Hip pain throughout the lifespan

Hip pain may arise from inflammation or injury of the many structures in and around the hip joint and may also be referred from distant spinal or intra-abdominal structures. The most common causes vary between age groups and by sex.
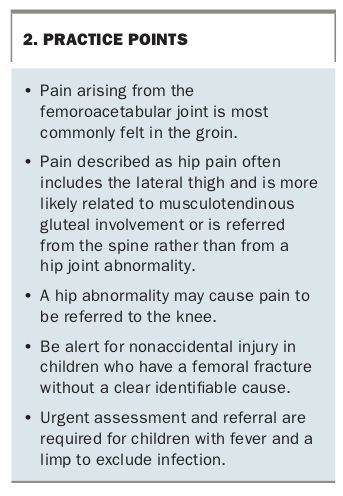
- Not all pain that the patient calls hip pain is coming from their hip; true hip joint pain is more commonly felt in the groin.
- The cause of hip pain can usually be identified based on a thorough history and physical examination.
- History taking should focus on the cardinal features of a patient’s pain, with special attention to the exact site, time course, associated features and functional profile.
- Systematic examination follows the basic process of look, feel, move.
- Choosing the appropriate imaging modality can help to rule diagnoses in or out, but inappropriate imaging may be misleading.
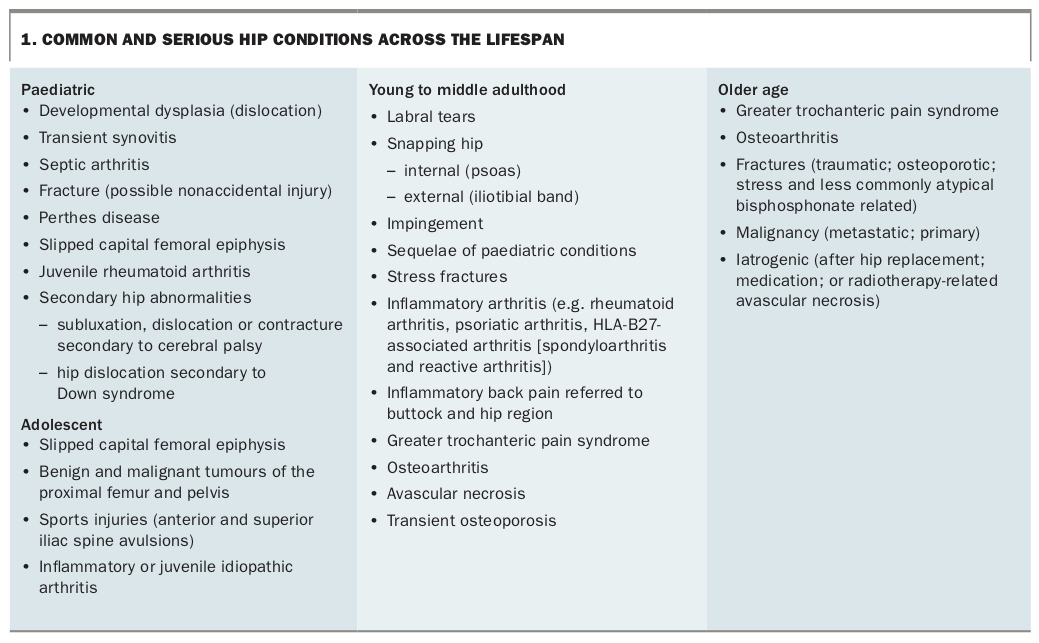
- Hip conditions are complex and vary greatly between the paediatric, adolescent, middle-aged and older-age populations.
- Be alert for a child with a limp and a fever as possible septic arthritis or osteomyelitis require urgent attention.
Hip conditions are complex and vary greatly between the paediatric, adolescent, middle-aged and older-age populations. Appropriate and timely management depends on accurate diagnosis, which requires a high index of suspicion and a broad knowledge of the many conditions that affect the hip throughout the lifespan.
It is important to take a detailed history of the pain site and aggravating actions as not all pain that the patient calls hip pain is coming from their hip. It may be referred from the spine or other structures. True hip joint pain is more commonly felt in the groin. Symptoms may include limp, clicking, instability, stiffness, weakness and pain that may be located in the groin, lateral hip, buttock, back or even the knee.
Examination can reveal many signs such as a short leg, loss of rotation, impingement and tenderness, and a positive Trendelenburg test result indicating impairment of hip abduction. Through performing a thorough assessment supported by appropriate investigations, GPs can identify a range of conditions, from common chronic conditions such as osteoarthritis (OA) of the hip through to septic arthritis in a young child, which is an acute emergency. This article provides a nonexhaustive review of common and serious hip conditions that occur across the lifespan, including a summary of typical signs, symptoms and management options.
Functional anatomy of the hip
The hip is a ball-and-socket synovial joint in which the rounded head of the femur articulates with the cup-shaped acetabulum, which has increased joint congruity due to the acetabular labrum. It is stabilised by a strong and dense fibrous capsule that is strengthened by three prominent reinforcements: the iliofemoral, pubofemoral and ischiofemoral ligaments.
The hip joint and its surrounding musculature help not only to propel the body forward but also to maintain the upright position of the trunk. The primary hip flexors are the iliopsoas, rectus femoris and sartorius muscles. The gluteus maximus and hamstring muscles (long head of biceps femoris, semimembranosus and semitendinosus) function as the primary hip extensors. Hip abduction is accomplished by the gluteus medius and gluteus minimus. The adductor group consists of the adductor longus, adductor magnus, adductor brevis, gracilis and pectineus muscles. The motion required for performing activities of daily living is flexion of at least 120°, abduction of 20° and rotation of 20°. However, sporting activities often necessitate a greater range of motion with studies suggesting that reduced total range of hip motion may predict the development of groin pain in athletes.1
Several prominent bursae around the hip joint facilitate the gliding of soft tissues over areas of friction. The largest and most important is the trochanteric bursa that is located between the iliotibial band and the insertion of gluteus medius onto the greater trochanter.
Hip pain may arise from inflammation or injury of the many structures in and around the hip joint and may also be referred from distant spinal or intra-abdominal structures. The most common causes vary between age groups and by sex and are discussed more fully below.
Clinical evaluation
Hip pain is commonly encountered in the primary care setting and the many diverse aetiologies are outlined in Box 1. The pain may be from local causes in the hip or referred from more proximal structures in the spine and pelvis (see Practice Points in Box 2). The cause can usually be identified based on a thorough history and physical examination. Imaging may be required if symptoms are not settling or a serious cause such as a fracture or tumour is suspected.
{kind=link}
{kind=link}
History
Taking a thorough history is the first step in assessing a patient who says they have hip pain. Questions should focus on the cardinal features of the pain, with special attention to the exact site, time course, associated features and functional profile.
Site
Pain that is mainly lateral and is causing inability to sleep on the affected side is likely to be indicative of trochanteric pain syndrome, whereas pain in the groin that is worse on mobilising and getting out of a chair is more likely to be due to an intra-articular abnormality such as OA. If the pain is mostly localised to the lateral thigh with associated numbness then cutaneous nerve entrapment (meralgia paraesthetica) may be likely, whereas buttock pain or pain radiating down the leg may suggest a lumbar spine abnormality.
It is important to recognise that pain from the hip can be referred to the knee. In some patients – most commonly in children – this may be the only reported site of pain. In such a patient, moving the knee does not cause pain but movement of the hip may reproduce the knee pain.
Time course
The time course of the pain is important in recognising serious conditions, such as occult fractures associated with a fall and ensuing groin pain. In a child, a fever with progressive difficulty in bearing weight is highly suggestive of infection. Pain that is worse at night may be suggestive of malignancy, whereas prolonged morning pain and stiffness may represent an inflammatory arthropathy.
Associated features
It is important to establish whether the patient has other features such as fevers, weight loss, other systemic conditions or neurological symptoms in the leg that are potentially associated with their pain. Involvement of other joints may provide clues to the primary disease affecting the hip; for example, metacarpophalangeal and proximal interphalangeal joint swelling or deformity may indicate rheumatoid arthritis, and distal interphalangeal joint involvement suggests OA.
Functional profile
Asking about exacerbating activities and forming a functional profile are essential to obtaining a complete patient history. Patients with hip pain may have particular difficulty with activities requiring hip flexion such as tending to their feet, doing up shoelaces, getting in and out of a car or standing from a seated position. With regard to chronic conditions, it is important to ask about walking distance and walking aids. In younger patients, it is important to ask about particular positions and movements that reproduce their pain, which may point toward impingement or a tendon abnormality as the diagnosis.
Family history and personal risk factors
When assessing hip pain in a child, it is important to ask about ‘clicky hips’ and whether they required a brace as a baby. Similarly, in adolescents and young adults, any history of childhood hip problems should be noted. If avascular necrosis (AVN) is suspected, risk factors such as corticosteroid use and alcohol abuse should be asked about. A family history of OA or inflammatory arthritis is relevant in assessing older patients.
Examination
A systematic examination of the hip can be done quickly. In many cases it can confirm the diagnosis that is suspected based on the patient’s history. Systematic examination follows the basic process of look, feel, move, as follows.
Look
With the patient standing, pelvic tilt, muscle wasting and scars are assessed and a Trendelenburg test is performed (remember: sound side sags). The patient then walks and the gait is observed for:
- antalgia – shortening of stance phase on one side to avoid pain
- a sideways lurch – patients with OA or abductor tears may sway their centre of gravity over the bad hip to reduce the load through the joint
- dropping shoulder – may suggest a leg-length discrepancy.
Feel
With the patient supine, the landmarks of the hip are palpated. Many of the bony landmarks and soft tissues around the hip are easily palpable, including the iliac crest, greater trochanter, ischial tuberosity, pubic symphysis, posterior superior iliac spine and anterior superior iliac spine. Exquisite lateral tenderness is found in trochanteric bursitis and abductor tears, whereas vague buttock tenderness may represent lumbar radiculopathy. A tender lump in the groin may reveal an abdominal hernia, whereas an intra-articular hip abnormality may not cause much tenderness at all, owing to the large soft tissue envelope of this deep joint.
Move
The range of motion of the hip is then tested. With the patient supine, a screening ‘log-roll’ of the leg on the bed is used to test for an irritable hip, which may be caused by severe intra-articular abnormalities such as infection, fracture, AVN or severe OA. Adduction and abduction are also assessed with the patient in the supine position, and the Thomas test may be performed to check for fixed flexion contracture. The hip is then flexed to 90° and internal and external rotation are assessed. It is crucial to assess both sides and document the range as accurately as possible. If rotation of the hip is significantly reduced and painful on one side, it is highly likely there is an intra-articular abnormality of the hip. Impingement may be confirmed with the FADIR test (pain in flexion, adduction, internal rotation).
Finally, a neurovascular screening examination is performed. For completeness the joint above (lumbar spine) and below (knee) the hip may also be examined if the diagnosis is unclear.
Radiographic evaluation
Imaging for hip disorders includes plain x-ray, ultrasound, MRI and, in rare circumstances, nuclear medicine scans. Choosing the appropriate modality can help to rule diagnoses in or out, but inappropriate imaging may be misleading.
OA is the most common cause of hip pain and can often be diagnosed clinically with pain reproduced on movement of the hip joint and reduced range of motion particularly on internal and external rotation. If the patient’s pain is not settling with simple measures, surgery is being considered or a more serious condition is suspected, a plain x-ray is indicated. If plain x-rays show OA then an MRI is of no further benefit. However, if plain x-rays are normal and a local hip abnormality is strongly suspected, an MRI can be useful for a broad spectrum of conditions including early OA, abductor tendon tears, stress fractures, AVN, labral tears, synovitis and tumours.
Ultrasound, although user-dependent, can be useful for finding clues to extra-articular causes of pain, including trochanteric bursitis, abductor tears, psoas tendinitis and snapping hip, and can also help determine whether there is an effusion. When combined with a corticosteroid injection or aspirate, ultrasound can play a therapeutic role.
CT scanning remains superior to MRI for imaging bony architecture and complex fractures. Although bone scans will show osseous conditions such as metastatic disease, Paget’s disease and occult femoral neck fractures, MRI will usually be more informative.
Common paediatric hip conditions
Developmental dysplasia and dislocation of the hip
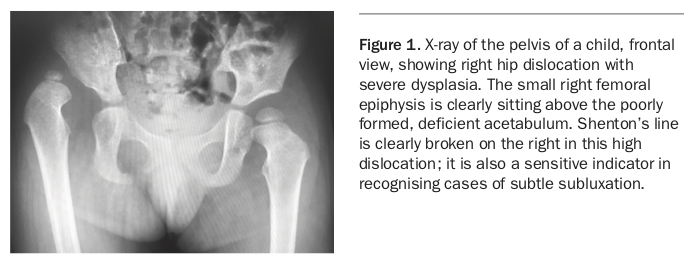
Developmental dysplasia of the hip encompasses a clinical spectrum ranging from mild early subluxation to irreducible teratological dislocation of the hip (Figure 1). It is more common in the left hip, and risk factors include family history, breech positioning, oligohydramnios, female sex and being first born.
{kind=link}
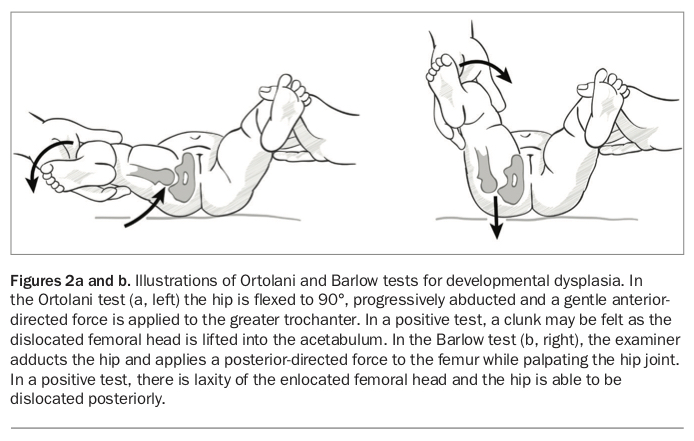
Clinically, developmental dysplasia may be suspected by the observation of asymmetric skin creases, reduced abduction of the affected hip and positive special tests (Barlow and Ortolani tests; Figure 2). Before six months of age, the femoral head has not ossified and ultrasound is the imaging modality of choice. After six months, progress may be monitored using pelvic x-rays and looking for symmetrical development of the acetabulum and femoral head.
{kind=link}
Management depends on severity and chronicity, ranging from observation to bracing in a Pavlik harness, surgical reduction and corrective osteotomies. Persistent dysplasia may lead to early hip joint degeneration and is one of the most common reasons for total hip replacement in young adults. Clinicians should have a high index of suspicion as clinical examination may not always be reliable. If in doubt, an ultrasound or x-ray is recommended.
Transient synovitis, septic arthritis and osteomyelitis
Children with transient synovitis, septic arthritis or osteomyelitis may present similarly, with a limp and a painful, irritable hip. Typically, there is an insidious onset of limp and progressive reluctance to bear weight. Prodromal viral illness may be associated with transient synovitis, but this is debatable.
Clinicians should have a high index of suspicion for infection and consider it a medical emergency. On clinical examination, a child with septic arthritis typically appears unwell, may have a fever, has an extremely irritable hip that is often held in a fixed position of slight flexion and external rotation and refuses to bear weight. A child who presents with transient synovitis, on the other hand, limps and has a hip that is irritable in end-range rotation but is comparatively happy.
In osteomyelitis of the proximal femoral metaphysis or pelvis, hip range of motion is often preserved, although there may be tenderness and pain on bearing weight. In assessing a limping child with a suspected hip abnormality, the threshold for performing a white blood cell count and blood culture and measuring C-reactive protein level should be low as untreated septic arthritis of the hip can cause cartilage destruction leading to permanent disability. The Kocher criteria are useful for distinguishing between transient synovitis and septic arthritis of the hip. The criteria include:
- fever of more than 38.5°C
- refusal to bear weight
- erythrocyte sedimentation rate of more than 40 mm/hour
- serum white blood cell count of more than 12,000 cells/mcL.
When four criteria are present, the probability of septic arthritis may be as high as 99.6%.2
Slipped capital (upper) femoral epiphysis
Slipped capital (upper) femoral epiphysis (SCFE) occurs when a relative weakness of the growth plate causes the femoral shaft to slip anteriorly and superiorly, leaving the epiphysis (femoral head) behind in the acetabulum. Classically, SCFE occurs in overweight adolescent males (male to female ratio, 2 to 1) who present with a limp and vague groin, thigh or knee pain that has been present for weeks to months. There may have been an acute injury, but onset is often insidious. It is more common in Pacific Islander, Maori, Indigenous Australian and black African populations and is usually idiopathic; however, the condition may also occur secondary to endocrinopathies such as hypothyroidism, hypo or hyperparathyroidism, renal osteodystrophy and hypopituitarism. The incidence may be rising in association with childhood and adolescent obesity.3
Examination of a patient with SCFE reveals an antalgic gait and obligatory external rotation as the hip is flexed with the patient in the supine position. In unstable femoral epiphysis slips, the patient may be unable to bear weight. Most slips can be identified on anteroposterior pelvis and frog-leg lateral radiographs, although undisplaced slips may only be visible on MRI as a widened physis with adjacent bony oedema.
SCFE is a serious condition that requires a high index of suspicion, diagnostic imaging confirmation and urgent referral to a paediatric orthopaedic surgeon. Once the diagnosis is confirmed, the child should be prevented from bearing weight and immediately referred for urgent (same day) orthopaedic review.
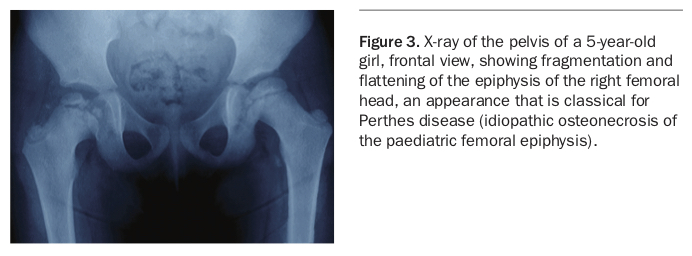
Perthes disease
Perthes disease is an uncommon idiopathic condition characterised by AVN of the femoral head. It typically occurs in males (male to female ratio, 5 to 1) from the ages of 4 to 8 years but may present outside these ages. As for patients with SCFE, patients with Perthes disease may report weeks to months of limp and pain that localises to the groin or even the knee. Unlike patients with SCFE, patients with Perthes disease tend to be small, and it is more commonly seen in Asian, Eskimo and European populations.
On clinical examination, children with Perthes disease may have a limp, with reduced abduction and internal rotation of the affected hip. Investigations include anteroposterior and frog-leg lateral hip x-rays, which may show sclerosis, fragmentation or a remodelling, misshapen femoral epiphysis, depending on the stage of the disease (Figure 3). Initial management after diagnosis if the patient is in the early stages of disease includes avoidance of playing sport and bearing weight, with early referral to an orthopaedic surgeon. Observation or surgery may be indicated.
{kind=link}
Fractures and nonaccidental injury
Fractures of the femoral shaft can occur at any age and radiological features cannot distinguish between accidental and nonaccidental fractures. Spiral fractures are not specific for child abuse; however, this possibility should be considered, particularly in younger and nonmobile infants.4
Common hip conditions of young to middle adulthood
Stress fracture
Stress fracture of the femoral neck can occur because of repetitive microtrauma from activities such as jogging. It occurs especially in underweight women with an associated low bone density. Patients typically present with groin pain that is exacerbated by bearing weight and relieved by rest.
X-rays may reveal sclerosis of the femoral neck or even a cortical lucency. Plain x-rays may be normal and the diagnosis decided on the basis of MRI or bone scanning. Stress fractures on the tension side of the femoral neck (the superolateral side) are much more likely to become complete displaced fractures and so are generally managed with prophylactic fixation, whereas those on the inferomedial (compression) side of the neck may be managed with restricted weightbearing and activity modification.
Impingement/labral tears
Femoroacetabular impingement (FAI) may be a cause of hip or groin pain in young active people. It occurs due to abutment of the femoral neck against the bony rim of the acetabulum, either due to overgrowth of the rim (pincer deformity) or loss of the normal concavity of the neck (cam deformity). Pain from FAI is exacerbated by activities involving hip flexion.
FAI may be associated with labral tears, chondral flaps or early degenerative arthritis of the hip. On physical examination, groin pain is reproduced by the FADIR (flexion, adduction, internal rotation) manoeuvre and there is restricted internal rotation in flexion. Plain x-rays show many findings of FAI such as a typical ‘pistol grip’ deformity (lack of a normal concavity to the femoral waist), coxa vara, an aspherical femoral head or a femoral head-neck junction cyst, and should be the first line of investigation. MRI can then be used to assess for labral tears, chondral flaps and focal articular cartilage loss. Initial treatment is nonoperative; however, hip arthroscopy may benefit appropriate patients with persistent pain.
Greater trochanteric pain syndrome
Lateral hip pain is a common complaint and can be due to multiple causes other than trochanteric bursitis, hence the more comprehensive term greater trochanteric pain syndrome. Causes include inflammation of the subgluteus maximus bursa (trochanteric bursa), tendinopathy or tears of the gluteus medius and minimus tendons and external snapping hip. Gluteal tendinopathy is often present with trochanteric bursitis and is more common in overweight women aged 40 to 60 years, probably owing to the biomechanics of the female pelvis. Patients often have quite debilitating pain on weightbearing, a limp and an inability to sleep on the affected side at night.
In 90% of cases, patients with greater trochanteric pain syndrome will either improve without intervention or only require short-term use of anti-inflammatories, education regarding normal gait preservation and instruction on gluteal strengthening exercises. Stretching may aggravate the condition if gluteal tendinopathy is present and the key focus of exercise should be on gradual progression of tendon loading. Weight loss and education regarding tendon care complement the physical therapy. Corticosteroid injections are no more effective than the above approach but are still often used for short-term relief ; however, they should only be considered as an adjunct to exercises. In the younger patient suspected abductor tears may be amenable to surgical repair.
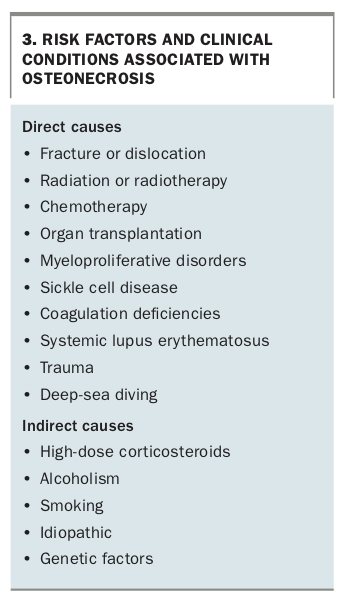
Osteonecrosis of the hip
Osteonecrosis of the hip, also referred to as AVN of the femoral head, presents as rapidly progressive acute groin pain, often in a younger population than would typically suffer from OA. The clinical features are similar to those of OA and include activity-related groin pain, night pain and difficulty reaching their feet and getting in and out of cars. Patients may also notice that the affected leg has become shorter. This is due to collapse of the femoral head.
AVN should be suspected in patients with known risk factors including, for example, high-dose corticosteroid use, alcoholism, sickle cell disease, deep-sea diving and trauma (Box 3). A plain x-ray may be normal in the very early stages of the disease, but MRI detects the earliest bone marrow oedema. X-rays of more advanced disease may show sclerosis or subchondral or advanced collapse of the femoral head. Treatment depends on stage and, although currently no therapies have been proven to halt the progression of the femoral head collapse, interventions may include bisphosphonates, restricted weightbearing, surgical core decompression, rotational osteotomies or hip replacement.
{kind=link}
Osteoarthritis in older age
Hip OA is most common in patients over the age of 50 years. The causes can be divided into primary or secondary (after disease or malalignment of the hip joint). An intrinsic disorder of articular cartilage can result in primary OA. Common causes of secondary OA include childhood hip disorders, trauma and previous inflammatory arthritis.
The characteristic symptom of OA is an insidious onset of pain in the groin, as opposed to the lateral hip in trochanteric bursitis, which is exacerbated by activity and relieved with rest. Patients with more advanced OA can also experience pain at rest and at night and radiation of pain to the knee along with subsequent loss of functional ability. Other key features include pain and restriction on internal rotation, short-lived early morning stiffness (less than 30 minutes) and limitation of flexion.
Gait is almost always affected and patients have either an antalgic gait (a swinging type of gait and a lurching of the trunk if the hip is stiff) or a Trendelenburg gait if any weakness of the abductor muscles is present. There is often poor correlation between the degree of pain and the radiological changes present.
In addition to simple analgesia, the patient should be advised to undertake nonweightbearing exercise such as hydrotherapy or riding an exercise bike. There is no evidence for benefit of stronger analgesics such as pregabalin or opioids and these are best avoided for long-term pain relief in hip OA. Weight loss has been shown to reduce pain. Consultation with physiotherapists and occupational therapists to increase the range of hip movement and to provide aids and supports around the house may also be beneficial. Swimming and aqua therapy can enable range-of-motion activities without the stress of bearing weight. Walking with a cane or stick in the opposite hand can also reduce the load and pain experienced through the affected hip joint. Physiotherapy review may be required to educate the patient about the appropriate gait with a cane.
Hip OA tends to progress more rapidly than knee OA and patients should be referred in a timely manner for consideration for total hip joint replacement or arthroplasty if the conservative measures are inadequately controlling the pain or improving function. Most people undergoing total hip replacement have very successful short- and long-term outcomes.
Inflammatory arthritis throughout the lifespan
Inflammatory arthritis comprises a broad range of autoimmune conditions that can occur throughout the lifespan. Juvenile idiopathic arthritis affects children under 16 years and may be oligoarticular, polyarticular or systemic. It is characterised by pain, swelling and stiffness with or without fever, rashes and uveitis. In patients with suspected arthritis accompanied by scaly skin rash and nail changes, psoriatic arthritis may be the diagnosis. The hip capsule is tight and even a small amount of additional synovial fluid associated with synovitis can be associated with quite significant pain and irritability on movement of the hip joint.
Ankylosing spondylitis causes spinal pain and stiffness most often involving the joints of the axial skeleton: the neck, back and pelvis. Symptoms usually commence between the ages of 15 and 45 years. In established ankylosing spondylitis the hip is the most common nonaxial joint to be involved and in the younger adolescent may be the first presenting feature of the condition, which then evolves. Pain from the sacroiliac joints can be commonly referred to the buttock and lateral thigh region and mistaken for hip pain. Inflammation of muscle and ligament attachments (enthesopathy) is the hallmark of ankylosing spondylitis and may manifest as adductor enthesopathy, osteitis pubis, achilles tendonitis or even plantar fasciitis.
Inflammatory bowel disease may present as isolated hip pain without more widespread arthritis as you would expect with rheumatoid arthritis. Rheumatoid arthritis is another autoimmune condition that typically affects the small joints of the hands and feet but may affect any joint in the body. It would be unusual for rheumatoid arthritis to begin in the hips, but it should be considered in patients presenting with hip pain. Synovitis of the affected joints causes swelling, tenderness and prolonged early morning stiffness that is often symmetrical in distribution.
Conclusion
Patients of all ages with hip pain commonly present to their GP. Hip conditions are varied and complex, yet the cause of hip pain can usually be identified based on a thorough history and physical examination of the patient. If imaging is required, a careful choice of the modality used can help to rule in or rule out a diagnosis. GPs therefore are central to recognising and managing common and serious hip abnormalities, including the acute emergency of septic arthritis in a young child. MT