When migraine becomes more than a pain in the head

A 14-year-old boy presents with a history of migraine and a constant dull headache. A multimodal approach is required to ensure there is no sinister cause for his pain and that he is managed appropriately.
Case scenario
Lachlan, a 14-year-old boy, began having occasional migraines, generally during school hours, when he was 12 years of age. He is now averaging one severe migraine every two to four weeks and has a dull headache on most days. He has a family history of migraine and background stress. Lachlan is attending counselling and being treated for depression with the selective serotonin reuptake inhibitor (SSRI) fluoxetine. What investigations should be considered in a patient such as Lachlan? Does medication for an adolescent patient differ from that for an adult with recurrent migraines?
Commentary
Headache is a common presentation in children and adolescents. The differential diagnoses of paediatric headache are broad and dependent on the co-presenting symptoms and signs. Common causes of headache include:
- localised infections (e.g. upper respiratory tract infections)
- inflammation (e.g. allergic rhinitis)
- tension headache
- migraine.
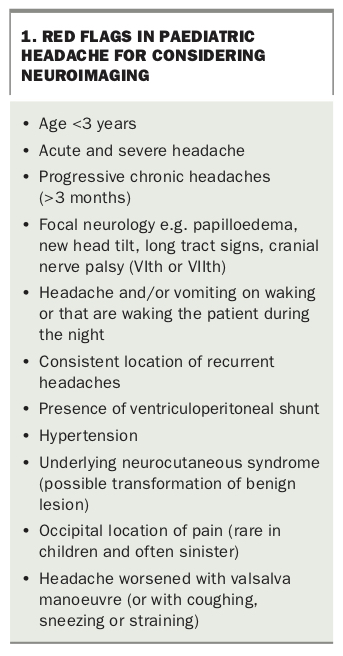
Less common but serious causes of headache include infections of the central nervous system, space-occupying lesions and other causes of raised intracranial pressure. Ensuring a patient’s blood pressure is normal for age is crucial and often overlooked. Establishing that the headache is due to migraine (or another primary headache syndrome) and is not a secondary symptomatic headache (e.g. vasculitis, tumour, raised intracranial pressure, meningitis) is an important consideration during the early time course. Parents are often anxious that the cause of the headache is sinister (e.g. brain tumour) and therefore assessing the likelihood of this diagnosis based on the presenting history and physical examination findings is a priority. Awareness of the ‘red flags’ during assessment can promote early and prompt referral for neuroimaging and/or specialist review if they are present (Box 1).
{kind=link}
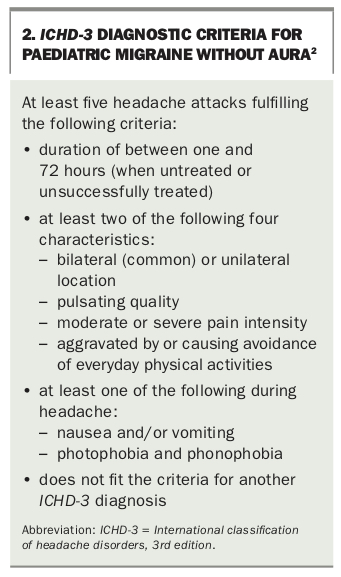
Migraine headache is common in the paediatric population, occurring in 7.7% of children and adolescents.1 Migraine is one of the most common reasons for referral to a paediatric neurologist. Establishing a diagnosis of migraine headache can be relatively straightforward if the child’s or adolescent’s symptoms fulfil the diagnostic criteria from the International classification of headache disorders, 3rd edition (ICHD-3; Box 2).2 Other clues to the diagnosis of migraine include a positive family history, a chronic recurrent time course and a normal physical examination.
{kind=link}
Classifying Lachlan's headache
In the case scenario, Lachlan is 14 years of age (postpubertal) and has an established diagnosis of migraine headache, made when he was 12 years of age. There is a family history of migraine, which is supportive of the diagnosis given that up to 80% of children with migraine headache have a positive family history.3
Lachlan’s current presentation is of acute-on-chronic headache. His migraine headaches have deteriorated, and he is described as having one to two severe migraines per month. It can be assumed that the character and location of these more severe headaches are like those he experienced in the past. In addition to this, Lachlan is describing a dull headache on most days. Given this combination, it is likely that Lachlan has transformed migraine, which is a migraine condition that typically begins with episodic migraine attacks that become more frequent over a period of months to years. Transformed migraines are usually a mixture of tension-type headaches and migraine attacks and they tend to occur daily or almost daily.
Investigations for paediatric headache
Investigations in children presenting with headache are often conducted early in the time course of presentation. Generally, paediatric patients are screened with baseline blood tests including a full blood count, iron studies, liver function tests and measurement of electrolyte, urea and creatinine levels. This is important as there are many systemic causes of headache that are treatable and reversible. If there is a strong family history of autoimmune conditions (e.g. coeliac disease, hypothyroidism) then it may be important to screen for these conditions also. Once a child has been reviewed over several months or years, investigations become less relevant unless a red flag evolves over time (Box 1). Neuroimaging is recommended early if there are red flags identified during the initial assessment of a patient.
Lachlan has a diagnosis of migraine headache with an acute increase in the severity of his migraine episodes. Although increasing severity of a headache can be a red flag, the duration and time course of Lachlan’s headache (over two years) makes a sinister cause to this exacerbation unlikely. Providing his examination is unchanged (still normal), the chance of finding a significant abnormality in a child or adolescent such as Lachlan with headache symptoms that meet the diagnostic criteria for migraine headache and no red flags is low. Neuroimaging is generally not recommended in this group.2
The complicating factor with many paediatric patients is that their parents are often anxious that a sinister cause is being ‘missed’ or their concerns are being ignored. This can lead to a neuroimaging request and unfortunately, not uncommonly, the MRI scan of the child is found to be abnormal. This heightens parental anxiety further even if the findings are nonspecific or benign. The literature estimates that up to 46% of all patients with migraine headache have small nonspecific hyperintensities in the deep white and periventricular white matter on T2-weighted MRI brain scans.4 However, there can be positive aspects to requesting a scan; once neuroimaging is performed and no sinister cause of headache has been found, parents are more open to a holistic management plan including lifestyle modifications, psychological help and medication.
Although Lachlan does not need neuroimaging based on his history and assuming his examination is normal, part of managing children and adolescents is also addressing the anxiety in parents, which can sometimes be futile to attempt without performing a scan.
Treatment options for an adolescent patient with recurrent migraines
Lachlan has transformed migraine. He previously did not require prescription medications for either acute exacerbations or as preventive measures; however, given he now has transformed migraine a different approach may be needed.
Determining the management approach that is needed in a child or adolescent with migraine depends on two main factors:
- the frequency of migraine episodes experienced per month
- the functional impairment caused by the episodes themselves.
Box 3 summarises the expert consensus statement of the US Headache Consortium that proposed a tiered-treatment approach to determining if preventive migraine management is needed.5 In addition to this, consideration must be given to the psychosocial aspects of the patient’s care.
{kind=link}
The following approach would generally be recommended.
- Lifestyle modifications. These can include appropriate sleep hygiene and habits, adequate hydration, consumption of well-balanced meals (not skipping breakfast), exercising three to four times per week and stress avoidance or management. These measures may help decrease the frequency of headache with the added benefit of conditioning the body to better cope with headache episodes as they arise.
- Nonpharmacological pain management. Given that pain can be cultural, psychological, physical, emotional or spiritual, an assessment with a clinical psychologist can identify specific triggers and offer cognitive behavioural therapy, biofeedback therapy and stress-management techniques. Mainstream physical therapy, as well as alternative therapies such as yoga or pilates may be trialled providing they are not costly or harmful. A trial of vitamin B2 and magnesium supplements can be suggested, but studies on their efficacy are not strong.
- Acute and preventive management. First-line therapy for acute management of migraine is typically an NSAID such as ibuprofen. Aspirin-containing products should be avoided in children under the age of 16 years to avoid the risk of developing Reye’s syndrome.6 Other therapies include paracetamol (less effective than ibuprofen) and naproxen. For acute and severe presentations of migraine headache, several studies have shown that triptans (e.g. sumatriptan, zolmitriptan) are safe and effective in the acute treatment of migraine in adolescents.7 This parallels the recommendations for acute migraine management in adults. There is less evidence for preventive therapies in paediatric patients with migraine. Where studies in adults with migraine show a clear benefit in several antimigraine medications, the same is not true of paediatric studies, which are either nonexistent or have shown conflicting or negative results. There are also high rates of placebo effect in paediatric studies. The optimal pharmacological treatment of migraine in children and adolescents is still unclear. The general recommendations are therefore to approach management of children and adolescents with multimodal care encompassing lifestyle, nonpharmacological and pharmacological management. Once initial measures have been implemented and at least one medication has been considered, it is advisable to refer the child or adolescent for specialist review.
Outcome
Lachlan has several psychological factors that are likely contributing to his headache presentation including stress and depression. He is already attending counselling and has been prescribed an SSRI. Exploration of factors that could be contributing to his current level of impairment are important.
Given that Lachlan is having acute episodes of severe migraine, a trial of a triptan (e.g. sumatriptan nasal spray or tablets) at the onset of a migraine headache would be recommended in addition to ibuprofen. Depending on how long he had been experiencing it before his presentation, the dull ache that is present on most days may improve with lifestyle measures and nonpharmacological management for a short period.
If Lachlan continues to have a daily headache and frequent exacerbations despite a multimodal approach, then trialling one or two of the antimigraine medications that have shown benefit in adults (e.g. tricyclic antidepressants [off-label use], topiramate, beta blockers) should be considered, providing that contraindications are not present (e.g. asthma for beta blockers) and that his family are aware that evidence for their efficacy in the paediatric population is lacking and that it is potentially an off-label use. A trial of at least eight weeks is recommended unless side effects are intolerable.
Conclusion
Migraine is a common cause of headache in the paediatric setting. Providing the examination and history do not show any red flags, it is generally safe to manage the symptoms in general practice. A multimodal approach to management is recommended. MT