An elderly woman with a hand rash and chest wall lesion

Test your diagnostic skills in our regular dermatology quiz. What is the cause of this painful condition affecting an elderly patient?
Case presentation
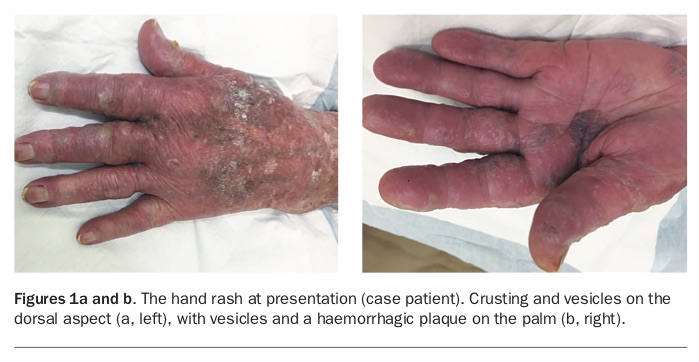
A 96-year-old left-handed woman presents with a three-day history of an intensely painful vesicular rash of the left hand (Figures 1a and b). She also has an isolated chest wall pustule with an erythematous base (Figure 2).
{kind=link}
{kind=link}
The hand rash extends to the radiocarpal joint and includes both dorsal and volar aspects. Some of the vesicles have coalesced, and there is a haemorrhagic plaque on the palm. Crusting is noted on the dorsal aspect. There are no left hand nail changes noted at assessment and the right hand is unaffected.
The chest wall lesion is noted on the patient’s left anterior chest wall over the fifth rib area. The erythematous lesion appeared at a similar time to the hand changes and is painful to light touch.
The patient has previously suffered from hand dermatitis, and she has gout (controlled with allopurinol). Four weeks previously, she had a skin biopsy from the dorsum of the affected hand (for a suspected, and later confirmed, actinic keratosis). At presentation, there was an incidental finding of a markedly elevated white cell count with a predominance of lymphocytes. The patient was subsequently referred to haematology outpatients and diagnosed with chronic lymphocytic leukaemia (CLL).
The patient has had no recent medication changes and no newly introduced soaps or detergents. She does not have any signs of oral or mucosal changes. There is no associated itch, lymphadenopathy, arthritis, cough, diarrhoea or signs of systemic compromise on general examination.
Differential diagnoses
Conditions to consider among the differential diagnoses include the following.
- Contact dermatitis. Contact dermatitis should be considered in any patient presenting with a vesicular rash to the dominant hand. The term contact dermatitis implies an inflammatory skin reaction to an external stimulus, either as an allergen (a type IV delayed hypersensitivity reaction on exposure and subsequent re-exposure to the specific allergen) or irritant (which would occur in any person sufficiently exposed to certain chemicals). Classically, the exposure is occupation related, with florists, hairdressers and cleaners suffering hand rashes from direct handling of certain substances, such as plant material, hair dyes and detergents. The case patient is retired but a history of gardening should be sought. There is no specific mention of irritants or allergens in her history, and a hand rash may be expected to be bilateral if acquired in everyday life. Contact dermatitis by handling substances would not explain the chest wall lesion but can produce erythematous and vesicular lesions such as those shown.
- Staphylococcal infection of the biopsy site. The possibility of acute infection should be considered. The case patient had a biopsy taken from the dorsum of her affected hand four weeks previously – this raises the possibility of biopsy site infection, which would explain the unilateral presentation. Issues are relatively common after skin biopsy, with research suggesting wound complications in 29% of biopsies.1 Infection is the most common complication and Staphylococcus aureus is the most common bacterium isolated from infected wound swabs. The case patient’s age, immunocompromised state and lack of antibiotic cover raise the risk of wound infection. However, although S. aureus can cause erythema, blisters and vesicles that crust, as described, the timescale involved makes a wound infection less likely. There would also be a nidus of infection around the original biopsy site and evidence of delayed healing secondary to this infection. Furthermore, there is no mention of systemic features of infection, axillary lymphadenopathy or increased temperature at the site.
- Sweet syndrome. This unusual disorder, also known as acute febrile neutrophilic dermatosis, should be considered due to the following: an elevated white cell count; tender, oedematous papules and plaques with a violaceous colour; and multiple vesicles, in an asymmetrical pattern. The presence of a haematological malignancy (CLL) also raises the suspicion. In this case, however, biopsies were negative, the patient was afebrile, and the elevated white cell count was due to lymphocytes rather than neutrophils.
- Dermatomal herpes zoster. This is the correct diagnosis. The rash was hyperalgesic, and had a classic vesicular appearance, with surrounding erythema and crusting. Immunohistochemical tests on biopsies taken from the lesions were positive for varicella zoster virus and microscopy of the cells demonstrated cytoplasmic and nuclear viral inclusions. This case demonstrates how dermatomal diseases may not follow the textbook definitions of well-demarcated areas, with this particular eruption affecting several dermatomes (C6,7,8 [hand] and T1 [chest wall]). There is a strong link between herpes zoster and increasing age. Furthermore, immunosuppression, such as coexisting CLL, will also increase the risk of developing the disease, especially multidermatomal disease. The condition is very common, with a lifetime incidence of one in three (www.cdc.gov/shingles/surveillance.html), and should be considered early on for a patient with a unilateral erythematous crusting rash.
Management
Herpes zoster is extremely painful because it involves the reactivation of viral replication within sensory ganglia. Treatment therefore centres around antiviral therapy and analgesia. The goals of treatment are to expedite healing of the vesicles and to decrease the duration and intensity of the acute neuritis. An example of a recommended regimen may be oral valaciclovir (1000 mg three times daily for seven days), paracetamol (1 g four times daily) and ibuprofen (400 mg three times daily), with stronger opioids such as oxycodone to be added if required.2 Oral famciclovir is an equally effective and cheap alternative to valaciclovir. Oral aciclovir is less convenient as it requires more frequent dosing.
There is strong evidence that antiviral therapy reduces the duration and intensity of acute neuritis.3-5 When started within 72 hours of the onset of herpes zoster there is a likely benefit of reduced overall intensity of pain.6 Starting antiviral treatment after the initial 72 hours is recommended if new lesions are still emerging, as this would suggest ongoing viral replication.7 However, our case patient is immunocompromised due to CLL, and therefore treatment should be started regardless of time of onset because there is a significant risk of disseminated infection that can lead to sequelae such as hepatitis or encephalitis. In this instance, hospital admission for intravenous aciclovir would be appropriate.
Ongoing pain at the site of cutaneous eruption is very common long after the rash disappears. Postherpetic neuralgia is defined as pain that persists for longer than four months after the onset of the initial rash.8 Gabapentin, pregabalin and tricyclic antidepressants (off-label use) are currently first-line treatments.9-11 Caution is required when using tricyclic antidepressants in elderly patients because of anticholinergic effects.
This case demonstrates the importance of shingles vaccination in the elderly and in immunocompromised patients. The Australian Government currently recommends and funds the vaccine through the National Immunisation Program for adults at 70 years of age, with a catch-up program available for those aged 71 to 79 years until 31 October 2021 (https://beta.health.gov.au/services/shingles-herpes-zoster-immunisation-service). MT
Acknowledgement
The authors acknowledge the assistance of Dr Mark Aldred in preparation of the manuscript.