Antimicrobial stewardship in the community: understanding the data

Associate Professor Buising is Deputy Director of the NHMRC-CRE National Centre for Antimicrobial Stewardship; Antimicrobial Resistance Theme Leader at the Peter Doherty Institute for Infection and Immunity; Director of the Victorian Infectious Diseases Service and Guidance Group at Royal Melbourne Hospital; and Associate Professor in the Department of Medicine, University of Melbourne, Melbourne. Dr Rajkhowa is Centre Manager of the NHMRC-CRE National Centre for Antimicrobial Stewardship, Melbourne. Professor Mazza is Head of the Department of General Practice, Monash University, Melbourne. Ms Hawes is a PhD Fellow at the NHMRC-CRE National Centre for Antimicrobial Stewardship and the Department of General Practice, Monash University, Melbourne, Vic.
Infection control
Bacterial infections
Australia has a higher per-capita consumption of antibiotics than Canada and many European countries and a higher average consumption than the OECD average. About 80% of antibiotic prescribing takes place in the community. Better data on antimicrobial prescribing behaviour might help identify opportunities for improved antimicrobial stewardship.
Case scenario
Xanthe, aged 55 years, presents to her GP as she has had a cough and has been feeling unwell for a few days. She also has a runny nose. The GP examines her, excludes pneumonia and diagnoses rhinitis and acute bronchitis. Xanthe does not smoke and is otherwise well. She reports that when she had bronchitis last winter, she was given amoxicillin, but was still coughing a few days later and was switched to amoxicillin-clavulanic acid. She recovered over the next week. This illness is like the previous one and she would like antibiotics again.
Case scenarios such as this can be common in general practice. What should the GP do?
- Option A: The GP gives Xanthe the prescription.
- Option B: The GP knows that acute bronchitis is caused by a virus in over 90% of cases and is usually self-limiting, and that antibiotic treatment is not recommended for acute bronchitis.1 The GP is also concerned about contributing to antimicrobial resistance. The GP explains to Xanthe that her illness is most likely due to a virus, and that a cold and cough such as this usually resolve over two to three weeks. The GP gives her a patient information leaflet on acute bronchitis from the Australian Commission on Safety and Quality in Health Care and discusses her options based on this leaflet.2 The GP explains that antibiotics may have side effects, and that she is likely to recover without these medications. The GP also tells her to look out for symptoms such as fever or a worsening cough and to come back if her condition worsens. Xanthe elects not to take antibiotics.
Option B represents the recommended approach and is an example of antimicrobial stewardship (AMS).
This article outlines current data on antimicrobial prescribing in the Australian community, which includes general practice, specialist outpatients and dental clinics and residential aged care facilities. It also suggests strategies that might enhance the quality of the data and antimicrobial prescribing practices.
What is antimicrobial stewardship?
AMS refers to principles and strategies that aim to optimise antimicrobial use. AMS should ensure that patients receive antimicrobial therapy that best treats or prevents infection and improves clinical outcomes, while balancing this against the potential harms of unnecessary or inappropriate antimicrobial use. These harms include adverse drug effects and the promotion of antimicrobial-resistant pathogens, both in the individual and in the population. Additionally, AMS should help promote cost-effective care.
Antimicrobial prescribing in the community
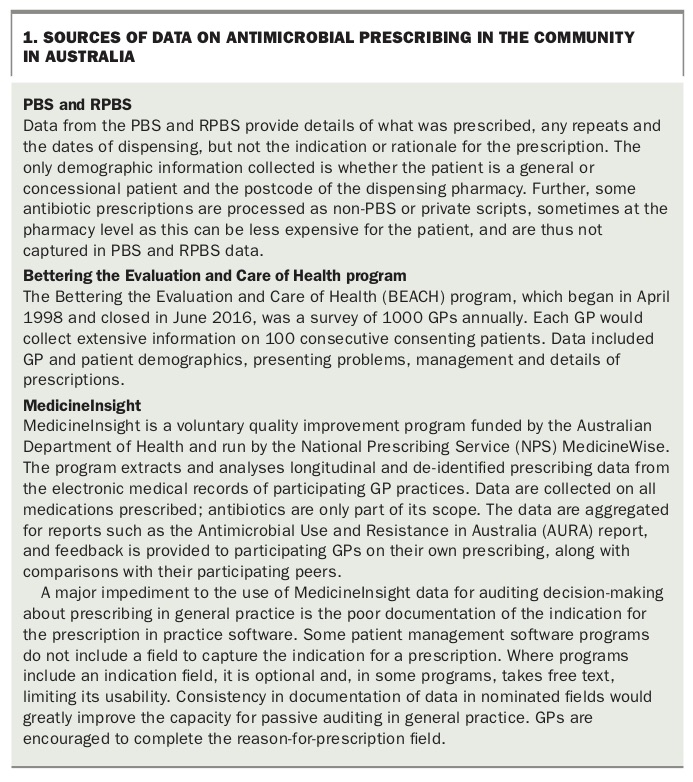
Australia has a high level of consumption of antibiotics, with higher per-capita consumption than Canada and many European countries.3 Average antibiotic consumption in Australia is higher than the OECD average.4 Most antibiotic prescribing (about 80%) takes place in the community. About 85% of the population visit a GP each year.5 We need to better understand antimicrobial prescribing behaviour in general practice to identify any opportunities for enhancing AMS. There are three main sources of data on GP prescribing in Australia, but all have limitations (Box 1).
{kind=link}
Analysis of PBS and RPBS data reveals that, in 2015, about 45% (10,701,804) of the Australian population was prescribed at least one systemic antibiotic.3 The most commonly prescribed systemic antibiotics were amoxicillin, cefalexin and amoxicillin-clavulanic acid. Winter increases were seen for amoxicillin, amoxicillin-clavulanic acid and roxithromycin. Patients younger than 5 years and older than 64 years together accounted for the highest proportion of antibiotic prescriptions.3
According to analysis in the 2017 AURA report, based on data extracted from the records of participating GP practices by the MedicineInsight program, 30% of patients in the 2015 dataset (968,259 out of 3,181,923) were prescribed systemic antibiotics each year.3 Older people were more likely to receive such a prescription. It must be recognised that only 23.5% of the records in MedicineInsight had an indication recorded, so any analysis that attempts to relate the prescription to the indication for use may be biased, and may not account for most prescribing.
Data from the BEACH program suggest that, between 2010 and 2015, about 60% of patients who presented to GPs with colds and other upper respiratory tract infections received a prescription for an antimicrobial agent.6 The report noted that prescribing rates were high for many conditions that do not usually require antibiotics.6
High usage of broad-spectrum agents such as amoxicillin-clavulanic acid and moderate-spectrum agents such as cefalexin in Australian general practice is a concern, given that these are listed in guidelines as second-line agents for most indications. Research by the National Centre for Antimicrobial Stewardship shows that, in a selected group of general practice clinics in Melbourne between 2010 and 2014, antimicrobial prescribing increased in winter.7 Where indications were recorded, this increase was associated with an increase in patients presenting with upper respiratory tract infections. Cefalexin, amoxicillin-clavulanic acid, roxithromycin, doxycycline and clarithromycin were the most frequently prescribed antibiotics, and all antibiotics except cefalexin were prescribed more often in winter.7 Our analysis suggests that guideline-nonconcordant prescribing of broad-spectrum antibiotics such as amoxicillin-clavulanic acid and of the macrolides may be common.
The Royal Australian College of General Practitioners’ Standards for general practices (5th edition) recommends that GPs follow Therapeutic guidelines: antibiotic for antibiotic selection and dose.1,8
Antimicrobial prescribing in residential aged care
The National Centre for Antimicrobial Stewardship is beginning to gather useful data to better understand prescribing practices in residential aged care facilities. The Aged Care National Antimicrobial Prescribing Survey (ACNAPS) has been undertaken nationally over four years (2015 to 2018). The resulting data feed into the AURA reports. The results of ACNAPS show that there is a high prevalence of antibiotic use for residents in residential aged care facilities.9
Some of this antibiotic use may be inappropriate. For instance, the 2017 ACNAPS found that more than half (55.2%) of antimicrobial prescriptions were for residents who had no documented signs or symptoms of infection in the week before the antimicrobial start date.9 An example of a possible driver of this use may be the treatment of asymptomatic bacteriuria, for which antibiotic therapy is not recommended.1
Further, a quarter (26.9%) of prescriptions had a start date that went back over six months. This suggests that regular review of the ongoing need for an antibiotic prescription and attempts to rationalise use should be considered. More research is needed to improve our understanding of antibiotic prescribing in residential aged care facilities.
Conclusion
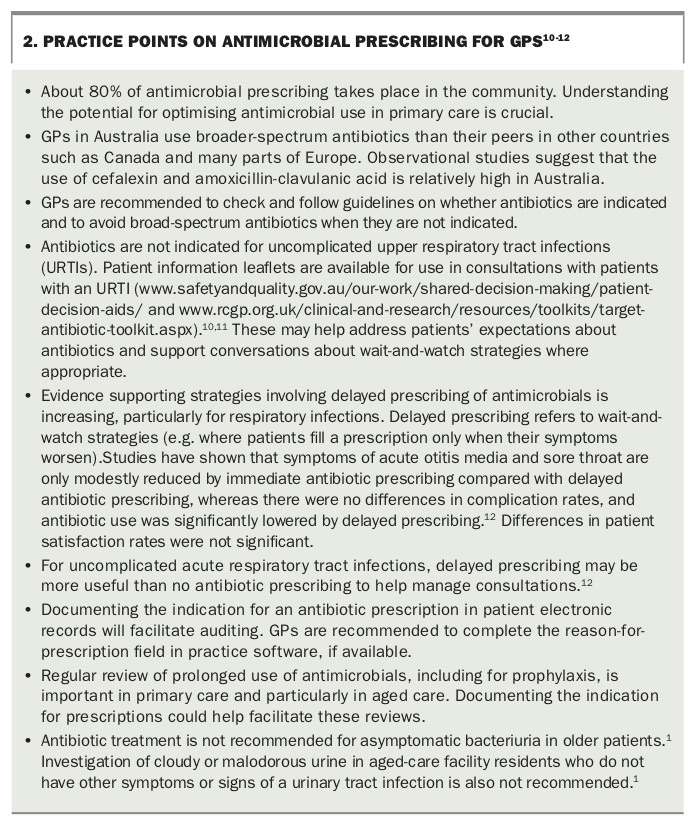
Available data on antibiotic prescribing in the community in Australia are limited but suggest that some antibiotic use is not concordant with guidelines. AMS activities could focus on high usage of broad-spectrum antibiotics and possible prescribing for conditions that do not usually require antibiotic treatment. Some practice points on antimicrobial prescribing for GPs are summarised in Box 2.10-12 Documentation of the indication for antibiotic prescriptions in practice software would facilitate better review of antibiotic prescribing. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.