Cognitive bias and failure to diagnose: when you need to 'think slow'

Medicolegal medicine
Articles in this series highlight common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, the series is based on actual cases, with details changed for privacy. This case study explores factors that led to misdiagnosis of an ectopic pregnancy and presents tips for avoiding errors in reasoning and cognitive biases.
The diagnostic process is often said to exemplify the interplay between the art and science of medicine. Clinicians are required in their everyday work to use their expertise and skill to accurately execute the diagnostic process. When patients present with a problem, clinicians often respond intuitively, sometimes even without conscious effort. But sometimes this intuitive, ‘fast thinking’ can lead them astray.1
Diagnostic error is defined as the failure to establish or to communicate an accurate and timely explanation of the patient’s health problem(s).2 Diagnostic error is sometimes founded in the failure to understand or to consciously activate effective cognitive clinical reasoning skills. As not all diagnostic errors lead to harm, it is important to differentiate diagnostic error from misdiagnosis-related harm.3 Many biases can come into play during the diagnostic process and derail a timely diagnosis.
The following case study describes a woman with an ectopic pregnancy who was misdiagnosed with a urinary tract infection (UTI) and subsequently had her fallopian tube removed, potentially affecting future fertility. It was alleged this outcome might have been avoided with an earlier diagnosis. The study explores the processes of clinical reasoning and considers how cognitive biases may have led to diagnostic error in this case. Tips for GPs on how to activate analytical thinking processes and help avoid such errors are also presented. Although the case involves a GP and gynaecologist, the analysis focuses on the GP’s actions.
Case study
Karen, aged 39 years, had a long history of endometriosis, irritable bowel syndrome and difficulty becoming pregnant. She was undergoing in vitro fertilisation (IVF) under the care of her gynaecologist, Dr Jones. In 2015, she underwent an embryonic transfer.
Ten days after the transfer, Karen developed vaginal bleeding with some clots and mild pain. She thought that the procedure was unsuccessful and that she was miscarrying. She contacted Dr Jones, who agreed with her conclusion. She was told to go to hospital if her condition worsened. A blood test organised that day showed a beta human chorionic gonadotrophin (HCG) level of 100 mIU/mL (indicating pregnancy but relatively low).
Three days later (13 days after the embryonic transfer), Karen went to see Dr Jones and described some urinary frequency, dysuria and pelvic pain. She had no fever. The vaginal bleeding had stopped. Dr Jones prescribed an antibiotic for a suspected UTI and sent a urine sample for pathology testing. Dr Jones also requested another beta HCG measurement, but Karen did not attend to this as she thought the miscarriage was complete because she had stopped bleeding.
Three weeks after the transfer, Karen went to see her GP, Dr Small. She complained of lower abdominal pain and discomfort and told him that ‘the UTI had come back’. She told him that her recent IVF procedure had failed, that she had fully miscarried, and that this was complicated by a UTI for which she had recently finished prescribed antibiotics. Dr Small examined her. Her blood pressure was normal. Her temperature was slightly raised at 37.7°C and she had slight tachycardia (heart rate of 100 beats per minute). She had no loin tenderness, but did have tenderness across her lower abdomen and pelvis that was slightly worse on the right side. She had no rebound tenderness.
Dr Small thought that Karen had a continuing UTI. He asked her whether she thought she was pregnant, and Karen replied she was not and that she had been reviewed by Dr Jones. Dr Small obtained the urine result from Dr Jones’s office, which showed mild pyuria, haematuria, more than 100 epithelial cells per high power field, and no microbial growth on culture. Dr Small advised Karen to have a repeat urine culture in two weeks and prescribed another course of the same antibiotic. He suggested simple analgesics for pain and told her to come back or go to hospital if she became worse.
A week later Karen presented to another medical centre as the pelvic pain had worsened and the vaginal bleeding had started again. A pregnancy test was positive. Following contact with Dr Jones, she was admitted to hospital for treatment of an ectopic pregnancy. The right fallopian tube had to be removed.
Karen subsequently commenced legal proceedings against Dr Small and Dr Jones, alleging failure to diagnose and treat her ectopic pregnancy and consequent loss of the opportunity for conservative management of the pregnancy with methotrexate. It was alleged that an earlier diagnosis and treatment with methotrexate might have allowed her fallopian tube to be conserved and avoided effects on her future fertility.
Discussion
Clinical reasoning, cognitive biases and the diagnostic process
Good clinical reasoning is the quintessential sign of clinical competency. It involves dealing with judgement and uncertainty, and balancing benefits, risks and harms of treatments and investigations. Although clinicians do not require diagnostic certainty to be able to initiate treatment, they nevertheless must be able to ‘reduce diagnostic uncertainty enough to make optimal decisions for subsequent care’.2
Sources of diagnostic error
The diagnostic process is an iterative, complex, patient-centred and collaborative activity that is open to error in any of its steps.2 Error is rarely due to one reason or one break in the process. In any case that involves diagnostic error, there may be many different causes, ranging from system causes to patient-specific and personality factors, professional bias, personal bias, financial and nonfinancial conflicts of interest and cognitive errors in clinical reasoning.2 In this article, we concentrate on the cognitive process and biases that may lead to diagnostic error.
Analytical versus nonanalytical thinking
Although research shows that knowledge remains the key determinant of diagnostic accuracy, a theory that helps explain clinical reasoning is the dual process theory.2,4 This theory differentiates two types of thinking: analytical (slow or system 2) thinking and nonanalytical (fast, system 1) thinking.
Analytical thinking involves the use of critical thinking and deductive and counterfactual reasoning skills, as well as hypothesis evaluation. It is slow and takes time and is based on sound knowledge as a prerequisite.2 Traditional teachings, such as the need to always formulate a differential diagnosis, are a good way of forcing us into this analytical thinking mode.
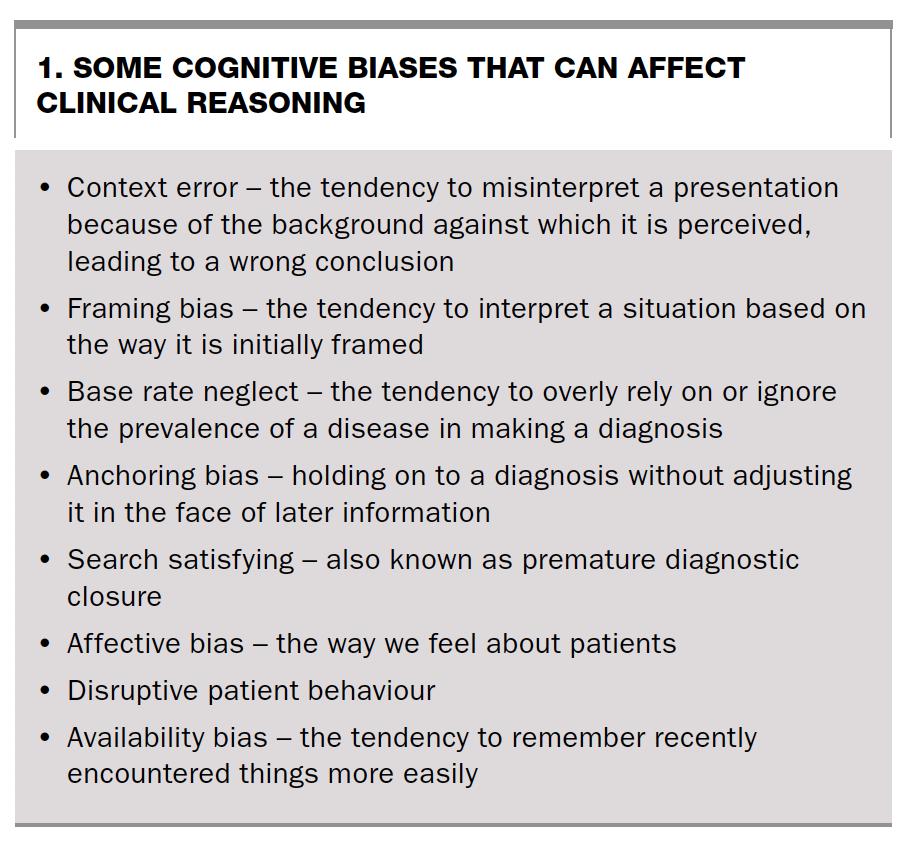
In contrast, nonanalytical thinking is a process that requires little working memory. It is fast, intuitive and automatic. It involves the conscious or subconscious use of heuristics (mental short cuts) to facilitate decision-making. Failure of heuristics, referred to as cognitive bias, often leads to error.2 Some types of cognitive bias that can affect clinical reasoning and lead to diagnostic errors are described in Box 1.
{kind=link}
Cognitive biases and Dr Small
Ectopic pregnancies can be difficult to diagnose, as the presenting symptoms and their timing can be nonspecific and vary.5 Most GPs know the theory and typical presentation of a UTI and an ectopic pregnancy, and are aware that a urine pregnancy test should always be performed to exclude pregnancy in a woman of reproductive age presenting with pelvic pain or abnormal vaginal bleeding. They also know how difficult it is to differentiate the multitude of causes of pelvic pain in female patients. A detailed review of these causes is beyond the scope of this article.
Nevertheless, with the benefit of hindsight, a number of crucial errors in Dr Small’s reasoning process and cognitive biases can be seen.2 These include the following.
- Context error. It is easy to think, like Dr Small, that a patient presenting with lower abdominal pain and a history of urinary-type symptoms has a problem that involves the urinary tract.
- Framing bias. The patient presented with a focus on the UTI for which she had just been treated and told Dr Small that her miscarriage had been ‘completed’. Dr Small did not analyse or assess the likelihood of this conclusion being correct.
- Base rate neglect. Dr Small perhaps relied on the fact that UTIs are much more common than ectopic pregnancies and did not further investigate the possibility of an ectopic pregnancy.
- Anchoring bias. From the outset, Dr Small’s working diagnosis was a UTI. He did not reassess the diagnosis when he received the previous urine culture result that showed a probably contaminated urine sample and no microbial growth on culture.
- Search satisfying. Premature diagnostic closure could also have been a factor affecting Dr Small’s cognitive reasoning.
Although not observed in this case, numerous other biases can affect cognitive reasoning. These include:
- affective bias (the way we feel about patients), which can certainly affect judgement
- disruptive patient behaviour, which has been shown to affect diagnostic accuracy and doctors’ performance6
- availability bias (Box 1).
- In addition, individual doctor characteristics (e.g. age, affect, experience, personality and overconfidence) can influence the rate of diagnostic error.
Outcome
Expert evidence was sought and suggested that even though Dr Small examined the patient, he did not adequately form a differential diagnosis or use adequate clinical reasoning to discharge his duty of care to act reasonably in the circumstances. Namely, he did not question or formulate a differential diagnosis and did not perform a pregnancy test or any tests to confirm his provisional diagnosis of a UTI. The case was settled out of court.
Risk management
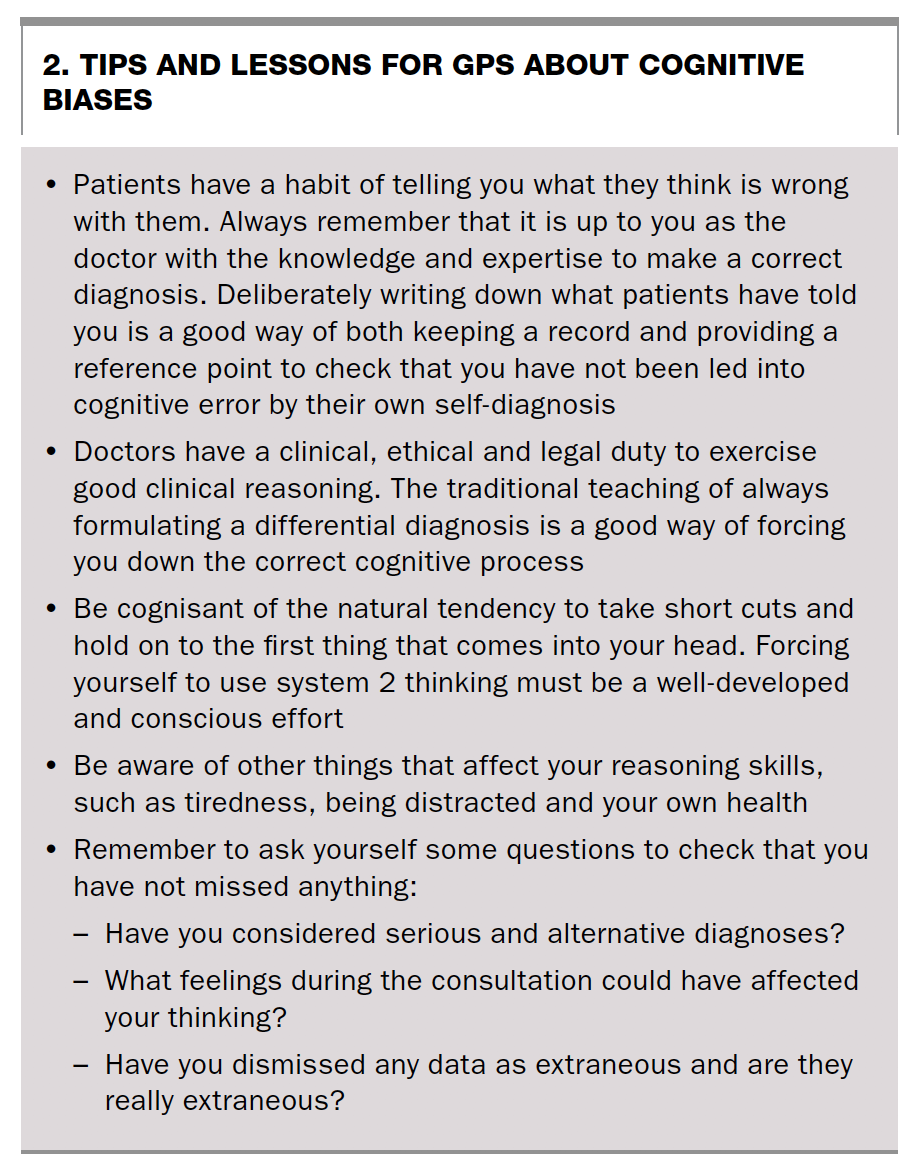
Case studies such as this provide lessons for all doctors. Tips on risk management and lessons about cognitive biases for GPs are summarised in Box 2. It is always easy to judge a case with the benefit of hindsight, and always easier to see bias when we know something has gone wrong.7 However, a good understanding of clinical reasoning skills, which are often subconscious, is important to continuous improvement. Focusing on cognitive skills, potential heuristic biases and the factors that can affect clinical reasoning should improve clinical safety and patient outcomes. Forcing oneself into system 2 ‘slow’ thinking is a skill that can be developed with practice and experience. MT
{kind=link}