
Dr Harris is a Dermatology Research Fellow, and Associate Professor Fischer is Associate Professor of Dermatology at Sydney Medical School – Northern, University of Sydney, Royal North Shore Hospital, Sydney, NSW.
Competing interests: None.
What’s the diagnosis?
A boy with papules on the toes and rash on the face






Case presentation
A 13-year-old boy presents with verrucous periungual lesions on his toes, which have been treated with cryotherapy on three occasions without success (Figure 1a). He also has some small red lesions scattered over his face that his mother mentions have been unresponsive to acne treatment (Figure 1b). The boy is otherwise well, but he has had learning difficulties at school.
On examination, the periungual lesions are observed to be papules with a smooth surface. No comedones or pustules are visible on the boy’s face, but he has multiple round, red micropapules, around 1 mm in diameter, along his nose, cheeks and nasolabial folds. A number of white macules are also noted on the trunk, arms and legs.
Differential diagnoses
Conditions to consider among the differential diagnoses for a child of this age include the following.
- Periungual warts. Common warts present as firm papules with a rough horny surface (Figure 2). They can disturb nail growth and may clear spontaneously at any time. It is unlikely to be the correct diagnosis of the periungual lesions in this patient’s case because his papules have a smooth surface.
- Digital fibroma. These smooth papular lesions are usually congenital. Digital fibromas typically resolve within a few years, but recurrence into adulthood has been reported.1
- Lymphangioma. These small lymphatic malformations may occur anywhere on the skin. They may be skin-coloured but a violaceous appearance is not uncommon (Figure 3). A lymphangioma can develop a rough surface and be mistaken for a wart when occurring on the foot (Figure 4).
- Tuberous sclerosis. This is the correct diagnosis. The case patient’s periungual lesions are fibromas known as Koenen tumours and the lesions on his face (which were mistaken for acne) are angiofibromas. The white macules on his trunk and limbs are areas of hypopigmentation; these are known as ‘ash leaf’ macules but they can take any shape.
Clinical features
Tuberous sclerosis is a dominantly inherited genetic disorder of hamartoma formation that affects multiple organs, particularly the skin, eye, kidney and heart. Onset before the age of 5 years is usual, but the disease can remain latent until adolescence or adulthood.
The three typical features of tuberous sclerosis are skin lesions, intellectual impairment and epilepsy, although these features are not all present in every patient. Characteristic skin signs include the following.
– Angiofibromas. These red-brown lesions usually appear around the age of 3 to 10 years and often become more extensive at puberty. They are located on the face and present as firm, discrete, telangiectatic papules, 1 to 10 mm in diameter.
– Ungual fibromas. These lesions appear around puberty as smooth, firm, flesh-coloured lesions that emerge from the nail folds.
– Shagreen patch. This connective tissue naevus presents as a soft skin-coloured plaque that is slightly elevated and irregularly thickened. It is usually located in the lumbosacral region.
– Hypopigmented (ash leaf) macules, which present as white lesions on the skin of most of the limbs and trunk (Figure 5). They measure from 1 to 3 cm and are most easily detected under a Wood’s lamp examination. Hypopigmented macules are not uncommon in children; however, a diagnosis of tuberous sclerosis should be considered in a child who has more than three of these macules, particularly in the presence of other skin signs and family history of the condition.
Diagnosis
The genetic and clinical criteria for a diagnosis of tuberous sclerosis are described in the 2012 Tuberous Sclerosis Complex Diagnostic Criteria Update; the clinical criteria (major and minor features) are summarised in the Box.2 A definite clinical diagnosis of tuberous sclerosis requires either two major features or one major feature with at least two minor features. A possible diagnosis requires either one major feature or at least two minor features.
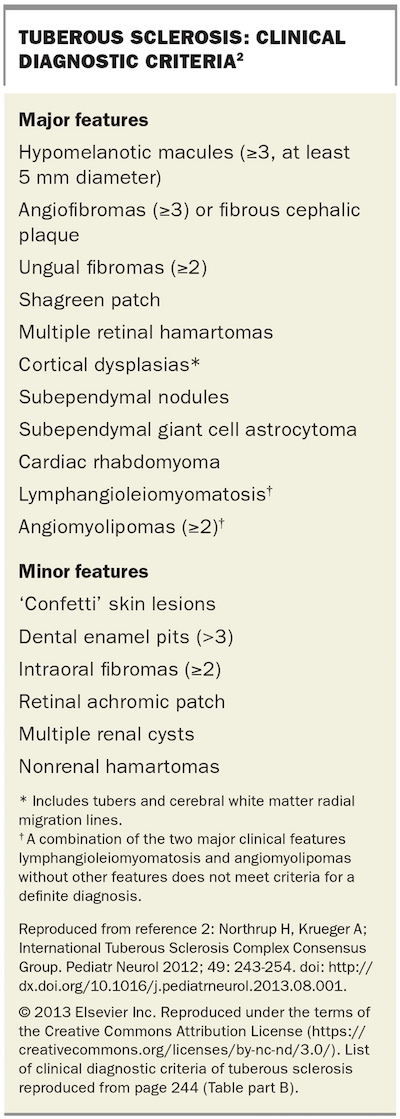{kind=link}
Management
A child with suspected tuberous sclerosis should be referred to a geneticist for evaluation. Patients with tuberous sclerosis may have renal, cardiac and ocular problems, which require assessment and multidisciplinary management. Early involvement of a neurologist is necessary for the management of epilepsy. Early intervention is essential for learning difficulties.
A periungual fibroma that is not causing discomfort can be left alone, but if removal is required then excision is the method of choice. Gum hypertrophy may be treated successfully with laser methods. Cutaneous connective tissue naevi and hypomelanotic macules are usually not a major cosmetic issue and can also be left untreated.
Facial angiofibromas, however, can be a major cosmetic issue. Laser treatment is often disappointing. Compounded topical sirolimus 1% applied daily may be of great benefit in children (off-label use).3 Systemic sirolimus may be useful in the treatment of cutaneous and visceral tumours for all age groups (off-label use).4
The clinical spectrum of tuberous sclerosis is wide. The life expectancy for a severely affected individual can be poor but many patients remain well and live a normal life.
References
1. Marks E, Ewart M. Infantile digital fibroma: a rare fibromatosis. Arch Pathol Lab Med 2016; 140: 1153-1156.
2. Northrup H, Krueger A; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol 2012; 49: 243-254. Available online at: http://www.pedneur.com/article/S0887-8994(13)00490-6/abstract (accessed February 2017).
3. Tanaka M, Wataya-Kaneda M, Nakamura A, Matsumoto S, Katayama I. First left–right comparative study of topical rapamycin vs. vehicle for facial angiofibromas in patients with tuberous sclerosis complex. Br J Dermatol 2013; 169: 1314-1318.
4. Nathan N, Wang J, Shaowei L, et al. Improvement of tuberous sclerosis complex (TSC) skin tumors during long-term treatment with oral sirolimus. J Am Acad Dermatol 2015; 73: 802-808.