Screening for atrial fibrillation: the essential role of GPs

Asymptomatic atrial fibrillation (AF) is associated with similar stroke risk as symptomatic AF, yet is often detected only after the patient presents with a devastating stroke. The first Australian guidelines for the screening and management of AF were released in 2018 by the National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand. This brief, practical summary of the guidelines focuses on screening in general practice.
- Atrial fibrillation (AF) is the most common heart arrhythmia, and is associated with a fivefold increased risk of stroke.
- AF increases markedly in prevalence after 65 years of age and often occurs in patients with multiple comorbidities.
- Opportunistic single-time point AF screening detects asymptomatic (‘silent’) and largely persistent AF, which confers similar stroke risk as the symptomatic form.
- Australian guidelines recommend opportunistic screening for AF in all people aged 65 years and older.
- Opportunistic screening can be incorporated easily and with minimal cost in routine patient care in general practice. New systems and technologies are being developed to overcome time barriers to screening in general practice.
- Significant reductions in preventable stroke can be achieved if AF screening works hand in hand with the provision of treatment and efforts to facilitate patient adherence.
Atrial fibrillation (AF) is a cardiac arrhythmia causing an uncoordinated contraction of the heart; the atria do not contract at all, and the ventricular rate is irregular. It is the most common arrhythmia seen by GPs in Australia, and its incidence is increasing with the ageing population, rising prevalence of risk factors such as hypertension and overweight/obesity, and increased longevity of patients with cardiac morbidities.1 About 3% of the population, or half a million adults in Australia, are estimated to have AF, with this proportion expected to double over the next two decades.2 The prevalence of AF increases markedly among older adults and is around 10% in the 75 years and older age group.3
AF is associated with increased mortality, cognitive decline, dementia, heart failure and renal dysfunction. However, the most devastating consequence is thromboembolic stroke, and about one-third of ischaemic strokes are attributed to AF.2,4 These strokes are more likely to be fatal or debilitating and to have a significant adverse impact on quality of life. Randomised controlled studies have shown that stroke in patients with AF can be reduced by two-thirds with oral anticoagulant therapy.5 However, because AF in older people is often asymptomatic (‘silent’), screening is required to reduce the approximately 10% of ischaemic strokes related to AF that are first diagnosed at the time of the stroke.
GPs are in a unique position to detect asymptomatic AF, and new Australian guidelines recommend that all patients aged 65 years and over should be opportunistically screened for AF by either pulse palpation or with a handheld ECG rhythm strip.2 If AF is detected then initiation of oral anticoagulant treatment by GPs can play a central role in reducing stroke risk.
This article provides a brief, practical summary of recent Australian guidelines on screening for AF, focusing on screening in general practice.
New national guidelines align with the Australian primary care environment
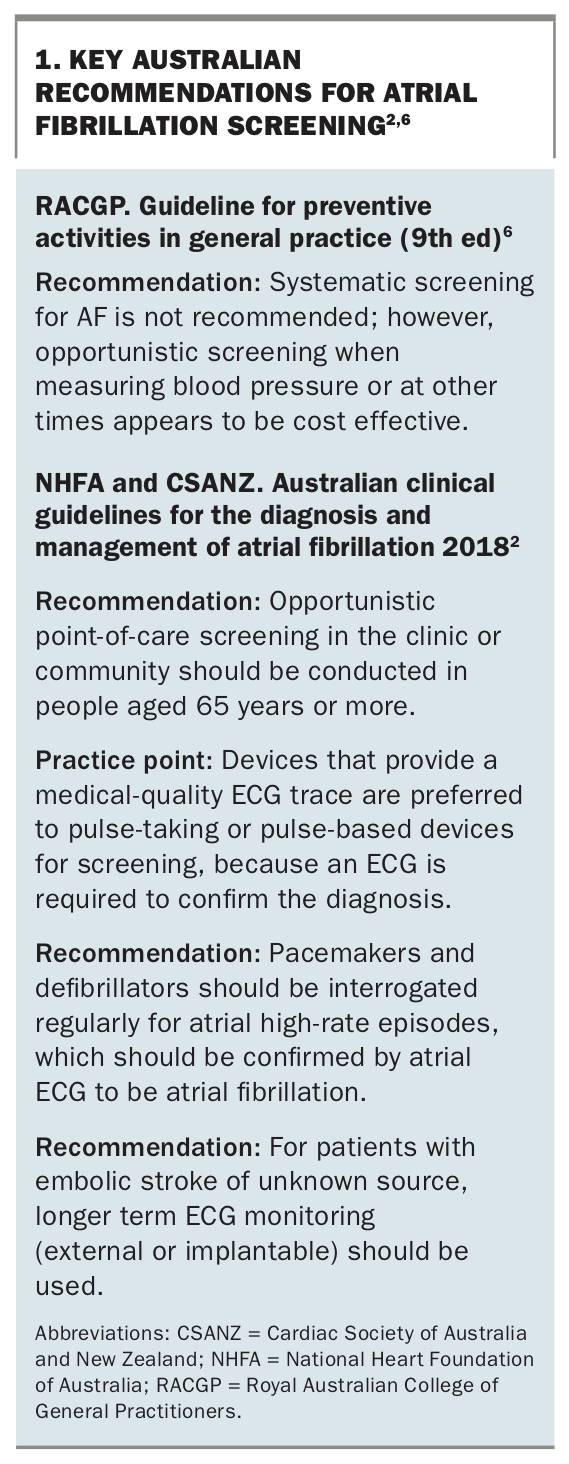
Over the past decade, much has changed in the landscape of AF screening and treatment. In 2015, the Cardiac Society of Australia and New Zealand (CSANZ) and National Heart Foundation of Australia (NHFA) undertook a review of emerging cardiovascular issues in Australia, and identified AF as an increasingly burdensome condition with evolving therapeutic management options and large treatment gaps.2 In the 2016 revision of the Guidelines for Preventive Activities in General Practice (Red Book), the RACGP included a new recommendation that all patients aged 65 years and older be screened opportunistically for AF.6 Two years later, the first Australian-developed guidelines, Australian Clinical Guidelines for the Diagnosis and Management of Atrial Fibrillation 2018, were released by CSANZ and NHFA.2 Key recommendations of these Australian-specific screening guidelines are summarised in Box 1.2,6
{kind=link}
Before these guidelines were developed, AF screening efforts in Australia were ad hoc, guided by a range of international guidelines with nuanced differences in recommendations, and not aligned to the Australian primary care environment. There are marked differences in primary care between Australia and other countries that have guided AF screening, such as Europe, where AF guidelines recommend opportunistic screening, and the US, where guidelines make no recommendation. A distinctive feature of general practice in Australia is its model for equitable provision of healthcare that is low- or no-cost to patients.7 Australian GPs tend to be more engaged in chronic disease management and are the first port of call for referral to specialist services. The vast geography of Australia also dictates that the scope of primary care provision in rural areas is often more diverse than in other countries.
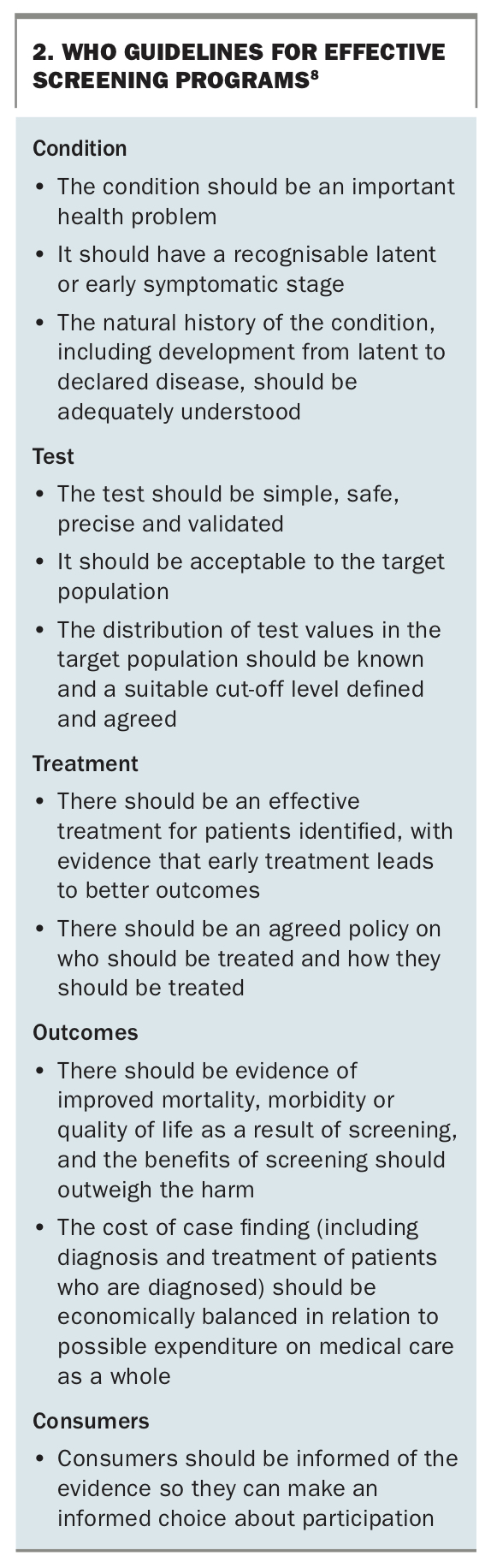
To be effective, screening efforts need not only to engage the target population in the screening but also to tackle a significant health issue with an effective available treatment, to use a screening method that is low cost and readily available, and also to include a pathway to access treatments that have demonstrated benefits in terms of morbidity and mortality (Box 2).8 AF screening meets most of these criteria, and Australian GPs are optimally placed because of their coverage of the 65 years and over age group, their preventive health role, and ability to provide a clear and direct pathway from the screening of AF to its management.9
{kind=link}
Screening identifies patients with asymptomatic AF
About two-thirds of patients with AF have symptoms.2 These patients often present to their GP or a hospital emergency department with palpitations or nonspecific symptoms such as fatigue, dizziness, dyspnoea or reduced exercise tolerance. Most will then be investigated with an ECG, which will detect AF, and they will be treated accordingly. One-third of patients with AF are asymptomatic. The arrhythmia in these patients would be detected only when discovered incidentally by an ECG performed for another reason or when the patient presents with a complication of AF.
In around 10% of patients with stroke attributed to AF, the AF was asymptomatic, and stroke was the first clinical presentation.10,11 If the arrhythmia had been detected earlier and appropriate treatment commenced, these patients might have been spared the risk of a potentially fatal or debilitating outcome. Stroke is an unacceptable warning sign for AF. It is crucial to note that asymptomatic AF carries the same stroke risk as symptomatic AF.12 Screening has the potential to identify individuals with asymptomatic AF who are nevertheless at high risk of stroke, so that stroke prevention treatments can begin in a timely manner.
Screening for AF is associated with minimal harms and is acceptable to patients
The benefits of stroke avoidance outweigh the minimal risks and theoretical harms of AF screening.13,14 Screening by pulse palpation or a single-channel ECG recorded with a handheld electronic device is not invasive, carries minimal risk to the patient and can increase rapport between practitioners and their patients.15 Patients positively evaluate the use of novel handheld ECG devices for assessing heart rhythm.15 Either method of screening is low cost, fast and easily incorporated into patient consultations.
Both pulse palpation and ECG recording with a handheld electronic device have good reliability and validity; however, an irregular pulse always requires confirmation of AF with either a 12-lead ECG or an ECG rhythm strip.4 Although the diagnosis of AF requires only a 30-second ECG rhythm strip, a 12-lead ECG is required for the additional diagnostic information it provides. The ECG rhythm strip and 12-lead ECG both need review by a GP or physician experienced in ECG interpretation to confirm the automated diagnosis and reduce the rate of false positives (which is less than 0.01% with some automated algorithms for the detection of AF4), which can lead to unnecessary investigations, anxiety and the risks of unnecessary oral anticoagulant therapy.
An important tip is that the handheld single-channel ECG is actually lead 1 (right arm to left arm) of a multiple-lead ECG, and the trace is therefore equivalent to the lead 1 trace on a 12-lead ECG. The finding of P waves in lead 1 of a 12-lead ECG performed after a handheld ECG rhythm strip showed no P waves and an irregular rhythm suggests paroxysmal AF, which is occasionally found through opportunistic single-time point screening.
Opportunistic point-of-care screening in the clinic or community is recommended in people aged 65 years or more
Many of the formalised screening activities in primary care are systematic screening programs that occur at defined ages or time intervals. In contrast, opportunistic screening takes place not on a regular schedule but whenever a patient attends primary care.6 When screening is incorporated into routine patient care in general practice, there is a direct pathway for GPs to review and manage abnormal results. Further, when screening is undertaken opportunistically, the repeated screenings that occur at each patient visit increase the likelihood of detecting paroxysmal or new-onset AF.
Opportunistic screening is more likely to detect persistent or permanent AF, which is associated with higher stroke risk, and occasionally detects paroxysmal AF with a high AF burden. These high-burden forms generally develop in ageing hearts and are also associated with comorbidities such as hypertension, myocardial ischaemia, diabetes, cardiac failure and cardiomyopathy.2 Therefore, it is not surprising that the prevalence of known AF increases with age, with an upswing seen around 65 years of age and a steady increase thereafter.16 The prevalence of asymptomatic AF is more difficult to ascertain, but recent Australian studies have estimated a prevalence of 1.4% in the 65 years and over age group, using screening with a single-time point 30-second handheld ECG in the community and general practice settings.17,18 When screening is repeated opportunistically as part of an ongoing program, the cumulative detection rate is likely to be higher.
General practice is the ideal location for screening as more than 90% of patients aged 65 years and over see their GP at least annually, with 70% visiting at least twice a year.9 Opportunistic screening for AF was shown to be cost effective in an Australian study utilising a single-time point 30-second handheld ECG in pharmacies, and opportunistic screening was shown to be more economical than systematic screening for increasing quality-adjusted life years and reducing stroke.17 A limitation of screening in pharmacies is that it lacks a clear or direct referral pathway for the management of patients with results suggesting AF or other abnormalities.4 The cost effectiveness of screening at GP practices has not been evaluated in Australia; however, an economic evaluation is currently underway. Further economic efficiencies would be expected when opportunistic screening is adopted as an enduring program rather than a one-off screen.
The NHFA/CSANZ guidelines also address AF screening among patients with implantable electronic devices and those presenting with embolic strokes of unknown cause.2 These patients are likely to be a small minority presenting in general practice, and device-detected AF will usually be reported to a cardiologist or neurologist rather than to the GP.
There are simple ways to screen for AF in general practice and new technologies and systems are being developed
Pulse palpation is the simplest and most cost effective means of screening for AF and is a free tool available to all GPs. Research shows that when GPs perform pulse palpation, their sensitivity for detecting AF is excellent and similar to that of electronic medical-grade devices.19 Despite the ease of undertaking pulse palpation, an international study found only 11% of Australian GPs performed it regularly.20 The most commonly reported barrier to pulse palpation is a lack of time during consultations, with GPs reporting an already jam-packed consultation agenda, driven by increasingly complex patients with multiple comorbidities.21 The high uptake of electronic blood pressure monitors that do not report on pulse regularity in general practices may also have steered practitioners away from pulse palpation.20
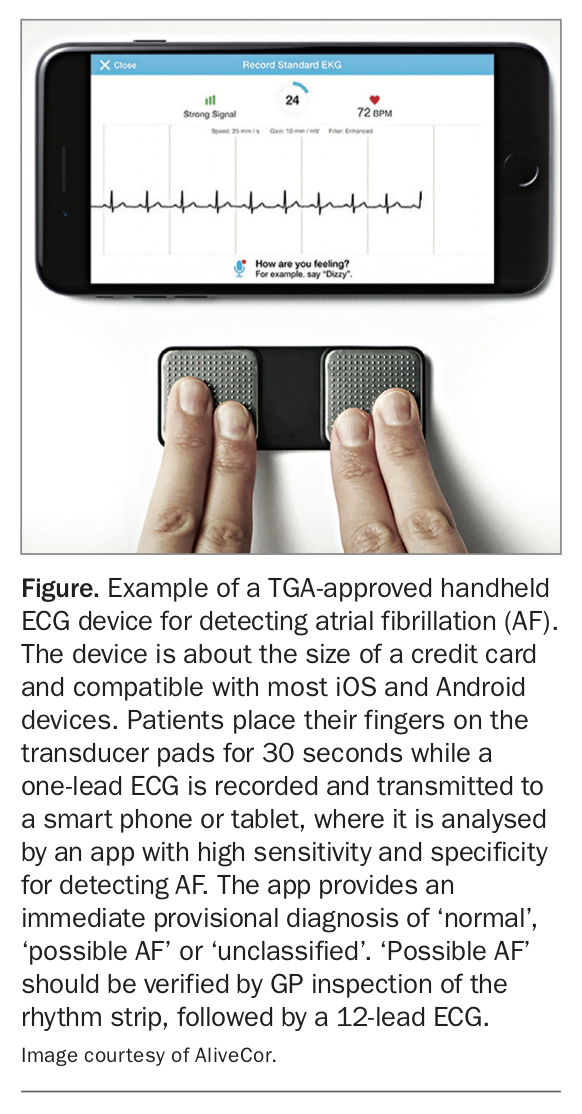
Both the RACGP and NHFA/CSANZ guidelines recommend manual pulse palpation for AF screening; however, the latter guidelines suggest that devices producing a medical-quality ECG trace are preferable, as an ECG is required to confirm the diagnosis.2,9 Several handheld single-channel ECG devices with automated rhythm-analysis algorithms for the detection of AF have been approved by the TGA and are suitable for opportunistic single-time point screening. They include the KardiaMobile (AliveCor) and WIWE (WIWE Australia).22,23 Both devices are about the size of a credit card. Patients place their fingers onto sensors on the device while a one-lead ECG is recorded and transmitted to a smart phone or tablet, where it is analysed by an app with high sensitivity and specificity for detecting AF (Figure).
{kind=link}
Trials of implementing an automated prompt for GPs to screen for AF incorporated in general practice software coupled with a handheld ECG device have shown AF screening to increase to 16%.18 Further gains in screening prevalence to around 39% have been achieved when screening is implemented during influenza vaccination clinics, which have high uptake with the target age group.24 Although this is a substantial gain in screening, it still falls far short of the screening prevalence required to substantially reduce AF-related strokes in Australia. Time constraints in the consultation time are still reported as the main barrier to achieving a greater uptake of screening and must be overcome to increase the effectiveness of screening.21
Australia is at the forefront of developing novel approaches to AF screening in general practice
An AF screening think tank comprising GPs, cardiologists, GP practice managers, GP practice nurses and patients was convened by the Heart Research Institute in Sydney in 2018 to discuss novel approaches to increase GP-led AF screening. The consensus was that higher screening rates could be achieved if screening was a minimal burden for practitioners and reception staff and if the results could be integrated into the existing workflow of GPs. A patient self-screening kiosk that transfers screening results to the patient medical record and integrates into GP workflow was raised as an option. We are currently undertaking a proof-of-concept study to assess the viability of such an AF self- screening station in GP practices to circumvent time pressure in consultations and better utilise the time patients spend waiting before a GP appointment for opportunistic screening.
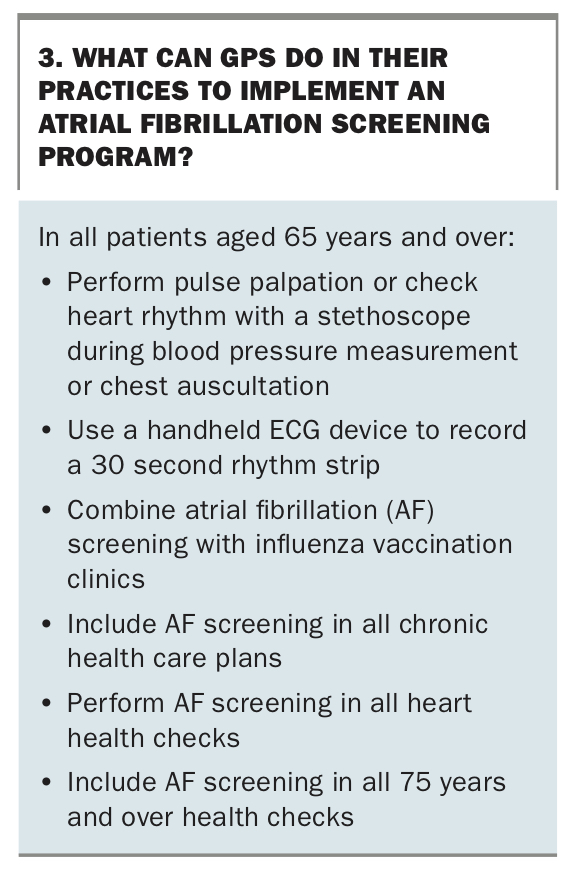
Other suggested strategies to help GPs begin implement opportunistic screening in their day-to-day practice are summarised in Box 3. Adopting a routine moment or opportunity for screening regularly incorporated into patient care will detect more disease than ad hoc screening. New screening technologies will be effective only if they are routinely incorporated in practice.
{kind=link}
Screening is only one step in reducing avoidable strokes
Identifying patients with asymptomatic AF is an important first step in reducing avoidable stroke, but medical management of high-risk patients needs to be optimised in tandem with improved screening to maximise reductions in avoidable AF-related strokes. The 2018 NHFA/CSANZ guidelines provide guidance on evidence-based management of newly diagnosed and existing AF, as summarised in the November 2019 issue of Medicine Today.25 Important changes are the omission of antiplatelet agents as medications to reduce stroke risk when AF is diagnosed, and the recognition that the benefits of stroke and mortality reduction from oral anticoagulant therapy outweigh the risk of major haemorrhage in patients at increased stroke risk (CHA2DS2-VA score of 2 or more).
Reassuring data suggest that the management of AF has improved in Australia over the past decade, with prescription rates of oral anticoagulants among high-risk patients steadily increasing.26 Although this is promising, there is scope for further improvement, as between one-third and one-quarter of patients with AF and high risk of stroke are not taking oral anticoagulant therapy.17 In countries where oral anticoagulant prescription rates have increased substantially, the AF-related stroke rate has decreased substantially.27,28 In the UK, oral anticoagulant prescription rates increased from 48.0% to 78.6% between 2006 and 2016, and this was estimated to have prevented 4068 strokes in 2015-2016 alone.10,27
Optimising patient adherence and persistence in taking oral anticoagulants is another challenge for GPs to reduce the incidence of avoidable strokes, as adherence to oral anticoagulants drops to less than 50% by 12 months after their initial prescription.2,26 Consequently, improved screening rates need to be combined with better management of high-risk patients and focused strategies to improve adherence and persistence with oral anticoagulant therapy to reduce avoidable strokes.
Conclusion
GPs are optimally positioned to reduce AF-related strokes, and screening for silent AF is a simple and cost effective way to identify patients who are at high risk of stroke. New Australian guidelines recommend opportunistic screening among patients aged 65 years and older, and there are multiple ways GPs can incorporate this into their day-to-day practice, as well as new technologies that may circumvent the time barriers faced by practitioners. A multipronged approach that improves screening rates, oral anticoagulant prescription and adherence among high-risk patients will result in the greatest reductions in AF-related strokes. MT
COVID-19 and GP screening for atrial fibrillation
Advice from the authors of this article on GP screening for AF during the COVID-19 pandemic is provided in the Box.
{kind=link}