Why not write yourself a script? The risks of self-prescribing

This series highlights common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, the series is based on actual situations, with details changed for privacy, and some issues summarised for discussion. This scenario is based on a reported decision of the Medical Council of New Zealand that highlights the risks of professional compromise when doctors prescribe for themselves.
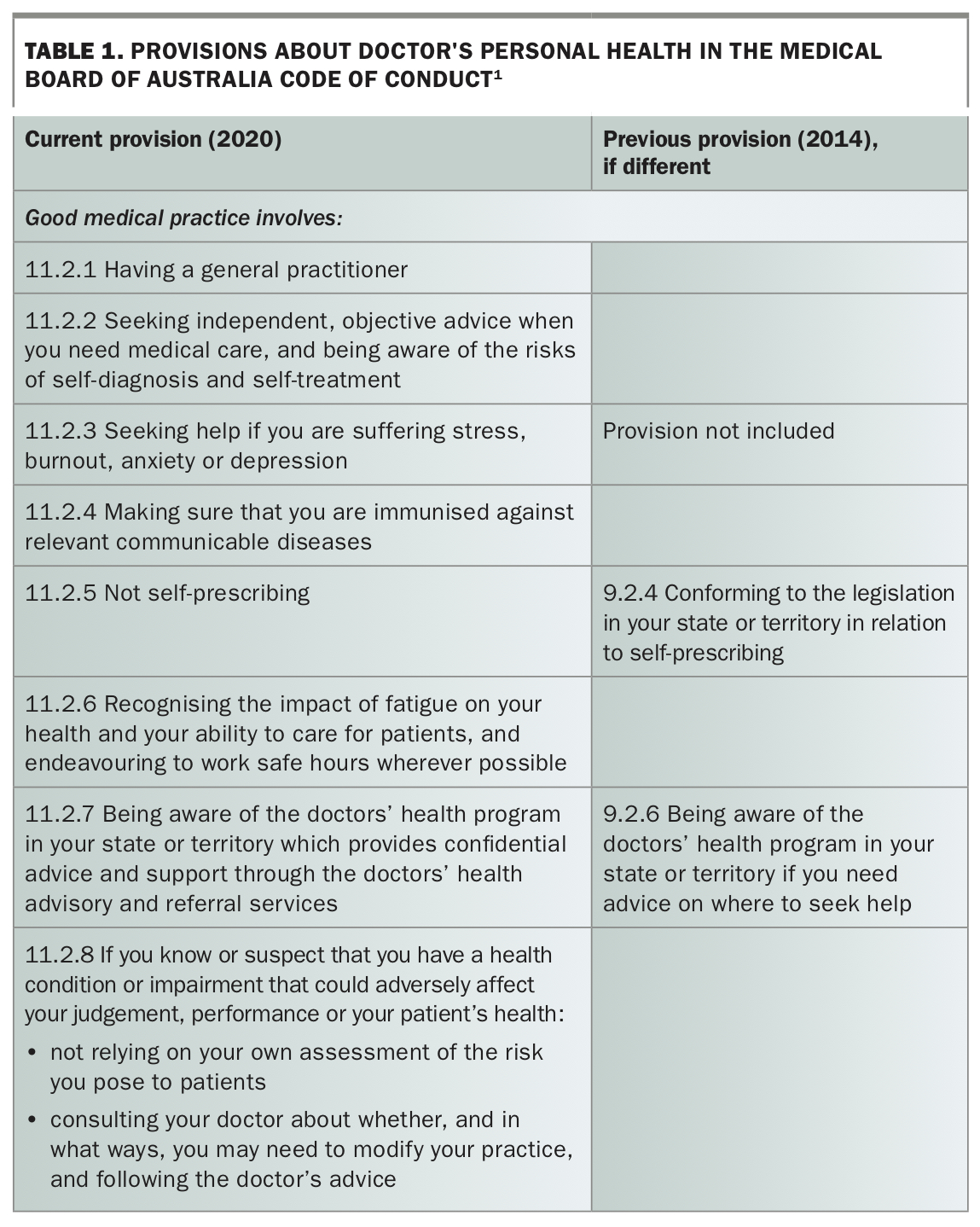
Self-prescribing can threaten the health and wellbeing of doctors and their patients. Legislation prohibits it in some cases, and professional codes of conduct have long warned against it. The most recent version of the Medical Board of Australia’s Code of Conduct is even more explicit than previous versions: good medical practice involves not self-prescribing (Table 1).1 Yet, as a recent New Zealand decision illustrates, the temptation to write themselves a prescription continues to catch doctors out.2
{kind=link}
Case scenario
Dr Amber, a GP, was reported to the Medical Council of New Zealand for self-prescribing and prescription fraud. She had been taking antianxiety and antidepressant medication prescribed by her own GP for several years. In late 2015, a pharmacist notified the Medical Council that he was concerned Dr Amber was self-prescribing zopiclone. When questioned by the Medical Council, Dr Amber explained she had been unable to see her GP over the holiday period and was anxious about running out of her medication. She assured the Medical Council this was a ‘one-off’ and that she understood her professional obligations about self-prescribing. The Medical Council took no further action at the time.
In 2017, she was again reported to the Medical Council for self-prescribing, this time by her employer. It emerged that over the past six years she had been self-prescribing medications, including restricted medications. She had also written prescriptions for drugs of addiction and psychotropic medications in the names of two family members, with the intention of consuming the medications herself.
The tribunal accepted that Dr Amber had admitted wrongdoing and shown insight and remorse. It found that after being reported, she had undertaken rehabilitation. It also accepted that Dr Amber’s personal situation had been particularly difficult. The tribunal found Dr Amber did not pose a risk to the public but determined that some deterrent penalty was required. Dr Amber was reprimanded, fined and had supervision conditions imposed on her registration.
Medicolegal issues
Legal restrictions on self-prescribing
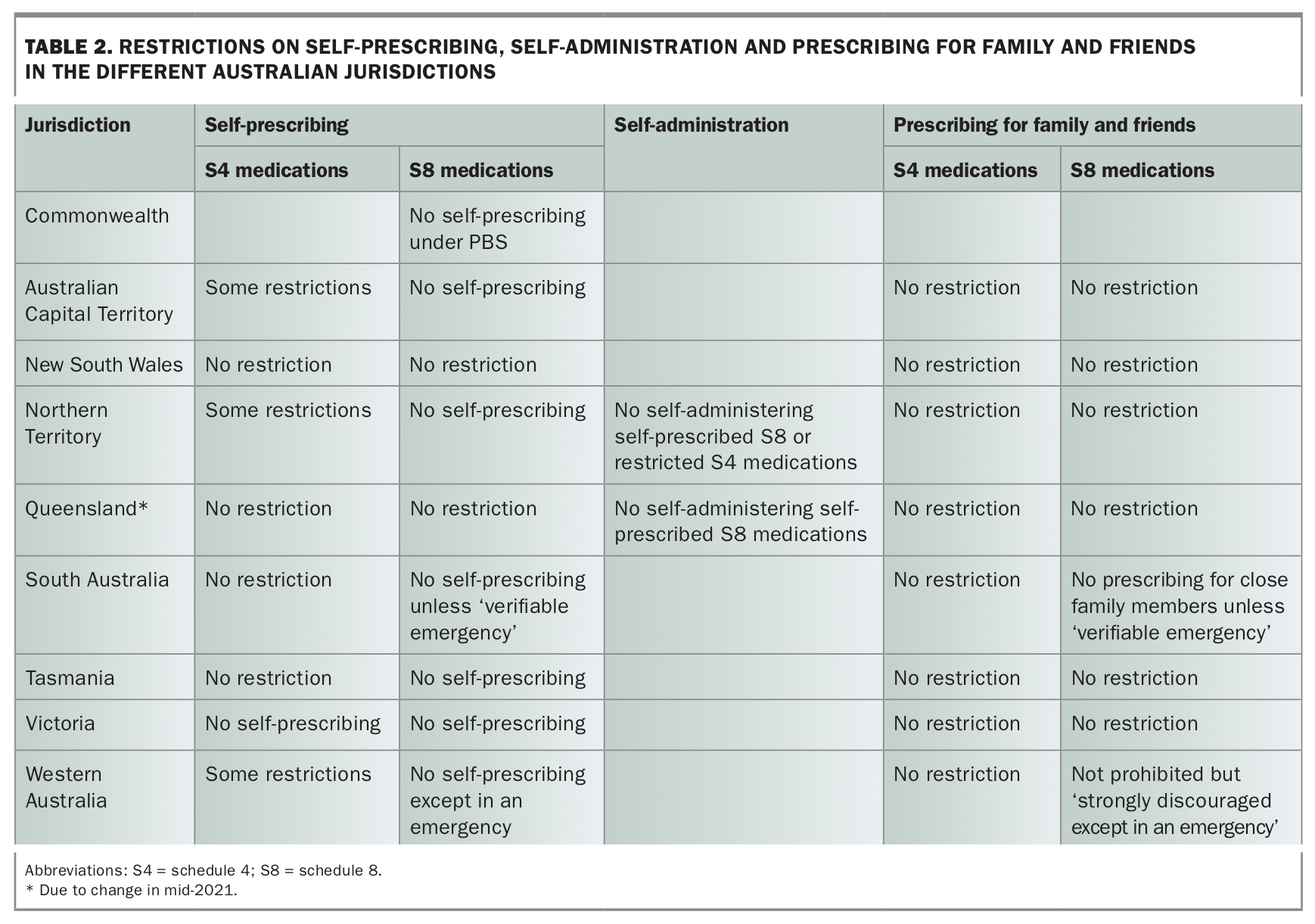
In Australia, both federal and state legislation regulates self-prescribing and self-administering medications. The strongest prohibitions apply to Schedule 8 (S8) medications. Doctors are not permitted to self-prescribe these under the national PBS. Self-prescribing S8 medications is expressly prohibited in all states and territories except NSW and Queensland, and will be prohibited in Queensland from mid-2021 (Table 2). Queensland and the Northern Territory also prohibit practitioners from self-administering S8 medications if these have been self-prescribed.
{kind=link}
In addition, Victoria prohibits self-prescribing Schedule 4 (S4) medications, and the Australian Capital Territory, Northern Territory and Western Australia have some restrictions on prescribing these medications. Interns cannot self-prescribe in the ACT, and certain types of S4 medications may not be self-prescribed in those jurisdictions.
Prescription fraud
To overcome prohibitions on self-prescribing, doctors are sometimes tempted to write the prescription in the name of another patient, such as a family member. There have also been reported cases where doctors have forged a colleague’s name on a prescription.
Breach of professional standards
Although this case took place in New Zealand, similar cases also occur in Australia, and the regulatory positions are similar. The Medical Board of Australia has long warned doctors against self-prescribing. Previously, the Board’s Code of Conduct reminded doctors they needed to abide by relevant legislative provisions on self-prescribing. The current version of the Code, updated as of October 2020, simply says good medical practice involves not self-prescribing (Table 1).1 Further, if self-prescribing also involves prescription fraud, that could lead to an investigation regarding whether the actions amount to professional misconduct or unprofessional conduct.
Professional harm to colleagues
In this case, Dr Amber was self-prescribing in addition to the medications her GP was prescribing. That meant her GP was unaware of the dosages she was taking. The tribunal pointed out this could have led the GP to provide inappropriate treatment, potentially putting his professional reputation at risk.
In another recent case, a doctor forged a colleague’s name on prescriptions to conceal that the doctor was prescribing for himself and his family.2 A pharmacist reported the prescribing as unsafe, and the colleague, whose name was on all the prescriptions, had his prescribing rights suspended and his prescribing practices investigated by the regulator.
The tribunal was clear that putting professional colleagues at risk in this way is also a breach of a doctor’s professional obligations to their colleagues.
Discussion
Self-treatment and risk of harm
The Board’s Code of Conduct warns doctors against providing medical care to those with whom they have a close personal relationship because of the lack of objectivity and risks to both patient and doctor.1 The risk of lack of objectivity is even greater when doctors are diagnosing, treating or prescribing for themselves.
The Australian Medical Association, medical colleges, regulators and doctors’ health organisations consistently state that doctors should have their own treating GP.3-6 The medical literature is also consistent in pointing out the risks of self-treatment.7,8
Doctors treating themselves may be unable to assess their own condition objectively, which can lead to missed or delayed diagnoses. Conflicting pressures and commitments may mean they do not seek or receive proper care. Self-treatment is more likely to be delayed or inappropriate. In a UK study, a panel of seven practitioners considered care provided by 275 GPs who reported having self-prescribed and self-referred. The panel concluded the GPs’ self-treatment had been inappropriate in 78% of cases, and the self-referrals were also significantly more likely to have been inappropriate.9
Having a regular healthcare provider also increases the likelihood of doctors receiving preventive health care.10
When cases of self-prescribing come before regulators and professional standards bodies, it is commonly reported that the stress of trying to manage, and conceal, their condition without support has made the doctor more unwell. This is particularly true for doctors self-prescribing in the context of an unmanaged addiction. As in the case described above, when the condition comes to light and the doctor begins to receive support, their condition often improves.
As Dr Amber herself put it, ‘Ironically, I am glad that all of this is out in the open now. I feel like a weight has in some way been lifted off my shoulders’. She told the tribunal she began self-prescribing the medications prescribed by her GPs because she was afraid she would run out. As her anxiety and other symptoms, including migraines and difficulty sleeping, escalated over the years, her self-prescribing also escalated. This enabled her to conceal the extent of her difficulties from her GP. It was not until she was reported to the regulator that she received appropriate assistance, including care from a psychologist, and was able to develop coping strategies. With treatment she was managing to reduce her medication.
Risk to patients
Doctors who are ill and not receiving appropriate treatment may also be putting the health of their patients and others at risk. If a doctor’s self-prescribing means an underlying mental illness or addiction issue is going unmonitored and unsupported, this can impair their ability to care for patients. Examples from other cases include doctors not recognising physical side effects, such as tremors, as caused by medication.11
More generally, the link between doctors’ wellbeing and the quality of patient care is well documented. Doctors who are experiencing burnout, stress or other health problems are more likely to make errors.12
Further, doctors who are self-prescribing sometimes write prescriptions in another person’s name, such as a family member or a patient, to avoid detection. In the case described above, the tribunal accepted that there was no sign that Dr Amber’s professional performance had been impaired or that she had directly harmed patients. However, it did point out her prescribing had the potential to harm a number of others as well as herself. The record of prescriptions in the names of family members meant their medication records were inaccurate, and they were potentially at risk of medication error or inappropriate treatment.
Mandatory reporting
Doctors may fall into self-prescribing out of embarrassment about a condition, or possibly out of fear that a treating doctor would be required to report them as being impaired.13 Fear of mandatory notification should never be a reason to avoid seeking help.
Treating practitioners are required to make a mandatory notification only if they form a reasonable belief in the course of treating another practitioner that their practitioner-patient is practising with an impairment and placing the public at substantial risk of harm. Ahpra is very clear that this is a very high threshold. Even if a practitioner is impaired, there is no need to report them if there are effective controls to manage the impairment and reduce the risk and severity of harm to the public. This could be, for example, treatment, a break from practice, modified scope of practice or other strategies to manage the impacts of the impairment.
Under the Health Practitioner Regulation National Law, a treating practitioner would rarely be required to notify on the grounds of impairment if their practitioner-patient’s illness is being treated and well managed.14-16
Conclusion
The research on doctors’ self-prescribing concludes that the practice is widespread. There seems to be acceptance, even an expectation among medical professionals, that doctors will self-treat for minor or acute issues. The research also reports on barriers that prevent doctors having a regular GP. Some of these are practical: time and geography. Others are psychological: embarrassment, not wanting to bother someone else, and fear of being reported for having an impairment. Nevertheless, the Medical Board insists doctors seek professional health care and avoid the temptation to treat themselves. The case described illustrates some of the reasons why this is important. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.