Closing the gap for women with coronary artery disease

Cardiovascular disease (CVD) remains the leading cause of death among women. Important sex differences in CVD risk factors, pathophysiology, presenting symptoms, treatment, preventive strategies and outcomes are increasingly recognised. More focus on female-specific features of CVD might help the development of targeted therapeutic interventions for both primary and secondary prevention in women.
- Chest pain is the most common symptom of an acute coronary syndrome in both women and men.
- Women with acute coronary syndromes have more associated symptoms (fatigue, breathlessness, nausea, dizziness and abdominal discomfort), which may distract from the diagnosis.
- The traditional cardiovascular risk factors of diabetes, smoking and inactivity increase the risk of cardiovascular disease in women more than they do in men.
- Women can have nontraditional cardiovascular risk factors such as gestational diabetes, gestational hypertension, pre-eclampsia and polycystic ovary syndrome.
- Women are less likely to receive guideline-directed treatment for primary and secondary prevention of cardiovascular disease.
Cardiovascular disease (CVD) remains the leading cause of morbidity and mortality among women worldwide. CVD accounts for one-third of all deaths among women, with more women than men dying annually from CVD.1,2 Potential contributors to this gender gap include greater variation in symptoms among women with CVD, which may delay presentation and treatment, and differences in management between women and men. The recognition of sex-specific risk factors for CVD among women raises questions about the practical utility of traditional cardiovascular risk scores in the female population. Female under-representation in clinical trials limits the evidence base for many cardiovascular treatments used in both sexes.
This review discusses important sex differences in risk stratification, diagnosis and treatment of coronary artery disease. It outlines strategies to help close the current gender gap in CVD outcomes.
Burden of cardiovascular disease in women in Australia
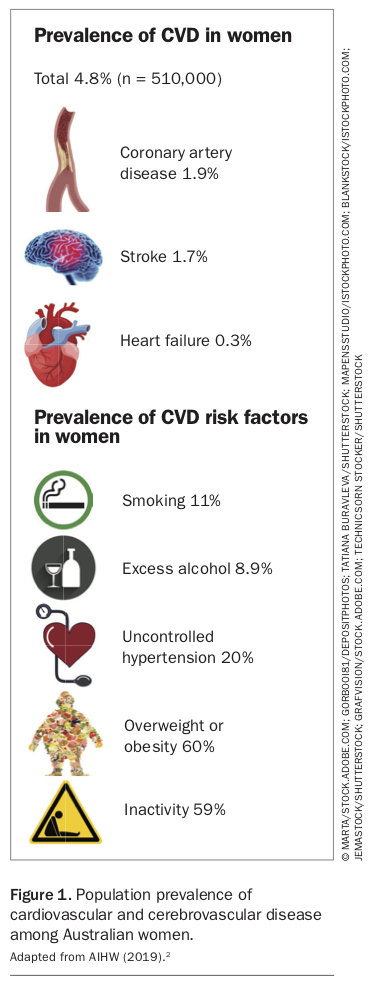
Advances in evidence-based cardiovascular therapies have reduced mortality over time. As a result, an increasing proportion of the Australian population are living with CVD, including more than 510,000 women (4.8%) in 2018.2 The population prevalence of cardiovascular and cerebrovascular disease among women in Australia is shown in Figure 1.2
{kind=link}
As female life expectancy continues to increase, so too will the burden of CVD and concurrent comorbidity.1 In addition, CVD has a significant impact on younger women, accounting for 8.4% of deaths among women younger than 45 years.2 As well as those with established CVD, a large proportion of women are at risk of CVD and are candidates for primary prevention. In 2016, 14% of Australian women aged between 45 and 74 years were deemed to be at high risk, and 2.9% (108,000) at moderate risk of experiencing a cardiovascular event within five years.3
However, the vast proportion of women with or at risk of CVD do not receive guideline-recommended therapies. Recent studies showed that 52% and 37% of women do not receive guideline-recommended lipid-lowering and antihypertensive pharmacotherapies, respectively.2,4 Moreover, women who develop an acute coronary syndrome are less likely to undergo invasive coronary angiography or to receive complete coronary revascularisation and guideline-directed medical therapy than men with an acute coronary syndrome.5-7
Women presenting with an acute coronary syndrome are more likely to have nonobstructive coronary artery disease, manifesting as coronary microvascular dysfunction, plaque erosion, thrombus formation and coronary vasospasm.8 Other causes of myocardial injury with a female predominance include coronary microvascular dysfunction, spontaneous coronary artery dissection and myocardial infarction with nonobstructive coronary arteries (MINOCA). Other cardiac conditions with a recognised female predominance include Takotsubo cardiomyopathy, peripartum cardiomyopathy and heart failure with preserved ejection fraction (HFpEF, also known as stiff heart syndrome). To date, management strategies for these conditions remain relatively limited.
Risk factors for coronary artery disease
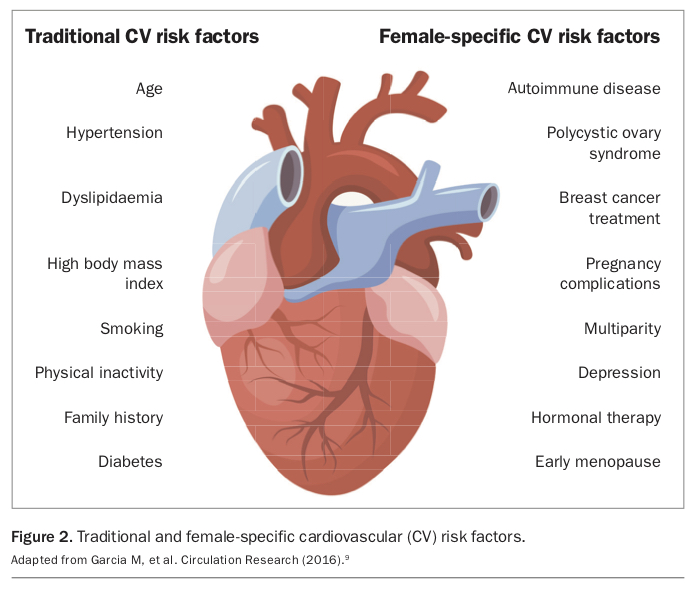
It is increasingly recognised that risk factors for CVD in women include traditional risk factors affecting both sexes and also female-specific risk factors (Figure 2).9
{kind=link}
Traditional cardiovascular risk factors
Conventional modifiable and non-modifiable risk factors are common contributors to CVD among both women and men. Nonmodifiable risk factors include age and family history of premature coronary artery disease. Modifiable risks pertain to lifestyle factors (smoking, excess alcohol use, substance use and inactivity) and comorbidities (diabetes, hypercholesterolaemia, hypertension, metabolic syndrome, chronic kidney disease and obesity) which promote atherogenesis.9 Certain traditional risk factors confer a higher risk of adverse cardiovascular outcomes in women.
Smoking
Although fewer women smoke overall, active female smokers have a 25% greater risk of developing coronary artery disease than male smokers across all age groups.10 Oral contraception has a synergistic effect on smoking, increasing the risk of acute myocardial infarction, stroke and venous thromboembolism.9
Obesity
Weight gain in adulthood leads to an incremental increase in atherosclerotic cardiovascular risk factor burden. The impact of obesity on coronary artery disease in women differs from that in men. Obese women have a relative risk increase in CVD of 64% compared with a 46% increase in obese men.11
Hypertension
Female sex does not influence the clinical sequelae of systemic hypertension; however, blood pressure optimisation is achieved less often in women, particularly in older women. In the over 80 years age group, only 23% of women achieved and maintained guideline-recommended targets compared with 38% of men.12
Diabetes
Women with diabetes have a higher burden of atherosclerotic risk factors (including metabolic syndrome, hypercoagulable state and endothelial dysfunction), with a higher risk of developing CVD (relative risk 44%), fatal coronary artery disease, stroke, heart failure and cardiovascular mortality than men with diabetes.9
Dyslipidaemia
Dyslipidaemia poses the greatest population-adjusted risk among the traditional atherosclerotic cardiovascular risk factors (47.1%). Women are less likely to be prescribed and adhere to statins. However, women who take statins derive the greatest benefit with regard to LDL-cholesterol lowering and atheroma regression.9
Emerging sex-specific cardiovascular risk factors
Women have unique, nontraditional risk factors that contribute to their cardiovascular risk profile. These are observed at key life stages when hormonal and physiological changes are most prominent (Box).
{kind=link}
Premenopausal risk factors, including pregnancy-related factors
Sex hormones play an important role in modulating vascular and cellular activities. The hormonal shifts seen in women with polycystic ovary syndrome and those taking oral contraceptives or hormonal therapies for breast cancer can influence blood viscosity, promoting thrombogenesis and atherosclerosis. Systemic inflammation mediated by autoimmune and rheumatological conditions can promote platelet activation, plaque formation and erosion.3,13
Pregnancy has a substantial physiological impact on the maternal cardiovascular system. The lifetime cardiovascular risk is increased in women with pregnancy-related complications such as pre-eclampsia and gestational diabetes or with more than one pregnancy.14,15 One in three women experience pregnancy-related complications, including hypertensive disorders of pregnancy, pre-eclampsia, gestational diabetes, miscarriage, still birth, preterm birth, low birthweight and placental abruption. Pregnancy complications tend to precede manifestations of traditional cardiovascular risk factors and provoke neurohormonal adaptations with a heightened (60 to 75%) long-term risk of developing CVD.16 The American College of Obstetricians and Gynecologists and the American Heart Association recommend interdisciplinary care and cardiovascular risk assessment and surveillance of these women in the postpartum years.17,18 However, no similar Australian guidelines have been established.
Postmenopausal risk factors
The antiatherogenic and lipid-regulating effects of oestrogen appear to be a key cardioprotective mechanism in premenopausal women. Low circulating oestrogen levels are implicated in the accelerated progression of atherosclerosis and higher prevalence of cardiovascular events observed in postmenopausal women.19 In general, the prevalence of acute myocardial infarction and sudden cardiac death remains low in premenopausal women. However, a sharp increment (threefold increase) in CVD prevalence and severity is observed in postmenopausal women.9,19
Presentation of coronary artery disease in women
Women with coronary artery disease tend to have a higher risk factor burden and to manifest symptoms later in life (on average seven to 10 years later) than men. Women with acute coronary syndromes, particularly when diagnosed at a younger age, have a worse prognosis than men.20
Historically, higher rates of atypical chest pain symptoms have been described in women.21,22 However, recent evidence has shown that typical ischaemic chest pain is the predominant presenting symptom in 90% of both women and men.23,24 However, women have more associated symptoms, including fatigue, shortness of breath, nausea, dizziness and epigastric or back pain.23 These additional symptoms may distract from the correct diagnosis. The resultant ‘atypical chest pain’ label may in part explain the finding that women with heart attack symptoms are 50% more likely to be misdiagnosed on initial assessment than men.23,25
Moreover, younger women presenting with typical symptoms and an acute coronary syndrome may have non-atherosclerotic coronary disease, such as spontaneous coronary artery dissection. This compounds diagnostic errors, with potentially catastrophic consequences.
Diagnostic work up: which tests should I order?
Asymptomatic women
The management of asymptomatic individuals has two key objectives: risk factor modification and risk stratification. Risk factor modification, primarily managed in the community by GPs, involves:
- blood pressure optimisation
- smoking abstinence
- exercise
- weight reduction (where relevant)
- stress management
- dietary modification.26
These measures, if addressed early, can halt, slow or prevent the development of heart disease.
The introduction of the ‘Heart Health Check’ MBS item in April 2019 enables access to a comprehensive cardiovascular risk assessment recommended by a GP and rebated under Medicare.27 The Heart Health Check is recommended for individuals aged 45 years or over (30 years or over for Aboriginal or Torres Strait Islander people).
Risk stratification
Risk stratification involves assessing for symptoms, cardiovascular risk factors (both traditional and nontraditional) and comorbidities that amplify cardiovascular risk to estimate the pretest probability of coronary artery disease. Conventionally, risk stratification has used validated risk scores that rely on traditional cardiovascular risk factors and do not factor in sex-specific or genetic factors. These scores may misclassify individuals, particularly women, with nontraditional risk factors (such as pregnancy complications, autoimmune conditions and genetic factors) as low risk. Nontraditional risk factors must be considered in addition to traditional cardiovascular risk factors when evaluating overall cardiovascular risk and should prompt further testing.
Calcium scores in women
CT coronary artery calcium (CAC) scoring is a noninvasive, quantitative method of estimating coronary artery calcification in asymptomatic patients, providing additional data to traditional risk calculators. Traditional risk scores often underestimate cardiovascular risk in women; CAC scoring may add incremental information and enhance overall cardiovascular risk assessment.
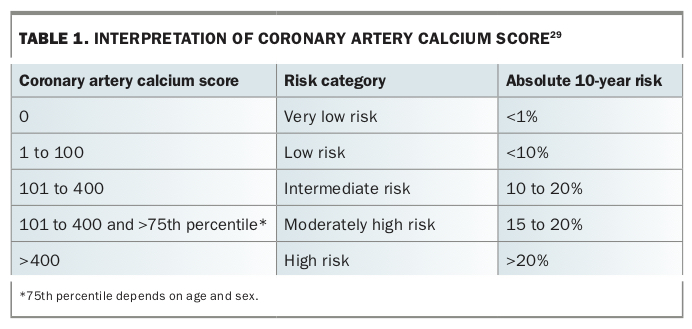
The CAC score has been shown to be an independent predictor of future cardiovascular morbidity and mortality.27 CAC scoring has the greatest yield in stratifying intermediate-risk individuals (absolute 10-year cardiovascular risk 10 to 20%) who are asymptomatic, aged 45 to 75 years and have no known coronary artery disease, potentially reclassifying individuals as either low or high risk.27,28 CAC scoring may also be considered in low-risk individuals (absolute 10-year risk 6 to 10%), particularly when conventional risk scores underestimate the risk, such as in those with a family history of premature coronary artery disease and sex-specific nontraditional risk factors.27
Interpretation of the CAC score is shown in Table 1.29 Asymptomatic individuals with a CAC score above 100 should undergo aggressive risk factor modification, focusing on blood pressure optimisation, lipid-lowering measures (including statins), weight loss and lifestyle measures.
{kind=link}
CAC is not currently Medicare-rebated, with a cost involved for the patient, reinforcing the importance of careful consideration of its role according to the patient’s risk. The radiation exposure, although low (equivalent to two breast mammograms), should also be considered in the decision to recommend CAC scoring, particularly in young women.28
Symptomatic women
Patients presenting with persisting or unstable symptoms that are potentially acute coronary symptoms should be referred urgently to hospital for troponin testing, ECG and a chest x-ray to investigate for possible myocardial ischaemia. Further investigations will depend on clinical signs and symptoms. Routine troponin testing in the community setting is not recommended.
The introduction of a high-sensitivity cardiac troponin assay allows better detection of myocardial ischaemia with sex-specific cut-offs with greater specificity.30
Clinical features supporting a likely diagnosis of an acute coronary syndrome include ECG changes, troponin elevation or ongoing symptoms suggestive of ischaemia. In these cases, inpatient investigations with invasive coronary angiography are usually appropriate.
In the absence of ongoing symptoms and objective markers of ischaemia, patients may be referred for outpatient testing. Treadmill exercise testing is a universally available and noninvasive test that provides useful information regarding inducible ischaemia and functional capacity and is a useful prognostic indicator for cardiovascular morbidity and mortality.30
Women have a higher rate of false-positive results on treadmill stress testing (up to 40% false-positive rate) than men.31 False-positive results may lead to significant psychological stress and invasive assessments. The specificity of treadmill stress testing is increased by concurrent echocardiography.
Stress imaging can be used when the baseline ECG is abnormal (i.e. left bundle branch block or left ventricular hypertrophy). It involves either stress echocardiography (exercise or dobutamine) or nuclear thallium testing. Chemical provocation is particularly useful in individuals with compromised mobility or exercise capacity, providing there are no contraindications.
CT coronary angiography is emerging as a more widely acceptable alternative to functional testing. It may be of particular use in younger patients and women, because of its greater sensitivity compared with stress imaging and the high false-positive result rate with treadmill stress testing.32-34 CT coronary angiography also provides valuable information on coronary artery plaque burden and the calcium score that can guide medical therapy decision making.35
A proposed diagnostic algorithm based on risk stratification for patients with chest pain who are troponin negative is shown in the Flowchart.
CT coronary angiography could have an evolving role across all risk groups in assessing and quantifying the burden of coronary artery calcification in patients with stable symptoms.35 The radiation exposure associated with CT coronary angiography is low (less than 2mSv), similar to the radiation dose during CT CAC scoring (0.5 to 1.5 mSv) and significantly less than during a nuclear stress test.28,36,37
Management and outcomes of coronary artery disease in women
Women with obstructive coronary artery disease have an overall worse prognosis than men, driven in part by older age and higher comorbidity burden.38,39 Australian data show that the death rate after a heart attack is up to twice as high in women as in men.6,8 Despite advances in management of acute myocardial infarction, improvements in mortality have been significantly less in women. Younger women in particular remain at high risk of adverse outcomes, with substantial delays in diagnosis and treatment despite their being more likely to present with typical ischaemic symptoms than older women.40-42
Women of all ages with coronary artery disease are less likely to receive guideline-directed therapies, including lipid-lowering and antiplatelet therapy, lifestyle modification advice and specialist follow up. Moreover, when evidence-based treatments are implemented, prescribing practices are less likely to achieve optimal therapeutic targets.3,8,23
In addition, women are less likely to be referred to cardiac rehabilitation programs; however, women who are engaged in cardiac rehabilitation appear to derive similar or greater benefit than men.43 Cardiac rehabilitation in addition to guideline-directed therapy is a fundamental step in optimising outcomes for women with coronary artery disease.
Female under-representation in guidelines and clinical trials
Women remain largely under-represented in cardiovascular clinical trials, comprising fewer than 20% of study participants.44 Management of CVD in women has largely focused on guidelines derived from clinical studies involving predominantly male participants. Although some mechanisms are common to both men and women, sex-specific differences exist in the anatomy and physiology of myocardial function, vascular physiology and hormones.45,46 It is incumbent upon us to encourage female participation and equitable gender representation in clinical trials to better inform future guidelines and establish targeted interventions to optimise cardiovascular care among women.
Women's cardiovascular health: a public health priority
Public awareness of heart disease in women is poor. A National Heart Foundation survey found that only one in five women were aware that heart disease is the leading cause of death among women, and only one in two women felt they could confidently recognise symptoms of a heart attack.47
This finding has led to various interventions to improve heart health awareness in the population in Australia through the National Heart Foundation’s campaign ‘Making the Invisible Visible’, which was inspired by the American Heart Association’s campaign ‘Go Red for Women’.48-50 Initiatives include the inaugural Women and Heart Disease Forum, held in NSW in June 2019, and publication of an annual report on the cardiovascular profile of women in Australia.51
More recently, the Department of Health introduced the Heart Health Check, which encourages Australians to seek advice about their heart health and individualised risk factor care. This is an ideal opportunity for GPs to discuss cardiovascular risk with women who have no known heart disease or stroke. It includes obtaining a history (with the opportunity to identify traditional and nontraditional cardiovascular risk factors), performing an examination including blood pressure measurement, lipid studies and screening for diabetic markers, and instigation of a management plan for any identified risk factors. We recommend performing a Heart Health Check in women aged 45 years or over (30 years or over for Aboriginal and Torres Strait Islander peoples).
GPs and cardiologists have an important collaborative opportunity to mitigate the risk of adverse cardiovascular events by:
- educating women and the general public about heart disease and sex differences
- identifying relevant risk factors
- prescribing guideline-directed pharmacotherapy
- promoting risk factor modification.
Long-term follow up for women with coronary artery disease
Women with established coronary artery disease who have had a cardiac event require long-term follow up that addresses risk factor modification with glycaemic and lipid control and medication management.17 This can be best achieved through a shared-care model involving both the GP and cardiologist, using guideline-based pharmacotherapy and secondary prevention strategies.
Recent studies suggest that women undergo fewer risk factor assessments, are undertreated and report a greater burden of adverse effects from pharmacotherapy, particularly statins. However, the proportion of women who adhere to guideline-directed therapy derive a significant reduction in future cardiovascular events.52,53 Routine surveillance of blood pressure, weight and body mass index as well as lipid profile and glycaemic control are crucial in determining whether risk factors are adequately optimised and in guiding decisions regarding adjustments to pharmacotherapy.54
Contemporary guidelines recommend the use of high-intensity statins in secondary prevention for both men and women because of a significant reduction in mortality in this patient population.54 However, statin intolerance, predominantly manifesting as myalgia, is common among women (up to 20%) and is likely a major contributor to statin nonadherence and discontinuation among women. Despite this, there are inadequate sex-specific disaggregated analyses in previous statin trials to inform sex-specific statin titration.55
Role of the GP
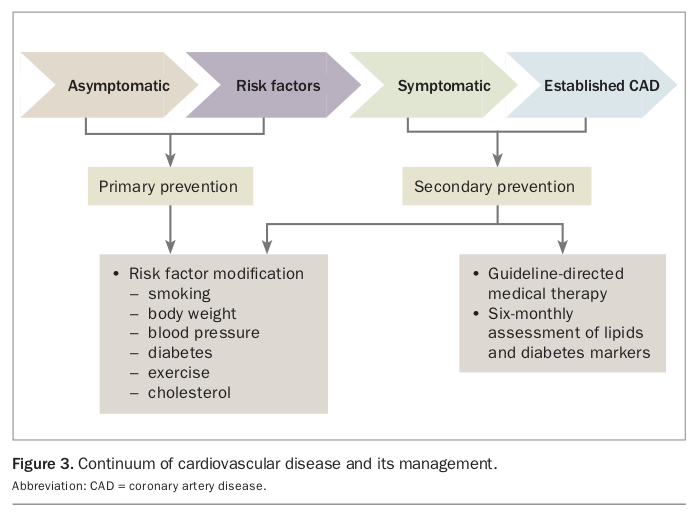
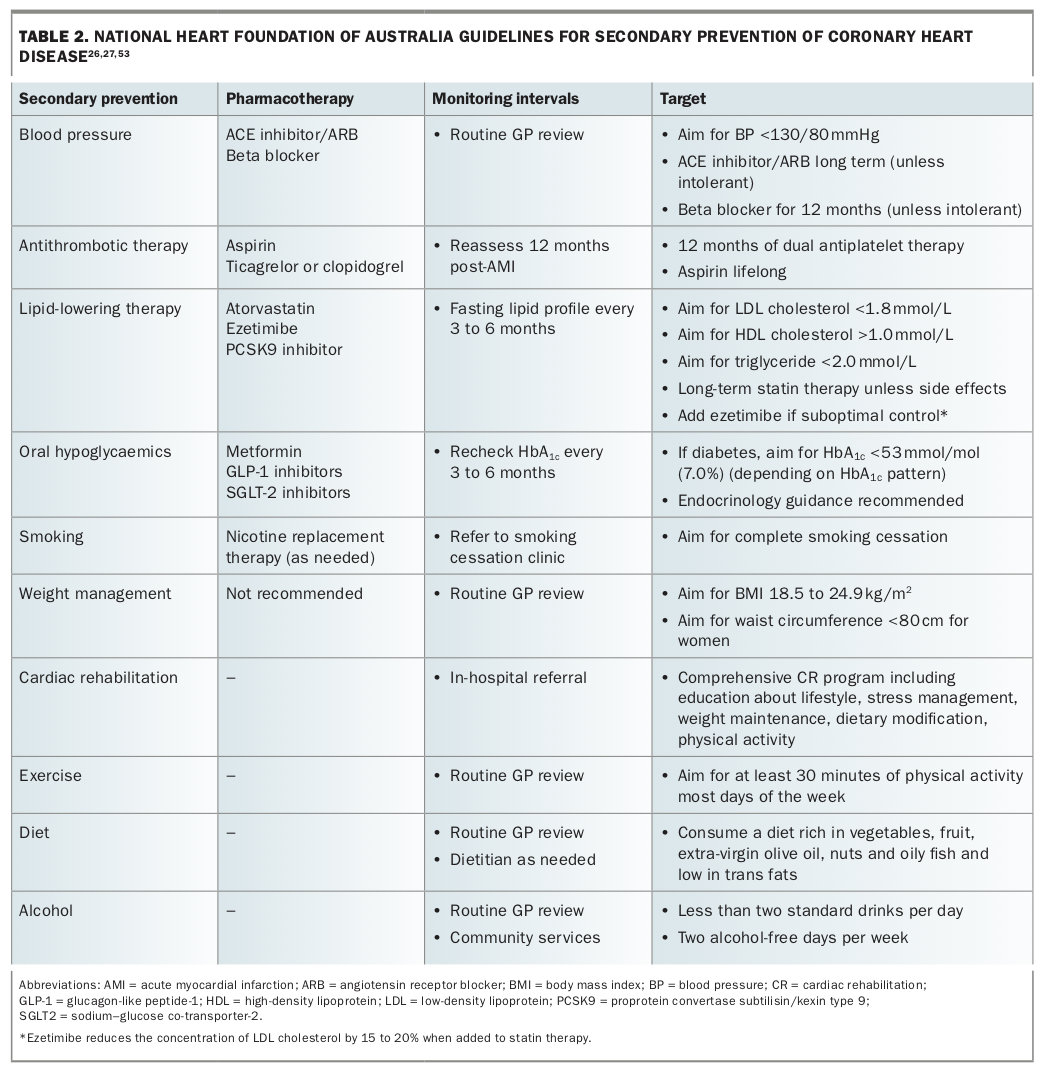
GPs are on the frontline of assessing and managing cardiovascular risk in the broader community. It is imperative that GPs recognise the continuum of CVD, ranging from an asymptomatic preclinical state to established symptomatic of coronary heart disease (Figure 3). GPs play a crucial role in recognising individuals at risk of developing CVD and managing those with established disease. Guidelines for secondary prevention of coronary heart disease from the Heart Foundation are summarised in Table 2.26,27,53
{kind=link}
{kind=link}
Routine patient encounters should prompt assessment of cardiovascular risk factors, including blood pressure, smoking, alcohol intake and weight, and screening for diabetes and hypercholesterolaemia. This is an opportunistic time to intervene and address modifiable risk factors to mitigate the risk of future cardiovascular events. Women who have had a complication of pregnancy such as pre-eclampsia can be assessed for their cardiovascular risk when they return to their GP for routine postpartum follow up.
Patients with established CVD risk factors should receive individualised, targeted advice and pharmacotherapy (where appropriate) to moderate their risk, along with interval monitoring to assess the response to these interventions. Nonpharmacological strategies may include referral to an exercise program, dietitian, smoking cessation clinic, counselling or weight loss program.
Individuals presenting with new symptoms often require specialist cardiology input to assess the need for specific cardiovascular testing and treatments, either in the community when symptoms are stable or in hospital when symptoms are progressive, incessant or unstable. Patients with established coronary artery disease require collaborative management between the GP and cardiologist to reduce the risk of future cardiovascular events. These patients will require review of their pharmacotherapy and close metabolic monitoring (six-monthly HbA1c measurement and full lipid profile) for risk factor optimisation (Table 2).26,27,53
‘Heart centres for women’ are emerging as a way to address the gender gap in cardiovascular care. These centres provide better awareness and focused care for women and address gender disparities in sex-specific research on cardiovascular outcomes.56
Conclusion
CVD remains the leading cause of death among women. Women’s estimated lifetime risk of developing CVD, currently 40%, continues to climb as they accumulate more traditional and nontraditional cardiovascular risk factors. A greater focus on sex-specific differences will facilitate development of targeted therapeutic interventions for both primary and secondary prevention of CVD for women. This requires a coordinated effort between GPs and cardiologists that incorporates sex-specific risk factors and management to improve women’s cardiovascular health outcomes. MT
References
wp-content/uploads/2014/12/2012_HF_CSANZ_Reducing_Risk_in_Heart_Disease.pdf (accessed December 2019).
Absolute_Cardiovascular_Disease_Risk_Assessments_-_A_Guide_For_Professionals.pdf (accessed December 2019).