Diagnosis and management of primary Sjögren’s syndrome

Sjogren's syndrome
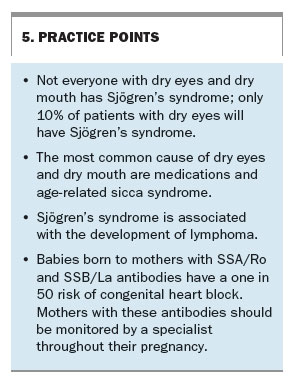
Not everyone with dry eyes and dry mouth has Sjögren’s syndrome; the differential diagnosis is broad, and patients with this condition present with a wide range of symptoms and spectrum of disease. The prognosis is largely determined by the extent of systemic disease, although exocrine manifestations can have a severe impact on a patient’s quality of life.
Sjögren’s syndrome is a common autoimmune disorder characterised by the destruction of lacrimal and salivary gland function leading to the classic symptoms of keratoconjunctivitis sicca (dry eyes) and xerostomia (dry mouth).1 It can occur alone in primary form, which will be discussed here, or in a secondary form with other rheumatological diseases, most commonly rheumatoid arthritis but also others such as systemic lupus erythematosus (SLE), systemic sclerosis or an inflammatory myopathy.2
The cause of primary Sjögren’s syndrome is unknown, and as with most autoimmune disorders, both environmental and genetic factors play a role. The underlying pathogenesis is characterised by a cellular infiltrate (predominantly CD4+ T lymphoctyes) that leads to destruction of the lacrimal and salivary glands. Inhibitory antibodies against muscarinic receptors and a general cytokine milieu causing accelerated breakdown of neurotransmitters both contribute to reduced stimulation of secretions.3
Epidemiology
Primary Sjögren’s syndrome is common, affecting 0.5 to 1% of the population.4,5 It has a strong female predominance (9 to 1) with a peak incidence in the fourth to sixth decades, and is found worldwide, with the highest incidence rates occurring in Europe and Asia.5 It is worth noting that although primary Sjögren’s syndrome may occur at any age, the incidence decreases in patients over 65 years, an important consideration when considering a diagnosis of primary Sjögren’s syndrome in the elderly.6,7
Clinical manifestations
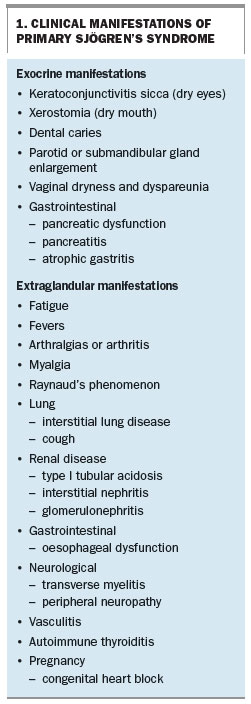
The clinical manifestations of primary Sjögren’s syndrome can be divided into exocrine and extraglandular features, which are summarised in Box 1.
{kind=link}
The prognosis remains variable. It is largely determined by the extent of systemic disease although the exocrine manifestations can have a severe impact on a patient’s quality of life.8
Exocrine manifestations
The most common exocrine features, occurring in more than 95% of patients, include keratoconjunctivitis sicca and xerostomia, known together as the ‘sicca syndrome’. Most patients will complain of dry, gritty, itchy or painful eyes. Severe keratoconjunctivitis sicca can lead to infection, ulceration and visual loss. Wearing contact lenses is contraindicated in patients with severely dry eyes.
Lack of saliva may cause difficulty with swallowing or speech, and patients may report altered taste sensation. Oral Candida infection is common in patients with xerostomia. Oral dryness also contributes to dental caries, and regular dental review is essential. Enlargement of salivary glands, predominantly the parotid and submandibular glands, can be seen in patients with more severe xerostomia.
Extraglandular manifestations
A third of patients with primary Sjögren’s syndrome report extraglandular symptoms, the most common being fatigue, arthralgias, myalgias and low-grade fever. The skin may be affected by hypersensitivity vasculitis. Clinically, some patients’ symptoms may resemble those of SLE.
Renal manifestations include interstitial nephritis, and there is an association between Sjögren’s syndrome and distal (type 1) renal tubular acidosis. This is seen in up to 25% of patients and can result in a mild metabolic acidosis and potassium wasting.
The risk of patients with primary Sjögren’s syndrome developing non-Hodgkin’s lymphoma has been shown to be up to about 40 times that of the general population, although it is still uncommon.9,10 Persistent lymphadenopathy must be investigated. The risk factors include splenomegaly, glomerulonephritis, hypocomplementaemia, monoclonal gammopathy, cryoglobulinaemia and neutropenia.11 The most important clinical risk factor for the development of lymphoma is persistent salivary gland enlargement.12
Although less common, primary Sjögren’s syndrome may initially be confined to one organ system. For example, a patient may have an isolated neuropathy or a persistent dry cough in the setting of lung fibrosis. With such a patient, appropriate questioning regarding sicca symptoms and subsequent investigation as outlined below become vital in establishing the underlying diagnosis.
Diagnosis
Primary Sjögren’s syndrome should be suspected in patients presenting with symptoms of ocular or oral dryness, enlarged parotid glands or significant dental caries without adequate explanation. Confirmation of the diagnosis requires objective evidence of dry eyes and/or dry mouth with evidence of underlying autoimmunity and the exclusion of secondary causes.
Ocular assessment should include an evaluation of tear production using the Schirmer test and ocular surface staining using rose bengal or fluorescein drops. A Schirmer test showing less than 5 mm of wetting in five minutes in either eye is supportive of a diagnosis of primary Sjögren’s syndrome. If ocular surface staining shows severe keratoconjunctivitis sicca or substantial corneal abrasion, the patient should be referred immediately to an ophthalmologist.
Oral dryness can be objectively determined by measuring the patient’s unstimulated salivary flow rate. One method requires the patient to empty their saliva into a cup over five to 15 minutes. A collection of 0.1 mL/min or less is a positive test result. The patient must not have eaten, chewed gum or drunk water for the 90 minutes before the test. Other methods include the Saxon test, which requires the patient to chew on a sponge for two minutes without swallowing; a change in weight of the sponge of less than 2.75 g is indicative of xerostoma. Formal testing of oral dryness is rarely performed in clinical practice.
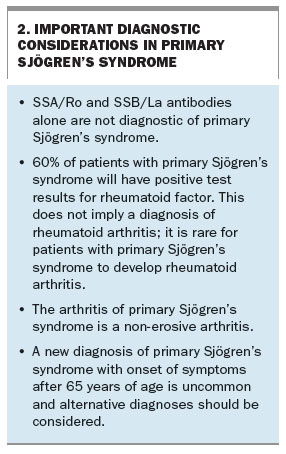
Serologically, most patients (80%) with primary Sjögren’s syndrome test positive for antinuclear antibodies. Antibodies to the extractable nuclear antigens SSA/Ro and SSB/La will be detected in 65% and 55% of patients, respectively. Rheumatoid factor will be detected at low titre in 60%.
In patients who are strongly suspected of having primary Sjögren’s syndrome but who lack SSA/Ro or SSB/La antibodies, a labial salivary gland biopsy may aid in diagnosis.2 Patients must be made aware that up to 2% of people who undergo this procedure may be left with persistent lip numbness.13 The typical histological finding is a focal collection or collections of tightly aggregated lymphocytes in periductal distribution.
Correct diagnosis is crucial, as misdiagnosis with another connective tissue disease such as rheumatoid arthritis or SLE can result in inappropriate treatment and morbidity. Further, it allows appropriate monitoring for complications (see below), as well as consideration of emerging therapies currently in clinical trials. Initial investigations should include a full blood count, renal and liver function tests, serological testing for inflammatory markers, antinuclear antibodies and extractable nuclear antigen antibodies, and urine testing for proteinuria and/or haematuria. If there is evidence of autoimmune disease then consider double- stranded DNA antibodies, rheumatoid factor, complement and immunoglobulin levels before referring, but these do not need to be repeated annually as part of routine monitoring.
Important diagnostic considerations in Sjögren’s syndrome are summarised in Box 2.
{kind=link}
Differential diagnoses
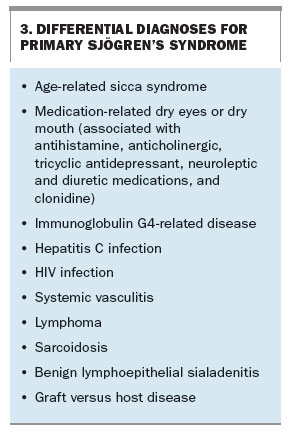
The differential diagnoses when primary Sjögren’s syndrome is being considered are broad and are summarised in Box 3.
{kind=link}
The most common differential diagnosis is medication-related dry eyes or dry mouth, especially in the elderly. Age-related sicca syndrome results in reduced saliva and tear formation, and is common. It can be differentiated from primary Sjögren’s syndrome by the absence of systemic features, unremarkable histological findings and normal results for serological testing.
Other differential diagnoses include infections such as hepatitis and HIV, inflammatory conditions such as immunoglobulin G4-related disease and vasculitis, and uncommonly but importantly lymphoma and other malignancies.
Treatment
As with the clinical manifestations, management of primary Sjögren’s syndrome may be divided into treatment of glandular and extraglandular features.
Treatment of glandular manifestations
Management of dry eyes and dry mouth is aimed at reducing symptoms. Patients should be given general education regarding lifestyle and environmental modification (Box 4).
{kind=link}
It is essential to treat coexisting blepharitis (inflammation of the meibomian glands) with warm compresses and massage. Eye drops and lubricant ointments should be used as frequently as required to obtain relief. Preservative-free preparations are preferable in patients who require more than four applications per day. Ointment is particularly useful at night when applied before sleep. For patients with severe dry eyes, consider referral to an ophthalmologist, who may prescribe cyclosporin eye drops or recommend nasolacrimal punctal occlusion procedures. Lifitegrast (lymphocyte function-associated antigen 1 antagonist) is a new artificial tear that was approved by the FDA in the USA in July 2016 for the treatment of symptoms and signs of dry eye disease; it is not available in Australia.
The management of dry mouth requires attention to oral hygiene and regular dental review. For patients with mild disease, frequent small sips of water may be sufficient for comfort. Sugar-free gum or mints, oral wetting agents and saliva substitutes are also available. The oral cavity should be monitored for the development of oral candidiasis. It is important in elderly patients to look under dentures for Candida infection. Use of topical fluoride to prevent dental caries is strongly recommended. Severe dry mouth may lead to ulceration and scarring, and specialist referral for consideration of pilocarpine (off-label use) is suggested. Treatment of nasal congestion to avoid mouth breathing may help to alleviate the symptom.
Treatment of extraglandular manifestations
Corticosteroids and other immunosuppressants do not improve the sicca symptoms in primary Sjögren’s syndrome, so their use is limited to patients with extraglandular disease. Management should be organ-specific. Fatigue may be managed similarly to the fatigue in fibromyalgia but care needs to be taken with drugs that may exacerbate sicca symptoms, such as tricyclic antidepressants. NSAIDs are useful for patients with arthritis. Hydroxychloroquine is used for both arthritis and skin manifestations and may help with fatigue. Methotrexate may be required for patients whose arthritis remains symptomatic despite the use of hydroxychloroquine.
Patients with cardiopulmonary, renal or other internal organ involvement require specialist review and immunosuppression, often with a combination of prednisone and azathioprine, mycophenolate (off-label use) or cyclophosphamide. More recently, rituximab has been shown to be useful in treating the extraglandular manifestations in patients who are resistant to other therapies (off-label use).14
Monitoring and when to refer
Patients with mild disease limited to oral and ocular dryness may be followed up annually by their general practitioner. Regular dental and optometry review is essential. For patients with more severe symptoms or extraglandular manifestations of Sjögren’s syndrome, regular follow up by a rheumatologist is advisable.
Routine review should consist of examination of the eyes and mouth looking for local complications of disease, as well as a peripheral lymph node examination. Annual blood tests should include a full blood count, liver and renal function tests and inflammatory marker levels. For patients with progression of symptoms or poor prognostic markers of disease, repeat immunological tests should be considered. Women of childbearing age with positive SSA/Ro or SSB/La antibodies should be informed of the risk of congenital heart block before conception and should be monitored by a specialist from 16 weeks’ gestation onwards, including use of fetal echocardiography.
Conclusion
Primary Sjögren’s syndrome is a common autoimmune disorder with a wide range of symptoms and spectrum of disease, from patients with mild dry eyes and mouth to patients with severe systemic involvement requiring immunosuppression. Co-ordinated care between the general practitioner, ophthalmologist, rheumatologist and dentist is essential to optimising patient care.
Practice points are listed in Box 5.
{kind=link}
MT
COMPETING INTERESTS: None.
References
- Ramos-Casals M, Tzioufas A, Font J. Primary Sjögren’s syndrome: new clinical and therapeutic concepts. Ann Rheum Dis 2005; 64: 347-354.
- Hochberg M, Silman A, Smolen J, Weinblatt M, Weisman M, eds. Rheumatology. 6th ed. Vol 1. Philadelphia: Elsevier Mosby; 2015.
- West S. Rheumatology secrets. 3rd ed. Phildelphia: Elsevier Mosby; 2014.
- Winer S, Astsaturov I, Cheung R, et al. Primary Sjögren’s syndrome and deficiency of ICA69. Lancet 2002; 360: 1063-1069.
- Qin B, Wang J, Yang M, et al. Epidemiology of primary Sjögren’s syndrome: a systematic review and meta-analysis. Ann Rheum Dis 2015; 74: 1983-1989.
- Watts R, Conaghan P, Denton C, Foster H, Issacs J, Muller-Ladner U, eds. Oxford textbook of rheumatology. 4th ed. Oxford University Press; 2013.
- Botsios C, Furlan A, Ostuni P, et al. Elderly onset ofprimary Sjögren’s syndrome: clinical manifestations, serological features and oral/ocular diagnostic tests. Comparison with adult and young onset of the disease in a cohort of 336 Italian patients. Joint Bone Spine 2011; 78: 171-174.
- Belenguer R, Ramos-Casals M, et al. Influence of clinical and immunological parameters on the health-related quality of life of patients with primary Sjögren’s syndrome. Clin Exp Rheumatol 2005; 23: 351-356.
- Zintzaras E, Voulgarelis M, Moutsopoulos H. The risk of lymphoma development in autoimmune diseases: a meta-analysis. Arch Intern Med 2005; 165: 2337-2344.
- Kassan S, Thomas T, Moutsopoulos H, et al. Increased risk of lymphoma in sicca syndrome. Ann Intern Med 1978; 89: 888-892.
- Giannouli S, Voulgarelis M. Predicting progression to lymphoma in Sjögren’s syndrome patients. Expert Rev Clin Immunol 2014; 10: 501-512.
- Voulgarelis M, Tzioufas A, Moutsopoulos H. Mortality in Sjögren’s syndrome. Clin Exp Rheumatol 2008; 26 (5 Suppl 51): S66-S71.
- Caporali R, Bonacci E, Epis O, Bobbio-Pallavicini F, Morbini P, Montecucco C. Safety and usefulness of minor salivary gland biopsy: retrospective analysis of 502 procedures performed at a single center. Arthritis Rheum 2008; 59: 714-720.
- Ramos-Casals M, García-Hernández F, de Ramón E, et al; BIOGEAS Study Group. Off-label use of rituximab in 196 patients with severe, refractory systemic autoimmune diseases. Clin Exp Rheumatol 2010; 28: 468-476.