Part 1. Finding your patients with hepatitis C


Direct-acting antivirals (DAAs) can now cure almost all patients with chronic hepatitis C. This gives us the opportunity to eliminate hepatitis C from Australia. However, the number of people receiving DAA therapy is declining despite an estimated 165,000 people living with chronic hepatitis C. GPs have a key role in identifying and treating their patients living with hepatitis C if we are to reduce disease burden and achieve hepatitis C elimination.
- Direct-acting antivirals (DAAs) can cure over 95% of people with hepatitis C with only eight or 12 weeks of treatment.
- Curing patients of hepatitis C not only reduces disease burden for the individuals but can contribute to the elimination of hepatitis C in Australia.
- GPs, nurse practitioners and specialists can all prescribe DAA therapy.
- Of the estimated 165,000 people in Australia with chronic hepatitis C, about 20% are undiagnosed, and among those diagnosed more than half have not been treated.
- GPs have a crucial role in identifying their patients living with hepatitis C through sensitively raising the topic of HCV infection and offering testing and treatment.
New curative treatments for hepatitis C, known as direct-acting antivirals (DAAs), have revolutionised the management of people living with hepatitis C virus (HCV) infection. The simplicity and tolerability of DAAs means it is now easy to cure hepatitis C in most patients, making possible the elimination of hepatitis C in Australia. However, major challenges remain in finding people with hepatitis C who have not been diagnosed, linking people who have been previously diagnosed into care, and supporting patients to complete treatment. GPs have a crucial role in identifying and treating their patients with hepatitis C to help achieve the goal of eliminating hepatitis C in Australia by 2030.
This article is the first in a series about eliminating hepatitis C in Australia. The series will guide GPs through testing, treating and curing hepatitis C in primary care. This article focuses on who to test and how to test.
Hepatitis C virus infection
HCV is a bloodborne virus that can cause liver inflammation and liver scarring and puts people at risk of cirrhosis, liver failure and hepatocellular carcinoma (HCC). There are six main genotypes of HCV; the most common in Australia are genotype 1 and genotype 3.1
The natural history of HCV infection is summarised in Figure 1.2 Following acute HCV infection, 15 to 25% of people will spontaneously clear the infection, with the other 75 to 85% progressing to chronic infection. About 20 to 30% of people with chronic HCV infection develop cirrhosis after 20 to 30 years of infection.3 Hepatitis C is the most common cause of HCC in Australia. HCC is the fifth most common cause of cancer death among males and the eighth most common cause of cancer death among females in Australia.4 Incidence rates of HCC have increased more than those of any other cancer except thyroid cancer in Australia.4
What are the signs and symptoms of chronic hepatitis C?
Chronic HCV infection is usually asymptomatic. If symptoms are present, they are usually nonspecific, such as tiredness and lethargy. Serious symptoms occur when advanced liver disease develops, including confusion, jaundice, ascites, peripheral oedema, easy bruising and bleeding, haematemesis and muscle wasting.
Investigation results such as raised alanine aminotransferase (ALT) or aspartate aminotransferase (AST) levels can indicate liver inflammation and warrant further investigation, including testing for viral hepatitis.
What are the benefits of cure?
Curing hepatitis C reduces the risk of cirrhosis and HCC. During 2016-17, there was an estimated 20% decline in deaths from hepatitis C-related liver failure and HCC in Australia due to the rapid increase in number of people cured of HCV infection.5
Recent evidence suggests that people who achieve a sustained virological response or hepatitis C cure (defined as no detectable HCV RNA on a blood test 12 weeks after treatment completion) report improved quality of life. This includes physical health benefits, notably less fatigue, and an improved sense of psychological wellbeing related to less uncertainty about future health and no longer fearing infecting others.6
Australia’s progress towards eliminating hepatitis C is shown in Box 1.7-10
How many people are living with hepatitis C?
Globally, an estimated 71.1 million people are living with chronic hepatitis C.11 More than 70,000 people with hepatitis C in Australia have been treated and cured since DAAs became available in this country.12 However, over 165,000 people in Australia are still living with hepatitis C (projections based on a published model and updates MBS and PBS data).9
The hepatitis C cascade of care describes the recommended pathway through clinical care for people at risk of hepatitis C. Numbers of people at each stage of the cascade of care in Australia in 2017 are shown in Figure 2.13 An estimated 80% of people living with hepatitis C had a positive HCV antibody result (145,838), but only 47% of those people (68,544) had a positive HCV RNA PCR result confirming chronic HCV infection (not shown). Of these, 31% (21,530) received hepatitis C DAA treatment in 2017, with 95% achieving cure.13
It is worth noting that although an estimated 80% of people infected with hepatitis C in Australia have been diagnosed HCV antibody-positive, this refers to ‘lifetime diagnosed’. Many people with chronic hepatitis C are not currently linked to health services for their hepatitis C and are missing out on treatment and cure. This is a key driver of the drop-off in the cascade from diagnosis to treatment. GPs can help reverse this drop-off through identifying patients who have been previously diagnosed with hepatitis C and supporting them into treatment.
Who should be tested for hepatitis C?
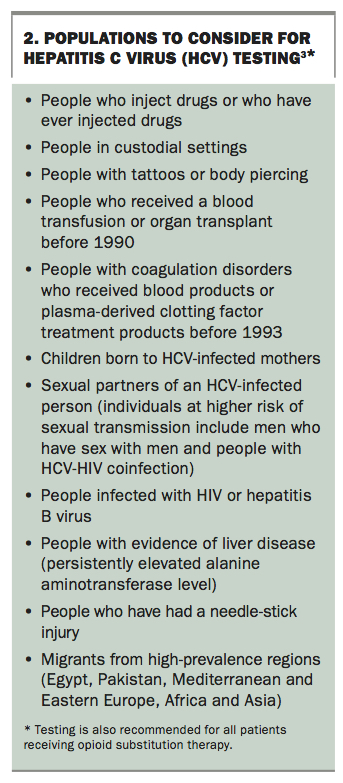
HCV is spread through blood to blood contact, where the blood of one person enters the bloodstream of another. Key risk factors and populations to consider for HCV testing in Australia are shown in Box 2.3 Sometimes these risk factors may be difficult to identify during busy GP consultations, and they may have occurred in the distant past for many patients.
{kind=link}
People who have ever injected drugs (recently or at some time in their life) are at risk of having hepatitis C because of the risk of acquiring HCV through sharing injecting equipment. With an estimated incidence of 5.4 per 100 person years among people who inject drugs, it is particularly important to test and treat people who currently inject drugs to reduce onward transmission of hepatitis C and prevent reinfections.13
In 2017, a total of 10,537 hepatitis C notifications were made in Australia.13 Of the notified patients, 11% were Aboriginal or Torres Strait Islander people, 69% were male and more than half were aged 40 years and over. When classified by age, 11% of notified patients were under 25 years, 12% were between 25 and 29 years, 26% were between 30 and 39 years and 51% were 40 years and over.
The National HCV Testing Policy provides detailed information on who to test (http://testingportal.ashm.org.au/hcv). Apart from identifying risk factors for infection, an incidental finding suggestive of advanced liver disease or abnormal liver function test results warrant further investigation, including testing for viral hepatitis. GPs working in high-prevalence practices, such as in homeless health or opioid substitution therapy, might consider offering testing to all patients.
Tips on starting the conversation about testing
GPs may find it challenging to ask patients about current or past risk practices related to hepatitis C. Most doctors take a social history from new patients, and this is an opportunity to enquire sensitively about risk factors for hepatitis C, such as current or past drug use, along with recording demographic variables such as country of birth and sexual behaviour. This information is also crucial for establishing whether there is a need to test for other bloodborne viruses, such as hepatitis B virus and HIV, which can all be undertaken as part of a ‘new patient screen’.
Existing patients also need to be tested for hepatitis C. There are many opportunities for testing as part of general health checks, sexual health screens, pre-travel check-ups and antenatal screening and as part of health promotion campaigns.
Starting a conversation with a patient about hepatitis C is sometimes difficult, as discussing past or current drug use can be uncomfortable for both the patient and the GP. Patients may be unlikely to disclose a history of injecting drug use, even to GPs with whom they have a good relationship.
Having a focus on ‘liver health’ or ‘new hepatitis C treatments’ in the clinic as part of a targeted health promotion campaign can be a strategy to initiate a conversation about hepatitis C and to introduce testing to people who might be at risk. For example, a GP could explain ‘Now that we have new effective treatments for hepatitis C that are available on the PBS, we want to make sure we offer this treatment to all our patients who are eligible. Would you be interested in knowing about the ways people get hepatitis C and seeing if you think you should get tested?’
Most people living with hepatitis C will have been previously diagnosed. This includes:
- individuals who are fully diagnosed or partly diagnosed (HCV antibody test but no HCV RNA PCR test)
- people who have previously been treated with older medications with treatment failure or who have been reinfected.
This group also includes people who have not previously been offered treatment, those who declined treatment and those who are not engaged with regular care. Many people living with hepatitis C have experienced stigma and discrimination related to their HCV infection or history of drug use. They may have had negative experiences when accessing health care in the past or have limited contact with the healthcare system. This is an important group to engage and to support into treatment.
Trying to engage this group into treatment can be difficult. Offering testing in the context of a discussion about the new treatments may be a good way to re-engage this group.
When discussing the new treatment options, GPs should cover the following:
- new treatments cure more than 95% of people with hepatitis C who complete the prescribed treatment course
- treatment lasts only eight or 12 weeks
- all treatments are oral (no injections)
- side effects, if any, are mild, such as fatigue, nausea and headaches; these generally subside after the first four weeks.
GPs can identify patients with hepatitis C or requiring testing by searching their practice management system. Third-party tools such as POLAR or Pencat can help identify patients with potential risk factors and indicators (e.g. abnormal liver function test results) or known hepatitis C by conducting a practice audit. Training and support may be available through your local Primary Health Network.
Points to discuss with patients before testing are shown in Box 3. Informed consent to testing is required and it is important to ensure your patient understands the next steps. Positive results need to be conveyed in a sensitive manner.
What tests are needed?
Two tests are required to diagnose HCV infection:
- an antibody test to screen for HCV antibodies (indicating past exposure to HCV)
- a polymerase chain reaction (PCR) test for the presence of HCV RNA (indicating current HCV infection).
To reduce the number of appointments, blood draws and time to diagnosis, we recommend reflexive hepatitis C testing. Both the HCV antibody test and the PCR test for HCV RNA can be ordered on the same pathology order form by writing ‘Please order hepatitis C PCR only if HCV antibody is detected’ or ‘HCV antibody +/- HCV RNA, if Ab positive’. The Medicare Benefits Schedule covers an HCV RNA PCR test only in the case of a positive HCV antibody result, and therefore it is recommended to add one of the above phrases in the clinical notes of the pathology request form to avoid an out-of-pocket cost for the patient.
A comprehensive bloodborne virus screen, including testing for hepatitis B and HIV infection, is also recommended for patients at risk of hepatitis C. This is because of the shared risk factors across all three infections and the availability of highly effective treatments for both hepatitis B and HIV infection.
Interpretation of HCV test results is shown in Figure 3. Documented chronic hepatitis C (duration of current HCV infection six months or longer) is a PBS eligibility criterion for accessing treatment. Test results in acute hepatitis C are discussed in Box 4.
If HCV RNA is not detected after a positive HCV antibody result then the patient has either spontaneously cleared HCV or been successfully treated in the past. HCV antibodies will most likely remain; however, HCV antibodies do not provide immunity to future infection, and there is currently no effective vaccine to prevent hepatitis C.
Hepatitis C is a notifiable condition (HCV antibody positive and/or RNA positive) by the laboratory or medical practitioner, depending on the jurisdiction. If results indicate current HCV infection, patients should consider recommending to their sexual or injecting partners to be tested also.
The diagnosis of hepatitis C can be distressing for patients. The support of a knowledgeable, caring GP is crucial. Patient support organisations such as Hepatitis Australia can be helpful in providing support by phone or in person. Useful resources on hepatitis C for GPs and patients are shown in the Box on the inside back cover.
Conclusion
An estimated 165,000 people are living with chronic HCV infection in Australia; however, the number of people being treated is declining. Renewed efforts are needed to reach everyone living with hepatitis C and ensure they are linked to testing and treatment. GPs are well placed to identify people at risk of hepatitis C and to offer testing and DAA therapy. Curing a patient with chronic hepatitis C is easier than ever before. It has the potential not only to benefit the individual by reducing their risk of liver disease and HCC and by preventing transmission but can also contribute to the elimination of hepatitis C in Australia. MT
Dr Doyle receives funding for investigator-initiated research or consulting from AbbVie, Bristol-Myers Squibb, Gilead and MSD.
Dr Baker has received clinical trial funding and conference sponsorship and serves on the advisory board for AbbVie, Gilead and MSD.
Professor Stoové has an NHMRC Senior Research Fellowship and has received funding for investigator-initiated research from AbbVie, Bristol-Myers Squibb and Gilead.
Dr Pedrana receives funding for investigator-initiated research from AbbVie, Gilead and MSD.
Acknowledgement
The authors gratefully acknowledge the contribution to this work of the Victorian Operational Infrastructure Support Program received by the Burnet Institute.