Faecal occult blood tests. How and when to use (or not)

The most appropriate use of a faecal occult blood test is screening in people who are of average risk for colorectal cancer – namely, individuals aged between 50 and 74 years and without symptoms or risk factors that warrant colonoscopy surveillance. The faecal immunochemical test is now the technology of choice. To obtain the best results, faecal samples should be collected by the person who is being screened, following the instructions provided with the test kit.
Remember
- Faecal occult blood tests (FOBTs) are most accurate when stools are sampled correctly.
- Screening average-risk people for colorectal cancer (CRC) is the main and near-exclusive indication for use of FOBTs. The faecal immunochemical test (FIT) is the best technology.
- In people who are at increased risk for CRC, colonoscopy should be considered as the first-line option.
- An FOBT of any type should not be repeated to confirm an already-positive test result.
- An FOBT of any type should not be offered to people who are not able or not willing to undergo colonoscopy if indicated.
- The risk for colorectal neoplasia is low for at least the first four years after a high-quality colonoscopy in a person at average risk.
- The Australian National Bowel Cancer Screening Program (NBCSP) provides a suitable program using FIT for screening people at average risk.
What is an FOBT?
An FOBT is a test for occult (macroscopically not visible) blood in faeces.
How are samples collected for an FOBT?
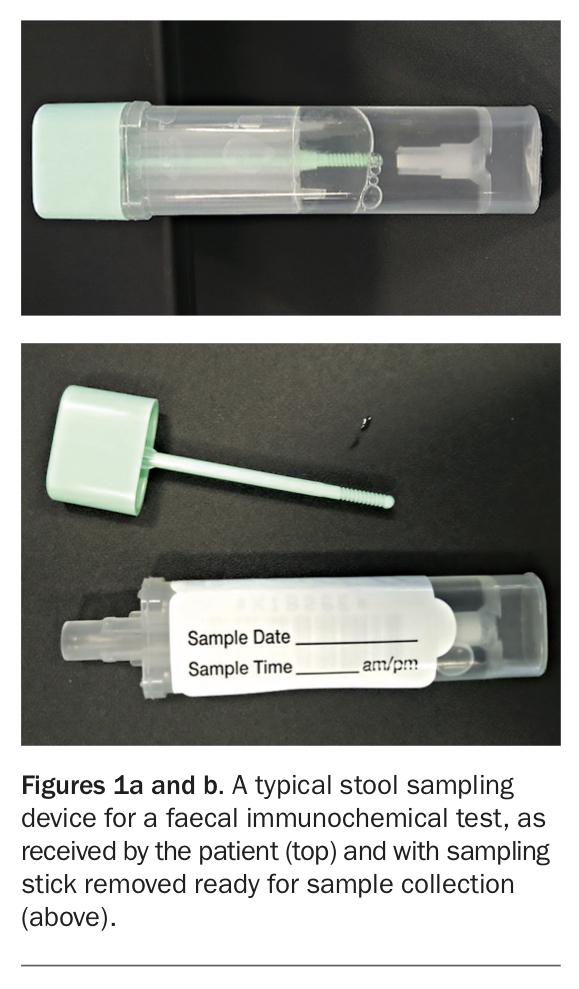
To obtain the best results from an FOBT, stool sampling devices must be used correctly and according to the provided instructions (Figures 1a and b). These devices control sample volume and minimise sample degradation in transit to the laboratory.
{kind=link}
The stool sample should be collected by the patient when passing a stool in the normal way. Many tests require the stool to be passed onto a paper ‘raft’ on top of the water in the toilet bowl to minimise immersion but a few tests do not require this.
It is advisable to collect samples from two separate stools because occult bleeding from gastrointestinal pathologies, especially colorectal neoplasia, varies in amount from stool to stool.
Appropriately sampled stool specimens need to be returned according to test instructions. Delays of more than a few days should be avoided; samples should be stored in a refrigerator (not freezer) in a hygienic device until returned. Some kits contain packets approved by Australia Post for returning tests by mail that are safe and hygienic, but to avoid excessive heat exposure these should not be posted on hot days.
The test result should be developed and read objectively (assuming a correctly sampled stool) in an approved laboratory.
What is analysed by an FOBT?
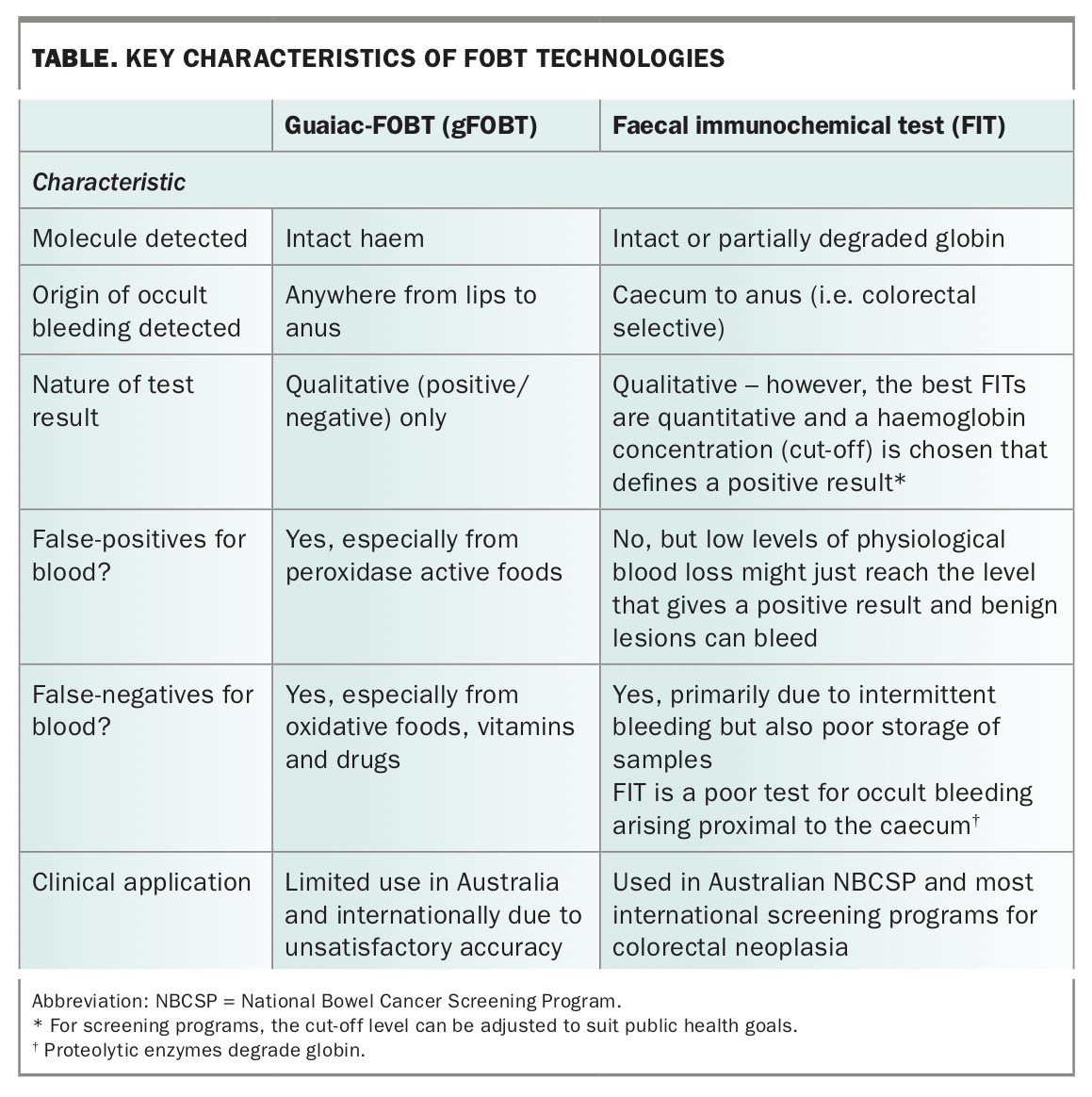
An FOBT detects certain components of blood in stool. There are two main technologies:
- guaiac-FOBT (gFOBT) – detects intact haem
- faecal immunochemical test (FIT, also known as iFOBT) – detects intact or partially degraded globin.
As the technologies detect different aspects of haemoglobin, they differ in their accuracy and the clinical context in which they are useful (Table).1
{kind=link}
The NBCSP uses a quantitative FIT. Results are reported qualitatively (positive or negative for blood), based on the cut-off for positivity considered to be suitable for the Australian context.
How and when is an FOBT used?
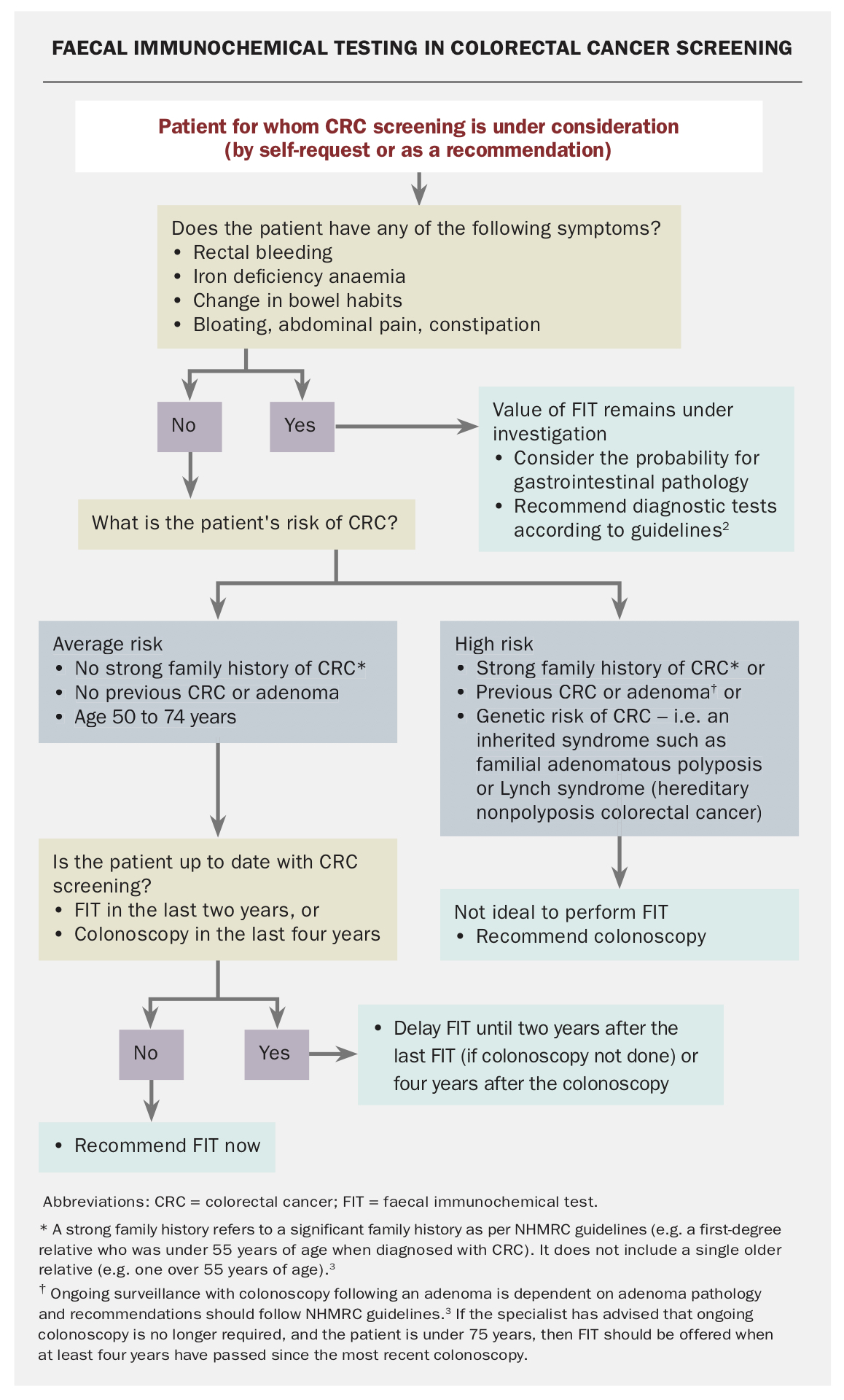
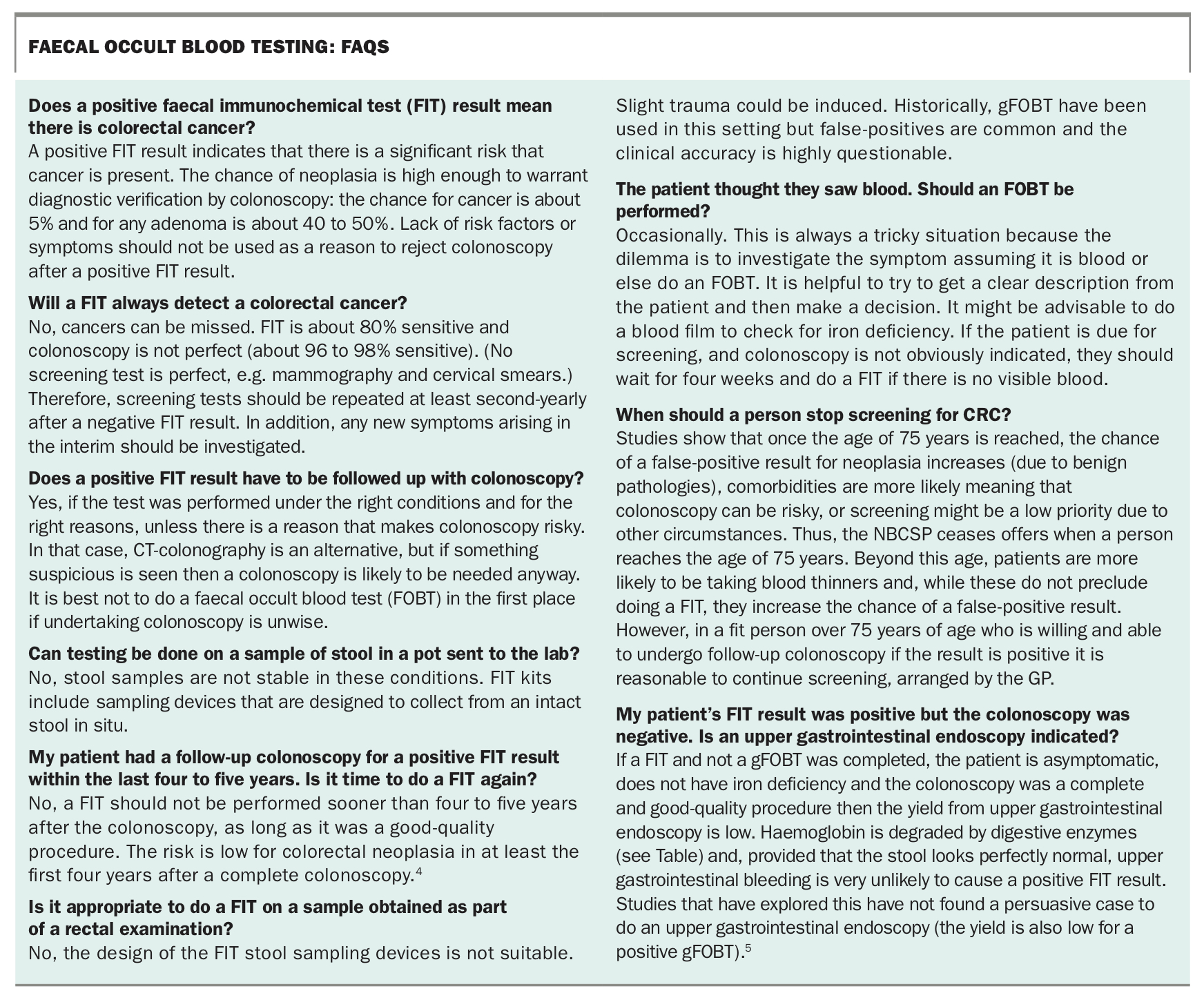
The indications for use of FITs are summarised in the Flowchart on page 41.2,3 Examples of questions that may arise in particular clinical scenarios are discussed in the Box on page 42.4,5
{kind=link}
{kind=link}
FITs for CRC screening: a major use
The use of FOBTs in practice for CRC screening is strongly supported by multiple randomised controlled trials. More than 40 countries use FITs for this purpose. Only a few countries continue to use gFOBT.6,7
The best FITs detect CRC with about 80% sensitivity and 92 to 95% specificity8 – excellent performance figures for a screening test that detects cancer (and for which overdiagnosis has not been documented). These performance characteristics lead to earlier detection of CRC, and reduced risk of death from CRC by around 50% in those who do the test.9
FITs are capable of detecting a proportion of precancerous advanced adenomas, although sensitivity is lower at 30 to 40%.8 Any detection and subsequent removal of adenoma facilitates a reduction in incidence of CRC due to FIT, which is supported by case-control studies.7
In Australia, the typical target population for screening is:10
- people with average risk for CRC (i.e. lacking risk factors based on personal or family history), and
- without symptoms suggestive of CRC, and
- aged 50 to 74 years.
In practice, people tend to participate in population screening whether or not they have symptoms or risk factors unless screening is personally managed by a health professional. Ideally, a screening program recommends consultation with a doctor to determine if just doing a FIT is adequate for the circumstances, such as when risk factors or symptoms are apparent. Symptoms should guide appropriate investigations. Patients with recent-onset rectal bleeding and patients found to have iron deficiency (if not menstruating) are the most predictive settings for CRC.2
The NBCSP offers a biennial (second-yearly) quantitative FIT that has been extensively studied and used worldwide. A person who has recently done a FIT and has no neoplasia at colonoscopy should normally wait two years before doing the next FIT.
FITs for high-risk subjects: a potential fallback option
People with risk factors for CRC (personal or family history) who meet guidelines for colonoscopy should be offered colonoscopy.3 If colonoscopy is refused, doing a FIT is better than nothing as long as the individual will agree in advance to proceed to colonoscopy if the result is positive.
FITs for symptomatic subjects: a triage option under evaluation
Apart from symptoms of rectal bleeding and iron deficiency, gastrointestinal symptoms such as constipation, abdominal distension and abdominal pain are not very specific for CRC and it can be difficult to decide at times if colonoscopy is needed.2 Studies are underway in symptomatic cases (those without visible bleeding) to determine if a FIT might triage who is of higher priority to proceed to colonoscopy.11 This is especially being considered in jurisdictions where colonoscopy resources are limited.
gFOBT – not useful, outdated and superseded for screening
The gFOBT has little if any place nowadays because it is less sensitive for colorectal bleeding and colorectal neoplasia, subject to false-positives due to diet and drugs, and less effective at reducing CRC mortality than are FITs.
Historically, the gFOBT has been used to test if blood is present in dark stools that might represent melaena. However, given the possibility of false-positive results they are not useful for this purpose. Proper visual inspection can usually differentiate blood as a cause from other agents such as iron.
When should an FOBT not be used?
An FOBT should not be performed to ‘validate’ a positive FIT result. Neoplasms bleed intermittently and a repeated test might be negative. Clinicians should act on the result of the first test.
In addition, an FOBT should not be used in the following situations:
- people who are not fit for follow-up colonoscopy if the test were to be positive
- people who are not prepared to undergo colonoscopy if they return a positive result. Always explain that the chance of a positive result when screening is about 7% (using tests with specifications such as those used in the NBCSP)
- people who have seen blood in the stools. To investigate dark stools a proper visual inspection is useful
- people with comorbidities and diseases that have a higher priority, particularly those aged over 75 years and especially if they are taking drugs that might produce gastrointestinal bleeding7
- people under 40 years of age without risk factors for CRC and without symptoms of concern. These are often the ‘worried well’. It is helpful to counsel them by explaining their risk for having a CRC now compared to the risk of a complication from colonoscopy. While the latter is low, it is higher than the risk of CRC being present.
Conclusion
CRC screening in average-risk subjects is the near-exclusive indication for use of an FOBT (ideally a FIT). Patients should sample the stool themselves using the instructions provided with the test kit. If a positive result is returned, diagnostic evaluation of the colon and rectum is essential. MT
Bowel cancer screening and COVID-19
Advice from the authors of this article on bowel cancer screening and the COVID-19 pandemic is provided in the Box.
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.