An approach to the patient with bloody diarrhoea

Gastrointestinal bleeding
Bloody diarrhoea is a common, usually benign presentation, but all patients require prompt review. Infective agents, such as Campylobacter species, are the most common causes, although other serious causes include malignancy and bowel ischaemia.
- In the Australian community, diarrhoea alone is a common and usually benign symptom, but the presence of blood is alarming for a patient and will usually prompt a medical review.
- The most common causes of bloody diarrhoea are infective agents, such as Campylobacter species.
- The most serious causes of bloody diarrhoea include malignancy, inflammatory bowel disease, bowel ischaemia and complications including sepsis related to severe infection and haemolytic uraemic syndrome.
- All cases of bloody diarrhoea warrant basic investigation including stool collection and analysis. Further investigation is then case specific.
- Patients should be referred early to hospital if they are very young, elderly or immunocompromised, or have peritonitis or significant systemic signs of sepsis, shock or dehydration.
- Review of all patients within 24 to 48 hours should be encouraged, and then again after seven to 10 days to ensure complete resolution of symptoms, and to inform and educate patients regarding culture results.
The occurrence of diarrhoeal symptoms among the population in Australia is common, with the majority of episodes being short and self-limited and presumed to be infective in origin. Diarrhoeal-related presentations to Australian GPs are frequent, accounting for about 1.3 per 100 GP encounters, or almost 1.25 million GP visits per year in Australia.1 The presence of blood in the stool is one factor that is likely to trigger a medical review, and the development of a diagnostic and management pathway for the patient with bloody diarrhoea is an important tool.
Bloody diarrhoea usually indicates colonic inflammation, often with smaller faecal volumes and passage of bloody, mucous-rich stools. This may be accompanied by tenesmus (the feeling of incomplete emptying with defaecation) and abdominal pain. Invasive enteric pathogens are most commonly involved. Small bowel involvement often results in a larger volume of watery diarrhoea, with cramping, bloating and weight loss. In general, the diarrhoea is usually less bloody.
Infants, young children, the elderly and those with complex medical issues and reduced physical reserve are more likely to have significant adverse outcomes associated with an episode of bloody diarrhoea. These groups also generally require earlier, more aggressive investigation and possibly earlier referral.
Approaching the patient
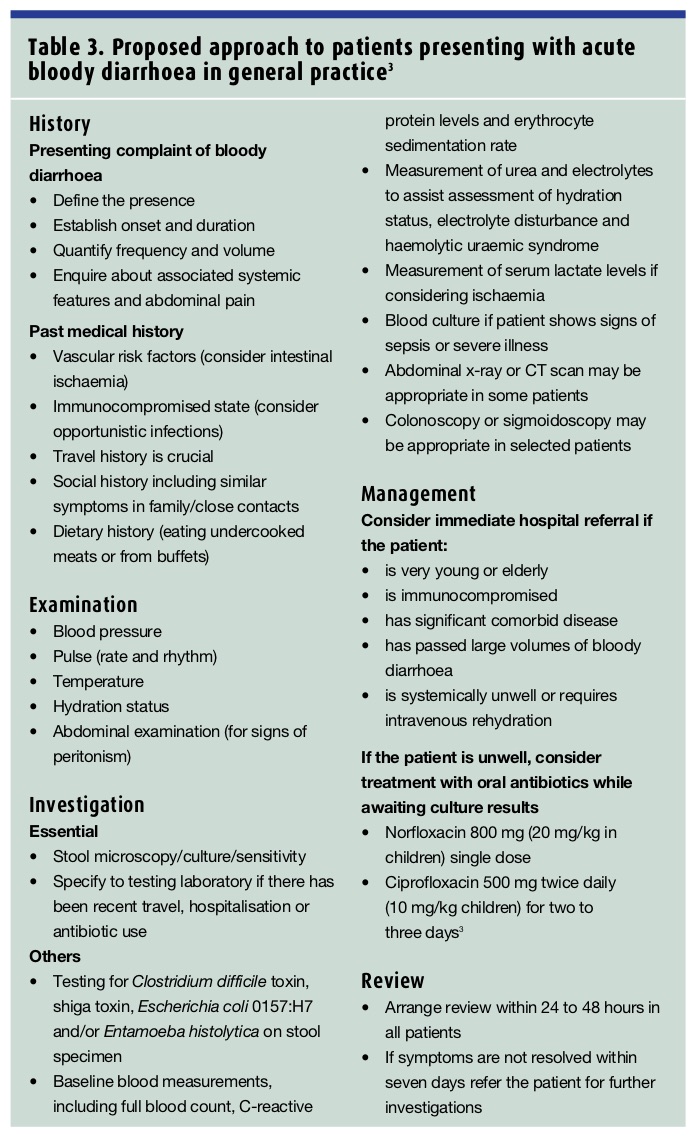
The causes of bloody diarrhoea are varied, some of which are listed in Table 1. Infective agents account for most cases of bloody diarrhoea in Australia, and some causative pathogens are listed in Table 2.2 A general approach to the patient with bloody diarrhoea is outlined in Table 3.3 Adult and paediatric patients share some common aetiologies; however, some unique causes need to be considered in paediatric patients, including infantile colitis, intussusception, malrotation and Hirschsprung’s disease.4
History
As in all aspects of medicine, a careful history is the best starting point. It is important to establish the onset and duration of the diarrhoea, the characteristics of the stool, the frequency and volume of the diarrhoea, and the presence or absence of associated features including vomiting, fever, abdominal pain and/or tenesmus. The basis of the definition of bloody diarrhoea is the macroscopic presence of blood that is mixed with the faeces or is inseparable from the stool.4 It is important to differentiate this from the presence of specks of bright red blood on the toilet paper after wiping or local soiling because this is more likely to be related to local perianal bleeding from excoriation, haemorrhoids or fissuring.
Enquiring about the patient’s recent travel history is vital. Any recent travel to areas of risk, including South-East Asia, Africa and South America, is important information to provide to the laboratory when requesting a stool analysis.
A thorough review of past medical history is relevant and may provide clues as to the aetiology of the condition, with vascular risk factors and immunodeficiency states being particularly important. For example, abdominal pain and bloody diarrhoea in a patient with a strong vascular history raises the possibility of gastrointestinal vascular insufficiency. Past or present radiotherapy to the abdomen or pelvis can predispose a patient to radiation-related colitis. A history of immunodeficiency increases the probability of an infective origin, particularly involving opportunistic pathogens. For example, in patients with advanced HIV infection or AIDS with CD4+ counts of less than 500 cells/mm3, opportunistic agents such as Cryptosporidium species, microsporidia, Cyclospora species, Mycobacterium avium intracellulare and cytomegalovirus should be considered, and may also prompt early specialist referral.4
Current and/or recent medication use should be reviewed in the patient with bloody diarrhoea, in particular the use of immunosuppressant medications, NSAIDs or antibiotics. Pseudomembranous colitis, associated with the emergence of toxin-producing Clostridium difficile strains, may occur during or up to four weeks after antibiotic use. Although usually not bloody, more severe disease may produce colonic bleeding.
A thorough social history including the occurrence of similar symptoms in close household contacts or contacts outside the family is very important. As infective agents remain the most common aetiology of bloody diarrhoea, a thorough dietary history is also vital, particularly relating to the ingestion of undercooked chicken, a common community source of campylobacter infection. A sexual history may also be appropriate, including relevant sexual behaviour such as men who have sex with men and those engaging in anal intercourse.
Relevant family history, including the occurrence of inflammatory bowel disease or colonic malignancy, should also be sought.
Examination
A general examination of the patient with bloody diarrhoea should include measurement of heart rate, blood pressure, hydration status and temperature. An irregular pulse in an elderly patient may suggest an ischaemic cause of bloody diarrhoea. A careful abdominal examination is very important, particularly focused on excluding signs of peritonitis, which may again indicate more serious illness and should lead to urgent hospital referral.
Investigations
The order of investigations will be guided by the clinical picture and patient demographics. Other factors influencing investigations include the GP location, either rural or urban, local access to laboratory facilities and specialist support. The level of experience and comfort of the individual GP will also influence which investigations will be performed in the community setting.
The presentation of a patient with acute bloody diarrhoea should always prompt stool collection for microscopy, culture and sensitivity. Of the infectious causes of bloody diarrhoea, many are notifiable diseases in Australia. The importance of testing and isolating these agents relates not only to the individual patient outcome, but also has broader public health implications, allowing for the tracking of outbreaks and identifying possible community sources of infection. Notifiable aetiologies in Australia include infection with shiga toxin-producing Escherichia coli, Shigella species, Salmonella species and Campylobacter species. Of infective agents, Australian figures released by the Department of Health and Ageing for 2009 revealed:5
- 15,925 infections with Campylobacter species
- 9542 infections with Salmonella species
- 622 infections with Shigella species
- 12 infections with E. coli-associated haemolytic uraemic syndrome.
When arranging for stool collection, it is important to remember that the diagnostic yield of stool culture can be as low as 1.2%.6 Three stool collections on three consecutive days increases the diagnostic yield significantly. However, current Medicare Benefits Schedule regulations only allow for one stool collection per patient per week, and testing more often than this may incur additional out-of-pocket expenses for the patient.
In addition to basic stool examination, additional testing for C. difficile toxin, shiga toxin and/or culture for E. coli 0157:H7 may be useful depending on the clinical situation. For example, if there is clinical or laboratory evidence of haemolytic uraemic syndrome, then targeted culture techniques for E. coli 0157:H7 would be appropriate. This is often not part of the routine stool analysis, and providing adequate clinical information will assist the laboratory in appropriate further testing. Bloody diarrhoea in a recently arrived immigrant or returned traveller from an area where Entamoeba histolytica is endemic, including tropical Africa, Asia and Latin America, would also prompt specific testing. The importance of guiding the testing laboratory with relevant clinical history should not be understated.
Obtaining baseline blood measurements may be useful; however, the need for these measurements will be guided by assessment of each case individually. A full blood count, including haemoglobin, differential and white cell counts, C-reactive protein levels and/or erythrocyte sedimentation rate may be useful. Measurement of urea, creatinine and electrolyte levels will help assess hydration status and detect electrolyte disturbances, and may suggest the presence of haemolytic uraemic syndrome. Serum lactate levels may become elevated late in the course of full-thickness intestinal ischaemia with bowel infarction; however, no serum marker has been shown to be sufficiently sensitive or specific for this diagnosis.7 Serum biomarkers are also seldom helpful for diagnosing the more common chronic intestinal ischaemia, in which more subtle mucosal changes are seen.7 Blood culture may also be appropriate, particularly when the clinical picture is that of severe illness with high fever or in the returned traveller when considering the possibility of salmonella infection.
Imaging of most patients with acute bloody diarrhoea who present in primary care is likely to have a limited role. However, there are some exceptions, particularly if the clinical picture is indicative of more severe illness. Plain abdominal x-ray may show colonic wall oedema consistent with colitis, the extent of the colitic process or changes of toxic dilation, a complication of both severe ulcerative colitis and some fulminant colonic infections.
A computed tomography (CT) scan may also be useful in demonstrating the extent of the colitis and detecting local complications including contained perforation and collections in some patients. It is also often used in the assessment of patients with suspected diverticulitis.8 Bloody diarrhoea alone is not a classic presentation for this condition, with diverticulitis more commonly associated with left iliac fossa pain and fever.9 A CT scan may also reveal a colonic mass lesion as a cause of bloody diarrhoea, which would prompt urgent referral for endoscopic assessment.
For most patients with acute bloody diarrhoea in the GP setting, flexible sigmoidoscopy or colonoscopy is not required as part of a routine investigation. Endoscopic examination can be very useful in some cases to allow for direct mucosal visualisation, determine the extent of inflammation and allow for tissue sampling for histopathology, as well as microscopy and culture of specific colonic pathogens.
From a primary health care perspective, referral for colonoscopy usually plays a role if:
- patients do not respond to empirical antibiotics
- patients have serial stool specimens containing blood and leucocytes and no bacterial growth
- patients have symptoms persisting for more than one week
- there is a high clinical suspicion of an alternative aetiology, including colonic malignancy.
Treatment
Determining which patients to treat empirically with antibiotics, and which to refer for early specialist investigation can be challenging. It is certainly reasonable to consider immediate hospital referral in patients:
- with significant constitutional symptoms
- who are very young or elderly
- who are immunocompromised
- with significant comorbid disease and limited reserve
- with large volumes of bloody diarrhoea
- with a high suspicion of an underlying malignancy.
Given that infective agents remain the most common cause of bloody diarrhoea in the community, with most occurring secondary to campylobacter infection, it may be reasonable to commence empirical antibiotics in the remainder of patients after the appropriate specimens have been collected.10 Table 3 lists appropriate antibiotic choices. It is, however, important to arrange adequate follow up, with all patients encouraged to return for review after 24 to 48 hours. A further review after seven to 10 days is also useful, to ensure complete resolution of symptoms, to arrange further investigation and/or referral for patients whose symptoms have not fully resolved.
{kind=link}
Conclusion
Bloody diarrhoea is a relatively common presentation in the primary care setting, and can represent serious pathology. Although the majority of patients will have an infective aetiology, the management should be tailored to each individual, and the formulation of a protocol for approaching these patients should help in identifying those with more serious causes. MT
COMPETING INTEREST: None.
References