Contraception in women aged 50 years and over

Contraception can be an important consideration for women aged 50 years and older who have not reached menopause, as unintended pregnancies at this stage of reproductive life can be medically and socially challenging. Determining whether contraception is required and actively informing patients of their options with respect to methods, contraindications, risks and benefits, will help GPs support women in this age group to make an informed choice that best suits their personal circumstances and preferences.
Contraception remains important in avoiding unintended pregnancy until menopause can be established, that is, until a woman has had two years of amenorrhoea if she is under the age of 50 years, or at least one year of amenorrhoea since turning 50. Although pregnancy in women aged 50 years or over is very uncommon and background fertility is low, unintended pregnancies can be problematic at this later stage of reproductive life.1 There is a high rate of miscarriage and fetal abnormality, as well as higher risks of background morbidity that can impact the outcome of a pregnancy.2 Available data indicate that around 16% of pregnancies in women aged 45 years or over end in abortion.3 It is important that GPs actively inform their perimenopausal patients about the risk of pregnancy as women in this age group may underestimate their fertility and be unaware of the need to use contraception. The role of the GP is to determine patient preferences and take a relevant medical and social history in order to provide balanced information on safe and suitable options.
Is contraception required?
In older women, it is important to establish when menopause is reached and if contraception is no longer required. Cessation or continuation of contraception depends on the type of contraceptive being used (Flowchart), in particular whether the method is hormonal or nonhormonal, as well as the woman’s individual circumstances and personal preference.
Women not using hormonal contraception
For women who are not using hormonal contraception, menopause is established after a year of amenorrhoea after the age of 50 years. A clinical history of amenorrhoea is sufficient to establish menopause and investigations of hormonal levels such as follicle stimulating hormone (FSH) are not required for women in this age range.4
Women using hormonal contraception
For women using hormonal contraception, amenorrhoea cannot be used to determine menopause because progestogen-only methods can themselves induce amenorrhoea. Further, women using combined methods will continue to have withdrawal bleeding in the hormone-free break, regardless of their menopausal status.
Women using the levonorgestrel IUD, the contraceptive implant or the progestogen-only pill can choose to continue the method until they are 55 years of age, provided there are no contraindications. Women can be advised that conception after this age is extremely unlikely.
Sexually active women who prefer to stop their progestogen-only method before the age of 55 years, can have a single FSH measurement taken after a year of amenorrhoea since turning 50 in order to predict the likelihood of menopause and guide clinical advice on when to cease contraception. The Faculty of Sexual and Reproductive Healthcare (FSRH) Guideline recommends a single FSH level of more than 30 IU/L as sufficient to discontinue contraception use after a further year. If the FSH level is 30 IU/L or less, the test can be repeated after 12 months.4
Although the contraceptive injection is not generally recommended for women aged over 50 years, a single FSH measurement can be used, as above, to determine when injections can be stopped, as progestogen-only methods do not affect the increase in FSH associated with menopause. FSH measurement cannot be used to predict menopause for women using combined hormonal contraceptive methods because oestrogen can suppress FSH.5
Considerations if contraception is required
If contraception is required, GPs should seek specific information from the patient. The woman’s preference, her social circumstances and her past experience with contraception are a good starting point; however, choices become more limited once a woman turns 50.
Contraceptive methods not recommended once a woman turns 50 years
Combined hormonal methods
Once a woman reaches the age of 50 years, there is an increased background risk of arterial vascular and venous disease, thus the use of oestrogen-containing hormonal methods, i.e. the combined oral contraceptive and the vaginal ring, are not recommended by the FSRH. Women should be advised to switch to another method of contraception until menopause is established and warned that oestrogen- containing contraceptive methods can mask menopausal symptoms, and that symptoms such as hot flushes might occur on cessation of the combined method. It is important to note that menopausal hormone therapy (MHT) is not considered contraceptive.
Depot medroxyprogesterone acetate (DMPA) injection
The use of DMPA is associated with a reduction in circulating oestrogen.6 This reduction in oestrogen is associated with a loss of bone density and there is a theoretical but unproven concern that this could result in an exacerbated fracture risk for women approaching menopause.7 DMPA may also have adverse effects on lipids, by altering lipid metabolism and affecting HDL and LDL cholesterol levels.8-10 DMPA users are generally advised to switch to another method of contraception at the age of 50 years; however, the benefits of initiating or continuing with DMPA might outweigh the risks for some women, such as those without additional cardiovascular disease risk factors who would benefit from DMPA-associated amenorrhoea. In addition, DMPA can be useful in reducing hot flushes.11 Ongoing use beyond 50 should be assessed on a case-by-case basis.
Contraceptive methods
The long-acting reversible contraceptive (LARC) methods (levonorgestrel IUD, copper IUD and contraceptive implant) are first-line recommendations for women of all age groups, including those 50 years and over. They are extremely effective and have high continuation rates. The progestogen- only pill can also be recommended to women aged 50 years and over as it is low dose, noninvasive and likely to be highly effective in this age group who have lower background fertility than younger women. Other methods with relatively low efficacy may also be suitable for women in this age group including condoms and the diaphragm.
IUDs
The levonorgestrel IUD
Levonorgestrel IUDs are a popular choice (the 52 mg levonorgestrel IUD is PBS-listed), with the benefit of a large reduction in menstrual bleeding and a reduction in dysmenorrhea.12-14 This can be particularly beneficial for women experiencing heavy menstrual bleeding in the perimenopause, with amenorrhoea being achieved in about 40% of users during the fifth year of use.15 It can also be used for endometrial protection in women who use MHT, or may wish to in the future for the control of vasomotor symptoms.16 When used in this situation, the device must be changed every five years with no recommendation for extended use.4
A 52 mg levonorgestrel IUD inserted at the age of 45 years or older can be left in place until menopause is determined (off-label extended use) using a single FSH measurement as previously discussed or until the age of 55 years.4 This advice does not apply to newer lower dose levonorgestrel IUDs that may become available in Australia in the future, including the 19.5 mg levonorgestrel IUD, or devices inserted overseas.
The copper IUD
The copper IUD is not PBS-listed and costs around A$70 to A$100. It can be an attractive option for those who prefer hormone-free contraception or who have contraindications to hormones. The main disadvantage of the copper IUD is an increase in menstrual blood loss, which limits its use in women experiencing heavy menstrual bleeding at the perimenopause.17 It provides extremely effective emergency contraception when it is inserted within five days of unprotected intercourse.18 Any copper IUD approved for use in Australia and inserted from the age of 40 years can be left in place until menopause, regardless of whether a five- or 10-year IUD is used and the age at which menopause occurs (off-label extended use).
Insertion of a copper or levonorgestrel IUD is associated with a small risk of uterine perforation, procedure-related infection and expulsion. When rare cases of failure occur, there is a moderately high risk the pregnancy will be ectopic rather than intrauterine, although the overall rate of ectopic pregnancies is reduced in women using IUDs compared with the rate in women not using contraception.19
The contraceptive implant
The contraceptive implant is extremely effective and has few contraindications. It does not adversely affect bone density and there are no clinically significant metabolic effects.20,21 The only known serious complication is deep insertion with migration of the device. Although around 20% of users achieve amenorrhoea, troublesome bleeding can also occur in 20% of all users.22 New onset bleeding abnormalities in women aged 50 years and older who have the contraceptive implant, should prompt consideration of investigations to rule out underlying pathologies such as endometrial hyperplasia and carcinoma that may be causing the bleeding rather than the implant. Note that the contraceptive implant cannot be used for endometrial protection in women using oestrogen as part of an MHT regimen.
The progestogen-only pill
The progestogen-only pill is a low-dose, oestrogen-free oral option. The timing of daily pill-taking is strict and a pill that is more than three hours late is considered missed. There are no known serious risks. However, as with other progestogen-only methods, irregular bleeding can occur and may prompt investigation in this age group because of the higher risk of serious pathology. As with the implant, the progestogen-only pill cannot be used to protect the endometrium as part of an MHT regimen.
Barrier methods
Although barrier methods have lower perfect and typical use efficacy compared with hormonal methods and the copper IUD, condoms and the single-size diaphragm can be relatively effective in this age group because of low background fertility.23 Unlike the diaphragm, both male (external) and female (internal) condoms have the additional benefit of protection from sexually transmissible infections (STIs). Male condoms can be problematic if the partner has erectile dysfunction, but female (internal) condoms and the diaphragm are unaffected.
The use of additional lubricants (must be water- or silicone-based for male latex or polyisoprene condoms) or regular use of vaginal oestrogen cream can assist with vaginal dryness, which may be a common issue for women in this age group.
Condoms are the only method that also prevent STIs and can be combined with other effective methods of contraception if required.
Withdrawal
Withdrawal is not recommended as a method of contraception at any age; however, it is acknowledged that it can be reasonably effective for very experienced users in this age group because of lowered background fertility.
Fertility awareness methods
Fertility awareness methods may be less effective in older women compared with other age groups because of the increased incidence of irregular cycles in the perimenopause, and are generally not recommended.
Oral emergency contraception
Women aged 50 years and over can be advised about oral emergency contraception, either the 1.5 mg levonorgestrel pill or the 30 mg ulipristal acetate pill, available over the counter at pharmacies. There are no contraindications to the oral emergency contraception in any age group.24
Permanent methods
Although tubal sterilisation or vasectomy in a partner can be considered, the relative benefits might be outweighed by the risks at this stage of reproductive life considering the low chance of conception.
Contraindications to contraceptive methods in women aged 50 years and over
Contraindications to the progestogen-only pill, the contraceptive implant, and both the levonorgestrel IUD and copper IUD can be considered in the same way as for younger women.
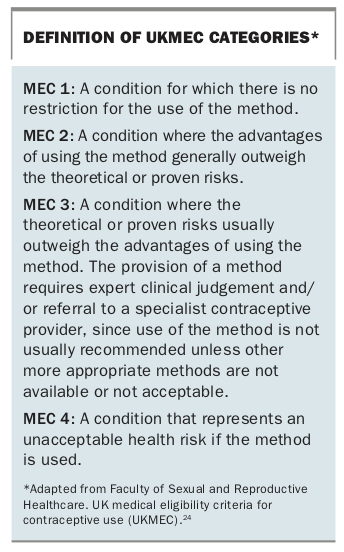
The UK Medical Eligibility Criteria (MEC) uses a four-tier system to classify conditions and risk factors affecting eligibility for hormonal contraception and copper IUDs. MEC 1 indicates that no restrictions exist, whereas MEC 4 is an absolute contraindication (Box).24 According to the FSRH Guideline, the most important MEC 3 or 4 contraindications to the levonorgestrel IUD, the contraceptive implant and the progestogen-only pill include current or past breast cancer, severe liver disease and hepatocellular adenoma or carcinoma. A history of venous or arterial vascular disease is MEC 2; however, if a user develops ischaemic heart disease, stroke or has a transient ischaemic attack while using these methods, then continued use is MEC 3 and switching to an alternative method is generally recommended. The levonorgestrel IUD also shares some MEC 3 or 4 contraindications with the copper IUD. These include unexplained vaginal bleeding suspicious for a serious condition, current pelvic infection, initiation in those diagnosed with endometrial or cervical cancer and distortion of the uterine cavity. Women with long QT syndrome, should have the IUD inserted in a hospital setting to avoid the risk of a bradycardia-induced arrythmia.24 For DMPA use, multiple risk factors for cardiovascular disease or a past history of stroke or ischaemic heart disease is MEC 3.
{kind=link}
Medication interactions
A number of specific medications, referred to as liver enzyme inducers, decrease the efficacy of most methods of hormonal contraception including the progestogen-only pill and the contraceptive implant, which may be recommended from the age of 50. These medications include but are not limited to some antiepileptic and antiretroviral drugs, and rifampicin/rifamycin.25 Contraceptive methods that are not affected by liver enzyme inducers include the hormonal IUD, non-hormonal contraceptives, the copper IUD and barrier methods. DMPA is also unaffected but is generally not recommended in this age group.
Supporting shared decision-making
Once a medically suitable method (or methods) of contraception has been established, GPs should help support women in their choice of method by discussing the following considerations:
- risk of sexually transmissible infections
- frequency of intercourse
- difficulty with daily pill-taking
- heavy menstrual bleeding
- partner erectile function
- desire for privacy
- costs and access to contraceptive
- previous side effects.
Conclusion
Contraception remains important for women aged 50 years and over who have continuing fertility. Although there are some limitations in contraceptive choice, a number of options can be considered. As for all reproductive age groups, the long-acting reversible methods are first-line choices; however, lower background fertility may make less effective contraceptive methods acceptable. A thorough medical and social history is important and can assist the GP to support women in making a suitable choice for their individual circumstances. MT