers, now and into the future.
How and why has the global malaria situation changed?
It is important to remember that historically, malaria reached into parts of Europe, the US and Australia. Indeed, Australia was only officially declared malaria-free in 1975. This followed the Global Malaria Eradication Program overseen by WHO throughout the 1950s and 1960s. As with smallpox and polio, the objective then was to completely eradicate the disease. Of course this did not happen – although feasible in developed countries such as Australia, elimination proved too difficult in most of the tropical developing world where eradication was abandoned in favour of the less ambitious aim of control. Deteriorating health systems and widespread drug-resistance subsequently saw things worsen rapidly and by the early part of the 21st century it was estimated that almost two million lives were being lost every year to the disease.2
Recently, we have come back to the idea that complete global eradication of malaria might actually be a realistic objective. A key event came in 2007 when Bill and Melinda Gates set eventual global malaria eradication as their foundation’s ultimate goal – an audacious idea that has now been widely endorsed by WHO and the more than 35 countries that have committed to an objective of eventual malaria elimination.3,4 Increased funding has flowed to the cornerstones of malaria control, including the use of insecticide-treated bed nets, mosquito control and ensuring ready availability of safe and effective malaria drugs. A particularly important event was the rediscovery of artemisinin (contained in a herbal medicine previously used to treat malaria in ancient times) by a group of Chinese scientists. This led to the development of a class of drugs that are safe, are highly effective, are active against strains of malaria resistant to previous drugs and can be cheaply manufactured.5 This has improved how the estimated more than 200 million global malaria cases are treated each year. The game-changing significance of the artemisinin class of drugs was acknowledged when the 2015 Nobel Prize in Physiology or Medicine was awarded to Youyou Tu for her ‘discoveries- concerning a novel therapy against malaria’.
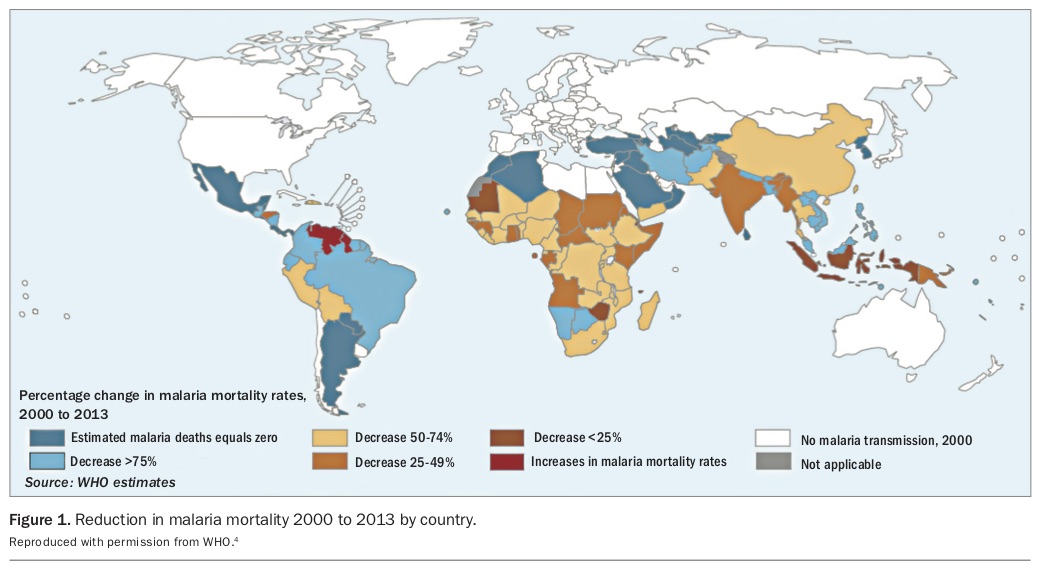
So how effective have these renewed efforts to combat malaria been? WHO now estimates that over a 15-year period annual numbers of malaria cases declined by 37% and deaths by 60%, equating to more than 1.2 billion cases being averted and more than six million lives being saved.4 Almost all countries have shared in this success with only one or two exceptions (Figure 1).
{kind=link}
Star performers include Sri Lanka (touted as the ‘next Bali’ for Australian tourists), which was recently declared completely malaria-free by WHO. Other popular travel destinations approaching elimination include Thailand, Vietnam, China, Nepal, Malaysia, the Philippines and Vanuatu. The few countries that have done less well are generally those experiencing conflict or major political dysfunction (e.g. Venezuela and Myanmar) or that have very large populations (e.g. India and Indonesia) or other significant logistic challenges (e.g. Papua New Guinea). An important issue in global malaria control in our own region is P. vivax, which is especially prevalent in the Asia-Pacific and has proved less susceptible to conventional control measures than its better known cousin P. falciparum. Because of this, many of Australia’s neighbours have seen a shift in epidemiology from P. falciparum to P. vivax as the predominant type of malaria. Because infection with P. vivax can cause later relapses from reactivation of sleeping liver stages (hypnozoites) this epidemiological change has important implications for treatment.
How has the epidemiology of imported malaria in Australia changed?
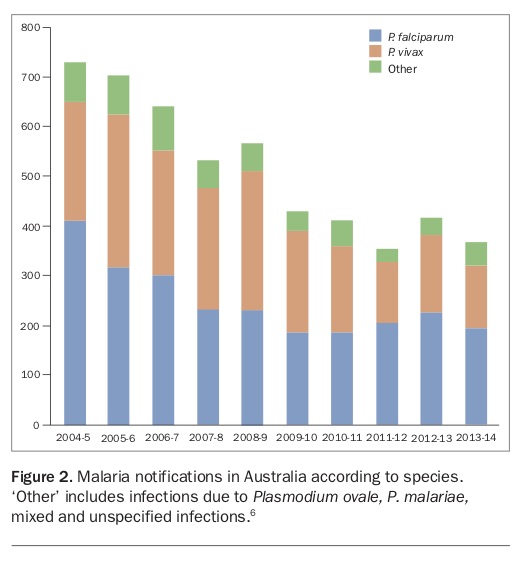
Although Australians are travelling more than ever and are increasingly travelling to the developing world, malaria cases in Australia are steadily declining, having more or less halved between 2004 and 2012 (Figure 2).6 This likely reflects lesser exposure to infectious mosquito bites due to improved malaria control in source countries.
{kind=link}
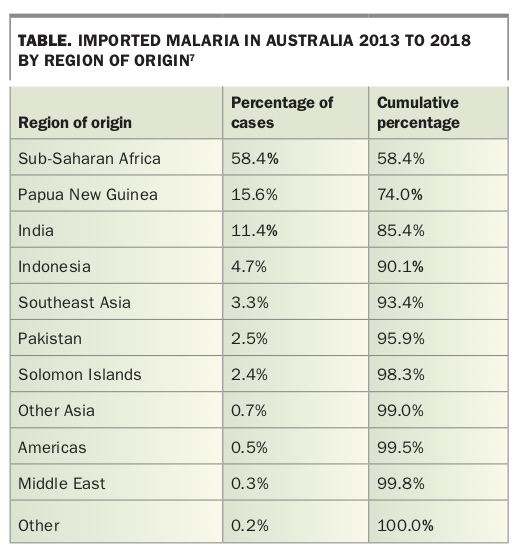
There also appears to be important changes in where malaria is being acquired, which travellers are infected and what type of malaria they are infected with. Latest notification data show that most imported malaria is now acquired in sub-Saharan Africa with the remainder mostly confined to one of three countries: Papua New Guinea, India and Indonesia (Table).7 Notably, only about 3% of cases were thought to be acquired in any other Southeast Asian country (including Cambodia, Thailand, Vietnam, Laos, the Philippines, Myanmar, Timor Leste and China) despite very high-volume travel by Australians to this region. Again, this probably reflects improved malaria control in this part of the world but also the nature of malaria transmission here, which is often confined to remote forest areas, especially in border zones that are rarely visited by tourists.
{kind=link}
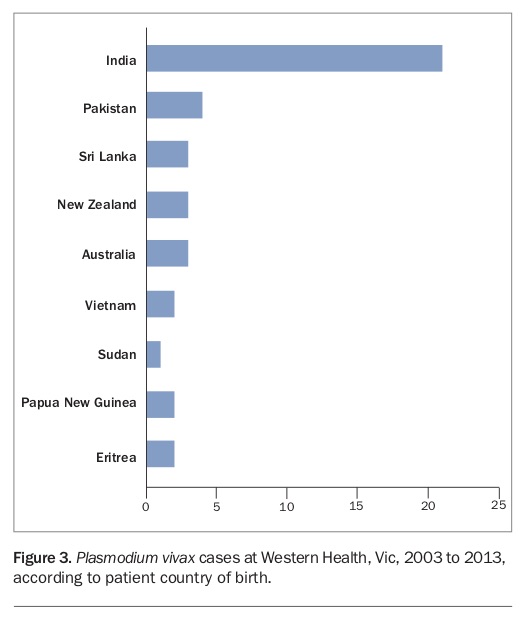
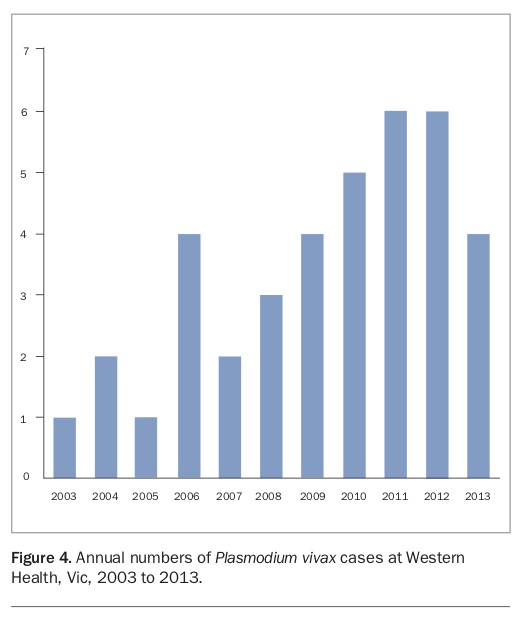
It is also notable that the source countries for imported malaria are relatively over-represented by those that have also been major contributors to Australia’s migration intake in recent years, including most notably Sudan (12.8% of cases) and India (11.4% of cases).7 This points to an important change in the demography of imported malaria cases, with higher proportions occurring in recent migrants in whom malaria is either detected as part of screening shortly after arrival or in whom malaria is acquired when returning to visit friends and relatives in their former home country. A striking example of this is seen at Western Health (which services the western suburbs of Melbourne) where almost all cases of P. vivax seen occur in overseas-born individuals, the majority from India (Figure 3). In contrast to the national trend, cases of P. vivax have been increasing in this area of Melbourne (Figure 4), probably reflecting a combination of migrant demographics, relatively stagnant progress in malaria control in India and the changing epidemiology that is seeing P. vivax predominate in much of the Asia-Pacific region.
{kind=link}
{kind=link}
How has the approach to treating malaria changed?
The development of the artemisinin class of drugs has revolutionised the treatment of malaria.5 Previously, treatment of malaria needed to be individualised according to the species of malaria and its likely drug-resistant characteristics based on where it was acquired. The mainstay of treatment for P. falciparum – quinine – carried potential for serious or at least very unpleasant side effects and had a relatively slow onset of action meaning that recovery was often delayed. By contrast, the artemisinins are characterised by being very safe, extremely well tolerated and having a much more rapid onset of action.5
Artemisinins are now manufactured as co-formulations in combination with a second long-acting partner drug that enables short courses (i.e. three days) that have high cure rates. WHO recommends these combinations, now referred to as ‘artemisinin combination treatments’ (ACTs), as first-choice treatment regardless of species, for almost all of the estimated more than 200 million malaria cases diagnosed globally each year.8
Although artemisinin resistance has emerged in the Greater Mekong region of Southeast Asia, currently this mainly manifests as somewhat slower rates of parasite killing and delayed clinical recovery, rather than treatment failure as such, and has not spread more widely.7 Currently, ACTs remain the treatment of choice in these countries (including Myanmar, Cambodia, Thailand, Vietnam and Laos), which are now thankfully very uncommon sources of imported malaria in Australians.7,9
Practical considerations for malaria treatment and prevention in Australia
Although there are now at least five different WHO-approved ACTs in use worldwide, only one of these, artemether-lumefantrine, is registered for use in Australia. So the choice for Australian GPs is relatively simple. Artemether-lumefantrine can be the initial treatment in nonpregnant individuals for nonsevere malaria due to any species – including P. falciparum, P. vivax, P. ovale, P. malariae and the newly discovered monkey malarias such as P. knowlesi – from anywhere in the world.10 It appears to have no major issues around safety or tolerability so, if there is any doubt about the diagnosis, the risk-benefit balance probably favours early empiric treatment rather than a wait-and-see approach. The only important consideration is that it should always be co-administered with fatty food or drink (a small amount of cow’s milk is fine) to ensure adequate absorption. Although patients may feel much better within 24 hours, it is important that the full three-day six-dose course be taken to ensure all parasites in the body are killed so that the disease does not relapse.
When does the ‘one-size-fits-all’ approach not apply?
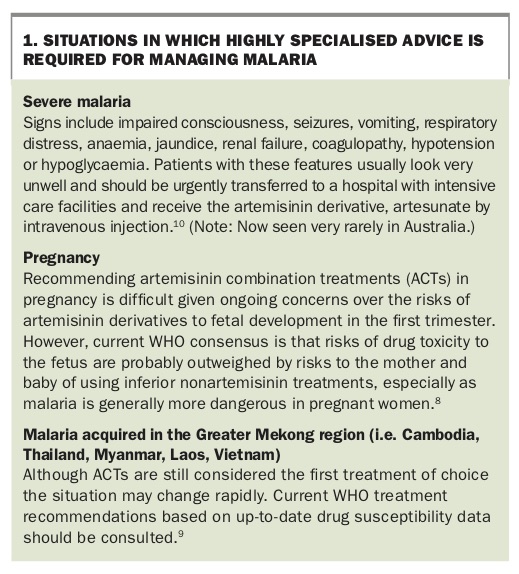
Although artemether-lumefantrine will be appropriate for almost all malaria cases seen in Australia, there are a few important exceptions that can be encountered on rare occasions and that should merit specialist advice (Box 1).
{kind=link}
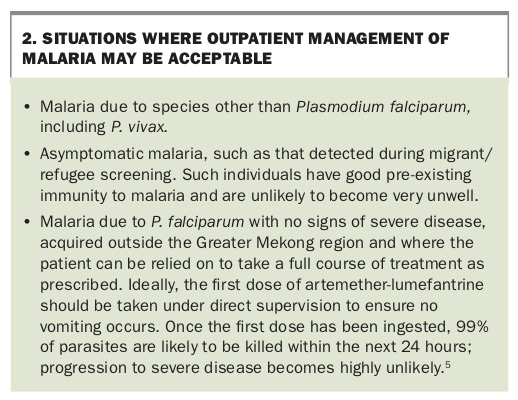
When is it safe to administer treatment as an outpatient?
For many years there has been a prevailing dogma, especially among infectious diseases physicians, that all cases of malaria due to P. falciparum should be admitted to hospital for at least 24 hours.11 However, with the availability of much safer and more rapidly effective artemisinin drugs, this might not always be strictly necessary (Box 2). It should also be noted that in parts of the Northern Territory and far North Queensland where the Anopheles mosquito is endemic, there is a public health imperative to prevent patients from transmitting their parasites to the local mosquito population – which could theoretically result in reintroduction of malaria to Australia. Therefore patients with malaria in these regions should always be admitted to hospital, nursed indoors during the initiation of treatment and receive adjunctive treatment with primaquine, which kills the gametocyte forms of the parasite that are infective to mosquitoes.10
{kind=link}
How can relapse be prevented in malaria due to P. vivax and P. ovale?
These malaria species are problematic because their life cycle includes sleeping hypnozoite liver stages that are not susceptible to most drugs (including ACTs) and that can cause multiple future relapses of malaria. Due to epidemiological changes, especially in our own Asia-Pacific region, these species now account for almost half of our imported malaria cases (Figure 2).6 Unfortunately the one currently available drug able to kill hypnozoites – primaquine – can cause serious haemolytic anaemia in G6PD-deficient individuals therefore mandating pre-treatment G6PD testing. It has also recently been recognised that individuals with certain genetic variations in drug metabolism (e.g. some cytochrome P450 2D6 genotypes) fail to metabolise primaquine to the active compound and are prone to treatment failure.12 This probably effects about 10% of Caucasians but possibly much higher proportions of people from Asian backgrounds. Pre-treatment genetic testing that could predict treatment responsiveness is not yet widely available. Risks of primaquine treatment failure are also compounded by difficulties ensuring compliance with recommended 14-day treatment courses, which can lead to further relapses occurring, even many months after the initial illness.
Who should be offered antimalarial prophylaxis?
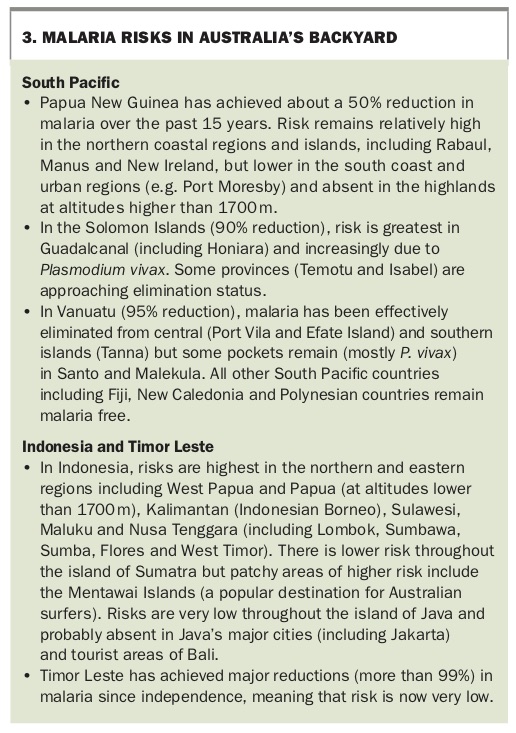
The current epidemiology of imported malaria in Australia suggests that antimalarial prophylaxis be considered in travellers to sub-Saharan Africa, Papua New Guinea, India and Indonesia. Further information regarding malaria risks in the Indo-Pacific region is provided in Box 3. As malaria control continues to improve throughout most of the world, the diminishing risks of acquiring malaria are progressively being outweighed by the small risks of side effects from prophylactic drugs. For example, it is becoming increasingly difficult to justify chemoprophylaxis in most tourists visiting Southeast Asian countries (with the possible exception of Myanmar) except where extensive travel in remote wilderness areas is planned. The three main choices for prophylaxis remain doxycycline, atovaquone-proguanil and mefloquine. The latter has been the subject of ongoing media attention regarding its potential for neuropsychiatric side effects.13 Although these risks have probably been over-stated, mefloquine should generally be considered a ‘third-choice’ for prophylaxis and even then only reserved for relatively high malaria-risk settings such as sub-Saharan Africa.13
{kind=link}
GP resources for advice on malaria treatment and prophylaxis are provided in Box 4.
{kind=link}
It is important to remember that preventing mosquito bites (especially with DEET-containing repellent and appropriate clothing) remains at least as effective for malaria prevention as chemoprophylaxis. Although malaria is waning, other mosquito-borne pathogens are on the rise, including dengue, chikungunya and zika viruses. The current situation therefore suggests we should be de-emphasising malaria prophylaxis and placing greater emphasis on mosquito-bite prevention, which, if practiced appropriately, can protect against a wide range of diseases in addition to malaria.
Conclusion
The improvement we have seen in the number of imported cases of malaria in Australia is a salient example of how, in an increasingly interconnected world, changes in disease control in developing countries can have direct implications to health and medical practice in Australia. The current pace of change is rapid, with high-level political commitment to achieving complete malaria elimination in the Asia-Pacific region within the next 12 years and encouraging progress in many other countries.14 Whether this very ambitious timeline is feasible remains to be seen. History suggests that our gains in malaria control are fragile and could be rapidly reversed, especially if complacency sets in and political commitment falters. The spectre of drug resistance is an ever-present threat that, if unchecked, could undermine recent achievements. However, we can still hope that one day soon we may see malaria treatment going the way of smallpox vaccination. MT