An approach to thyroid dysfunction

Thyroid diseases
Thyroid dysfunction is common and can range in severity from asymptomatic to life-threatening. It is important for health practitioners to understand the blood tests and imaging required to determine the cause of thyroid dysfunction.
- The initial screening test for thyroid dysfunction is measurement of thyroid stimulating hormone (TSH) level, followed by measurement of free thyroxine (T4) and free tri-iodothyronine (T3) if the TSH level is abnormal.
- TSH receptor antibodies should be measured in all patients with hyperthyroidism to assess for Graves’ disease; antithyroid peroxidase antibodies and antithyroglobulin antibodies are associated with autoimmune (Hashimoto’s) thyroiditis but not specific.
- A technetium-99m thyroid isotope scan is useful to clarify the cause of hyperthyroidism if this is unclear, and thyroid ultrasound examination is useful to assess thyroid structure if there are abnormalities on clinical examination.
- Subclinical thyroid dysfunction does not always warrant treatment and clinicians should be familiar with the current indications for therapy.
- Thyroid dysfunction during pregnancy requires special care, and specialist referral is appropriate.
Thyroid dysfunction is common in the general population and may affect many body systems, owing to the role of thyroid hormones in regulating growth and metabolism. Consequently, presenting signs and symptoms vary, and a thorough history and examination are needed. This article provides a case-based review of common disorders causing hyperthyroidism and hypothyroidism that may be encountered by GPs.
How common is thyroid dysfunction?
The prevalence of thyroid dysfunction varies around the world according to rates of iodine deficiency. In iodine-replete areas, where the most common cause of thyroid dysfunction is autoimmune thyroid disease, the prevalence is 0.5 to 2% for hyperthyroidism and about 1 to 5% for hypothyroidism.1,2 The prevalence of thyroid dysfunction increases with age and is higher among women, such that 10 to 15% of older women are affected by thyroid disease.3
Significance of thyroid autoantibodies
Thyroid autoantibodies may be assessed to aid in diagnosis in patients with abnormal thyroid function results. They include:
- thyroid stimulating hormone (TSH) receptor antibodies (TRAb)
- antithyroid peroxidase (anti-TPO) antibodies
- antithyroglobulin antibodies.
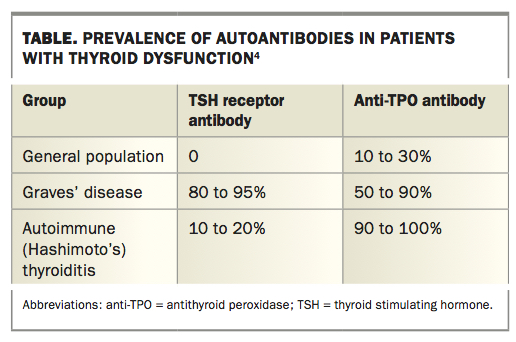
The interpretation of positive autoantibody results should take into account the sensitivity and specificity of the different tests (Table).4 Thyroid autoantibodies may be found in up to 15% of the population and may occur in the absence of thyroid dysfunction. In this setting, they are not clinically significant. Consequently, thyroid autoantibodies should not be assessed without a clear clinical indication, and the results should not be interpreted in isolation. Antithyroglobulin antibodies are no longer commonly used in the evaluation of patients with thyroid illness except in the follow up of thyroid cancer because of their lack of specificity.
{kind=link}
Hyperthyroidism
When should hyperthyroidism be suspected?
Hyperthyroidism should be considered in any patient presenting with symptoms or signs of anxiety or increased metabolism, including palpitations, diaphoresis, weight loss, amenorrhoea, tremor or atrial fibrillation, and especially in those with proptosis or goitre. Fatigue is a common symptom in patients with either hyperthyroidism or hypothyroidism.
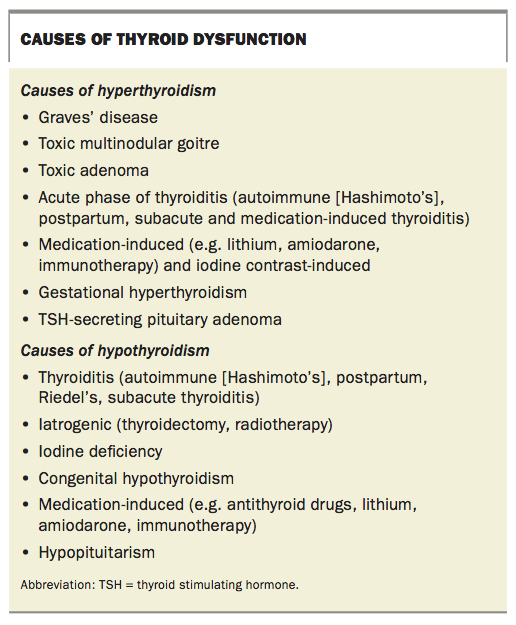
Common causes of hyperthyroidism are shown in the Box. Graves’ disease is the most common cause of hyperthyroidism.
{kind=link}
What blood tests should be ordered?
The initial screening test for thyroid dysfunction is measurement of serum TSH level. If this is in the normal range then thyroid dysfunction is unlikely. If the TSH level is low then subclinical or overt hyperthyroidism should be suspected, and measurement of free thyroxine (T4) and free tri-iodothyronine (T3) levels is important. In patients who are unwell for other reasons, sick euthyroid states can cause a low TSH level with generally low-normal T3 and T4 levels, and are a common differential diagnosis of subclinical hyperthyroidism.
An initial TRAb measurement is worthwhile in all patients with a TSH level below 0.1 mIU/L. A positive TRAb result has good specificity for Graves’ disease (Table). TRAb usually becomes negative when remission occurs. TRAb titres can be monitored to give an indication of Graves’ disease activity, as guided by a specialist.
Anti-TPO antibody (also known as antimicrosomal antibody) and antithyroglobulin antibodies can be assessed but are nonspecific. These antibodies are seen in many patients with Hashimoto’s, postpartum or subacute thyroiditis and in those with Graves’ disease. Titres of these antibodies do not reflect disease activity and thus serial monitoring is not needed if positive.
What other investigations might be useful?
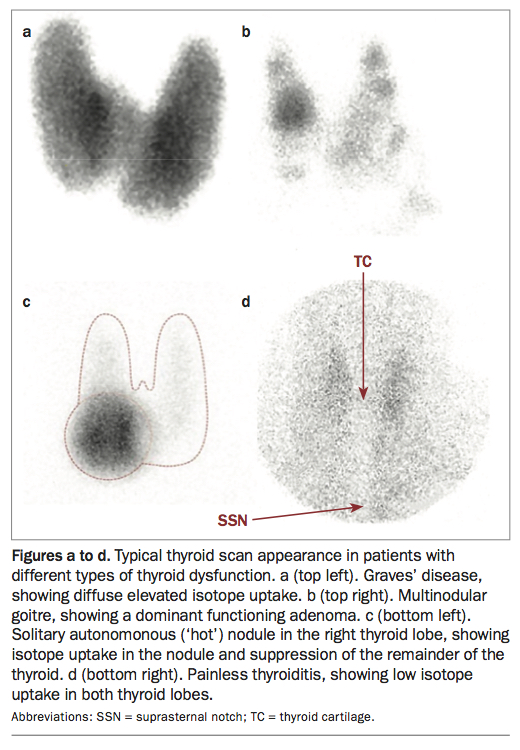
A technetium-99m (Tc-99m) thyroid isotope scan involves administering radioactive tracer that is taken up by functioning thyroid tissue. A Tc-99m thyroid scan assesses function and can be used to distinguish potential causes of hyperthyroidism when the diagnosis is not clear from clinical assessment and blood test results (Figures a to c). Tc-99m uptake is typically low in subacute thyroiditis (Figure d).
{kind=link}
A thyroid ultrasound scan can delineate any structural changes in the thyroid detected on examination, such as nodularity. However, an ultrasound scan is not routinely required in the workup of patients with thyroid dysfunction.
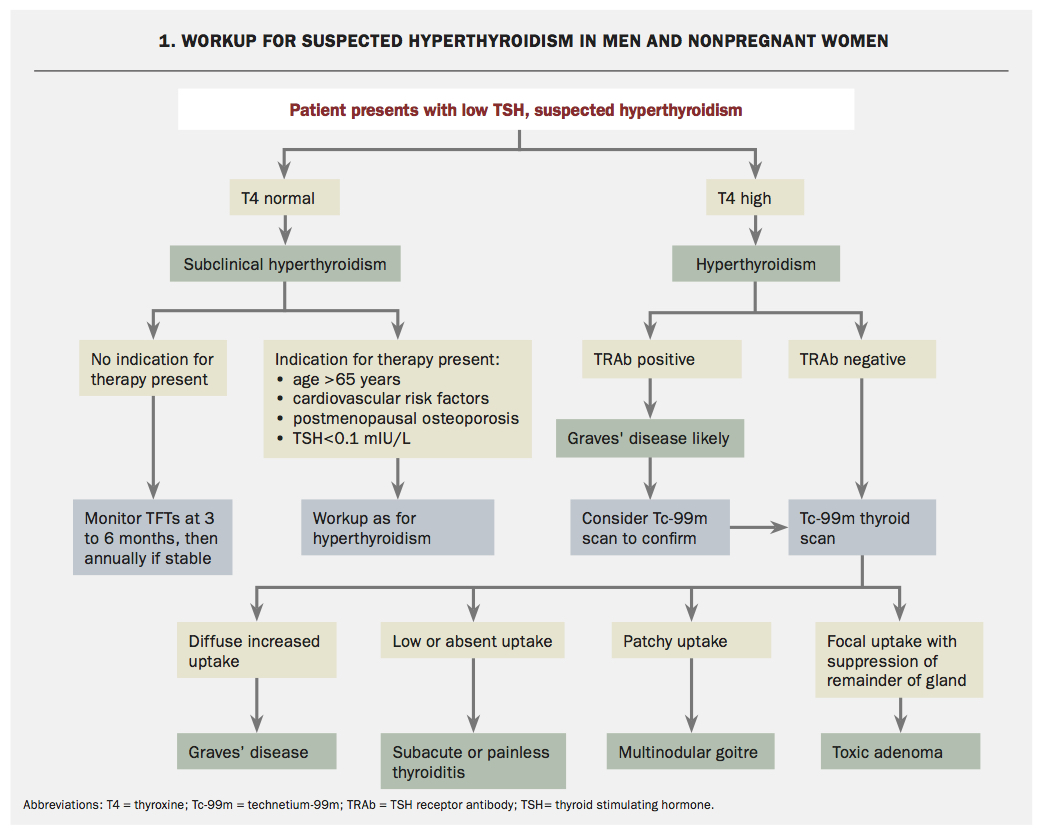
A general approach to the workup of patients with suspected hyperthyroidism is shown in Flowchart 1. Establishing the cause of hyperthyroidism is a crucial initial step, as illustrated in the following case scenarios.
Case 1. A young woman with thyrotoxicosis
A 29-year-old woman presents to hospital with a six-month history of panic attacks, weight loss and loose stools. Clinically, she has thyrotoxicosis, with a pulse rate of 100 beats per minute, a fine tremor, warm periphery and moderate diffuse goitre. There is no evidence of ophthalmopathy. Blood tests reveal the following levels: TSH less than 0.005 mIU/L (reference range [RR], 0.4 to 3.6 mIU/L), free T3 46 pmol/L (RR, 3 to 6 pmol/L) and free T4 70 pmol/L (RR, 10 to 20 pmol/L).
What other investigations should be ordered?
The patient’s TRAb level should be measured to confirm the presence of Graves’ disease. If she is positive for TRAb then no imaging is necessary at this stage. If she is negative for TRAb then a Tc-99m thyroid scan may clarify the cause of hyperthyroidism. If a nodule had been palpated on clinical examination then it would be reasonable to also order a thyroid ultrasound scan.
Result: The patient’s TRAb result is strongly positive at 20 mIU/L (RR <2 mIU/L).
How should the patient be managed?
This patient has clinical and biochemical thyrotoxicosis and should be commenced on carbimazole at a high dose, initially guided by an endocrinologist. She should be counselled on the potential adverse effects of carbimazole, including agranulocytosis, liver dysfunction and rash. Beta-blockers such as propranolol may also be indicated to provide symptomatic relief while she is thyrotoxic. Propylthiouracil is second-line therapy and usually reserved for treatment in the first trimester of pregnancy or for those who are allergic to carbimazole.
Given that this woman is of childbearing age, she should be counselled about the need for family planning. As carbimazole and propylthiouracil are both teratogenic, ideally women with Graves’ disease should not become pregnant until they are in remission. However, if a patient becomes pregnant while taking an antithyroid drug then propylthiouracil is preferred during the first trimester, and specialist involvement is crucial.5 If TRAb is present then it can cross the placenta during pregnancy and cause neonatal thyrotoxicosis, even in babies of mothers who are euthyroid throughout pregnancy.
Case 2. An older woman with low TSH but normal T3 and T4 levels
A 70-year-old woman presents to her GP for a routine annual health review. She has a history of osteoporosis, hypertension and one episode of atrial fibrillation five years ago. She is not taking any medication apart from vitamin D. On examination, she is clinically euthyroid. Blood tests reveal a low TSH level (0.08 mIU/L) and normal levels of free T3 (6 pmol/L) and free T4 (16 pmol/L). She is negative for TRAb.
What investigations should be ordered?
This patient is likely to have subclinical hyperthyroidism, with the underlying cause not immediately apparent on examination. A Tc-99m thyroid scan would be useful to clarify the cause.
Result: A Tc-99m thyroid scan shows a hot nodule in the left thyroid lobe with suppressed uptake in the remainder of the thyroid (Figure c).
How should the patient be managed?
Given that this patient is over the age of 65 years and has a TSH level less than 0.1 mIU/L and a history of osteoporosis and atrial fibrillation, treatment is indicated (Flowchart 1).6 The ideal treatment would be a single small dose of radioactive iodine to ablate the toxic adenoma. If she has contraindications to radioactive iodine, an alternative is carbimazole treatment. However, this may be needed long term, as spontaneous remissions of hot nodules are rare.
{kind=link}
Case 3. A patient taking lithium
A 51-year-old woman with long-term bipolar disorder has her condition well controlled with lithium treatment. Her GP checks her thyroid function every six months and notes that her thyroid function has become abnormal, with a low TSH level (0.03 mIU/L), raised free T3 (7.3 pmol/L) and free T4 at the upper limit of the reference range (20 pmol/L). She has no new symptoms but examination shows some asymmetry of the thyroid. The GP refers her for a thyroid ultrasound examination, which shows a 1.6 cm spongiform nodule in the right lower pole and some heterogenous echotexture in the remaining thyroid tissue.
What tests should be ordered next?
Lithium has been associated with both hyperthyroidism and hypothyroidism, although more commonly the latter.7 This patient is likely to have lithium-induced hyperthyroidism. A TRAb test should be ordered to exclude Graves’ disease. If this is negative for TRAb then the next step would be to order a Tc-99m thyroid scan.
The presence of a thyroid nodule with spongiform characteristics on ultrasound examination indicates a low suspicion of malignancy. Nodules with this appearance that are less than 2 cm in size do not require fine needle aspiration biopsy, according to current American Thyroid Association guidelines.8 Isotope uptake by the nodule on a Tc-99m thyroid scan would be additionally reassuring, as functioning thyroid nodules have a negligible risk of malignancy.
Result: A Tc-99m isotope thyroid scan shows low uptake in the thyroid gland (Figure d).
How should this patient be managed and followed up?
Results of the Tc-99m thyroid scan are consistent with lithium-induced thyroiditis. This is likely to resolve spontaneously, with return to a euthyroid state. Some patients with painless thyroiditis eventually develop hypothyroidism, and in 20 to 30% of cases this is permanent.9 This patient requires regular thyroid function monitoring at least monthly for three to six months to ensure she returns to a euthyroid state. If hypothyroidism develops, she should begin thyroxine replacement therapy.
Hypothyroidism
When should hypothyroidism be suspected?
Symptoms that may be associated with hypothyroidism include lethargy, weight gain, hyperlipidaemia, constipation, mood disturbance and hair loss. Causes of hypothyroidism are shown in the Box. Autoimmune (Hashimoto’s) thyroiditis is the most common cause of hypothyroidism.
What investigations should be ordered?
Measurement of TSH level is again the key screening test, followed by free T4 level if the TSH level is abnormal. The free T3 level is likely to be normal unless the hypothyroidism is advanced. In patients with hypothyroidism, the presence of anti-TPO antibodies suggests Hashimoto’s thyroiditis, although it is not specific. A thyroid ultrasound examination can be considered if there are structural abnormalities on clinical examination. Tc-99m thyroid scans are not helpful in investigating patients with hypothyroidism.
An approach to the investigation of patients with suspected hypothyroidism is shown in Flowchart 2.
Case 4. A young man with fatigue
A 32-year-old man presents to his GP with fatigue. He has a diffuse nontender goitre. Blood tests reveal a raised TSH level (105 mIU/L), free T3 level in the reference range (3.4 pmol/L), low free T4 level (9 pmol/L) and anti-TPO antibodies (greater than 1300 mIU/L; RR <40 mIU/L). A thyroid ultrasound examination shows a diffusely enlarged gland with increased vascularity, but no nodules are seen.
What levothyroxine dose is needed initially?
This presentation is consistent with overt hypothyroidism secondary to Hashimoto’s thyroiditis. Thyroxine replacement with levothyroxine is indicated. A reasonable starting dose of levothyroxine is 1.6 mcg/kg body weight, although a lower starting dose should be considered in older patients and those with a history of cardiac disease. The dose is related to lean body mass.
When should TSH be remeasured and how should levothyroxine dose be titrated?
TSH levels can take four to six weeks to respond to any adjustments in levothyroxine dosage. If symptoms are improving, TSH needs to be remeasured only four to six weeks after commencement or a dose change. If symptoms are not resolving, thyroid function tests can be repeated earlier, while recognising that the values will not be at steady state.
Case 5. A woman with Hashimoto’s thyroiditis planning pregnancy
A 26-year-old woman who is planning to conceive in the near future presents to her GP for advice. She has a history of Hashimoto’s thyroiditis and is taking 50 mcg levothyroxine daily. Her blood tests reveal normal levels of TSH (1.5 mIU/L), free T3 (4 pmol/L) and free T4 (14 pmol/L).
How should this patient be counselled?
Thyroxine requirements are higher in pregnancy. The patient should be advised to have baseline TSH testing and to increase her levothyroxine dose by 25 to 50% from the time of her first positive pregnancy test or sooner if the baseline TSH level is greater than 2.5 mIU/L.5
The patient becomes pregnant and increases her thyroxine dose to 75 mcg daily. She has further thyroid function blood tests four weeks later (at 10 weeks' gestation).
Results: The patient's thyroid function test results at 10 weeks’ gestation are in the normal range for the first trimester: TSH 1.7 mIU/L, free T3 5 pmol/L and free T4 13 pmol/L.
How should she be managed during pregnancy?
It is important to maintain a euthyroid state during pregnancy. Current guidelines recommend maintaining the TSH level either within specific trimester ranges for the assay (these can vary between laboratories) or alternatively at a TSH target level less than 2.5 mIU/L in the first trimester and less than 3.0 mIU/L in the second and third trimesters.5 It should be noted that targets remain controversial because of a lack of high-level evidence and that the normal range varies between trimesters.
This patient’s TSH level at 10 weeks’ gestation (1.7 mIU/L) is on target for the first trimester, indicating that the initial levothyroxine dose increase was adequate. Subsequently during the pregnancy, her thyroid function needs to be monitored about every four weeks in the first two trimesters and less frequently in the third trimester with the aim of maintaining a euthyroid state.5 She should receive care from both an obstetrician and an endocrinologist, if available. Postpartum levothyroxine adjustments are individualised depending on the incremental dose escalation required in pregnancy and should be guided by the treating specialist.
Case 6. An older woman with high TSH but normal T4
A 76-year-old woman presents to her GP for a routine annual review. She has a history of hypertension but is otherwise well. Her only medication is perindopril. Routine blood tests reveal a raised TSH level (6 mIU/L) and normal free T4 level (15 pmol/L). She has no symptoms and is clinically euthyroid.
How should this patient be managed?
This patient has subclinical hypothyroidism. Given her age, lack of symptoms and the small increase in TSH level, treatment is not recommended at this stage (see Flowchart 2).10 She should have a repeat TSH test in three to four months. There is no evidence that correcting a mild TSH elevation in this setting improves outcomes for older patients.11
Conclusion
The differential diagnosis of thyroid dysfunction is broad and identifying the underlying aetiology can be complex. The starting point should always be history, clinical assessment and blood tests to assess the severity of thyroid dysfunction. Thyroid autoantibodies should be measured only in patients with suspected or proven thyroid dysfunction and can help support a diagnosis. Imaging studies should be tailored towards the suspected type of thyroid dysfunction, with Tc-99m thyroid scans being useful in determining the cause of hyperthyroidism, and ultrasound examination being helpful in characterising structural abnormalities. Specialist referral should be considered for all patients with thyroid dysfunction, but particularly those with severe dysfunction based on symptoms or blood tests, patients with hyperthyroidism warranting treatment and pregnant women. MT