Take-home intranasal naloxone to prevent opioid overdose deaths

Take-home naloxone interventions are an effective and simple strategy to reduce opioid overdose morbidity and deaths. The recent PBS-listing of an intranasal naloxone product has the potential to increase uptake of these interventions.
Opioid overdose deaths continue to increase in Australia and are most often associated with the use of prescription opioids and other sedatives. An effective and simple strategy to reduce opioid overdose morbidity and mortality is the provision of take-home naloxone interventions (involving education and supply of naloxone) for patients and carers to use in the event of a suspected overdose in the community. The recent introduction of a PBS-listed intranasal naloxone product has the potential to facilitate uptake of take-home naloxone interventions.
This article describes the naloxone products available for take-home interventions, including the recently PBS-listed intranasal naloxone product, and the principles of their use. Practical tips are provided on who should have access to these interventions and how to deliver them in general practice.
Opioid overdoses in Australia
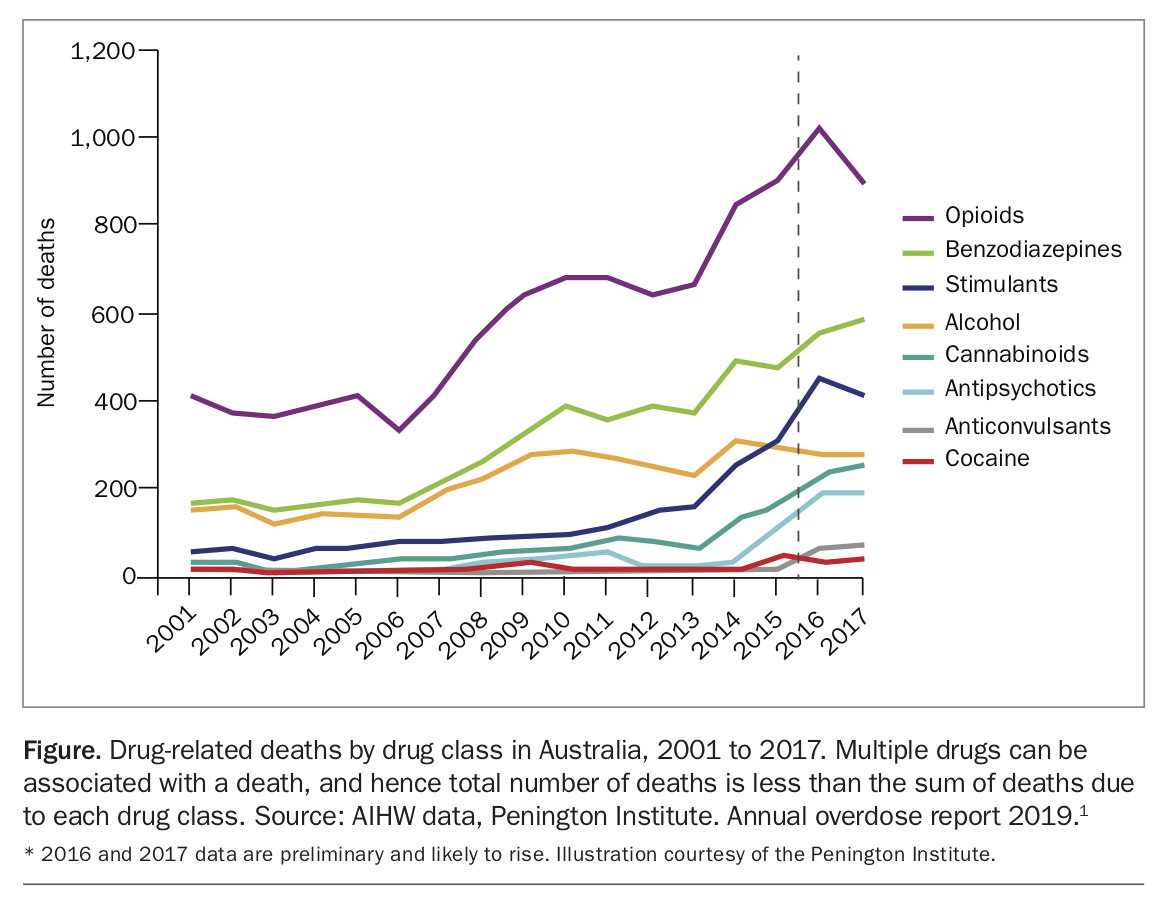
Rates of overdose from both prescription and illicit opioids have increased by 144% in Australia over the past 15 years (Figure).1 In 2017, there were more than 900 opioid-related overdose deaths in Australia – almost three deaths a day.1,2 Deaths from unintentional drug overdose now exceed road traffic fatalities (1612 compared with 1246 in 2017), and accidental poisoning is the second most common cause of mortality in Australians aged 25 to 44 years.3 Harm from overdose is not limited to death; nonfatal overdoses can cause long-term cognitive impairment, physical disability and psychological trauma to individuals and also affect their families and friends.
{kind=link}
The profile of overdose deaths in Australia has also changed in the past 15 years; most overdose deaths now occur in men aged 30 to 49 years, about two-thirds involve prescription opioids and one-third heroin, and most overdose deaths occur in combination with other sedatives such as alcohol, benzodiazepines and other prescription drugs. People from regional areas and those of Aboriginal background have higher rates of overdose.1,2
As most overdoses are related to prescription medicines, we as health professionals have a responsibility to address this increasing cause of mortality and morbidity. An effective and simple strategy to achieve this is to provide ‘take-home naloxone’ interventions to people who are likely to experience or witness an opioid overdose, including patients prescribed opioids for pain.
What is naloxone and what are take-home naloxone interventions?
Naloxone is a short-acting opioid antagonist medication that has been used to reverse opioid overdose for decades by doctors and paramedics in emergency settings. Naloxone displaces opioids from opioid receptors, reversing the respiratory depression underlying overdose deaths. It has a rapid onset of action (usually within two to three minutes), with effects lasting about one hour. Naloxone is registered as a Schedule 3 medicine and is available on prescription and over the counter at pharmacies.
The principle behind take-home naloxone interventions is straightforward – they empower patients and their carers to address overdose by providing them with:
- education on how to prevent, identify and respond to a suspected opioid overdose
- naloxone medication in a fit-for-purpose and easy to use formulation in the event of a suspected overdose.
In many ways take-home naloxone interventions resemble the ‘epinephrine autoinjector’ model for patients at risk of anaphylaxis and their families.
Take-home naloxone interventions have been repeatedly shown to be effective in reducing deaths from overdose, do not encourage increased substance use or other risk behaviours in patients, and are recommended by the WHO.4,5 About 20 to 30% of take-home naloxone supplies are used by consumers and carers to reverse an overdose, and US estimates suggest one overdose death is prevented for every 227 take-home naloxone interventions (95% confidence interval, 71 to 716).6
What take-home naloxone formulations are available?
Two naloxone formulations suitable for take-home use are now available in Australia for reversal of a suspected opioid overdose.
A naloxone solution for intramuscular injection (Prenoxad) has been available in Australia for several years. Although not registered in Australia, it is approved in the UK and has been granted temporary approval by the TGA. This product comprises a 2 mL prefilled syringe containing five 0.4 mg doses, supplied with two 23-gauge needles. Recommended dosing is 0.4 mg (0.4 mL) intramuscularly every two to three minutes until the overdose is reversed (i.e. the patient is conscious and breathing normally).7,8 This naloxone solution is not subsidised by the PBS, often costing consumers $50 to $60 per pack, with or without a prescription.
An intranasal naloxone product (Nyxoid), delivering a single dose of 1.8 mg naloxone (in a concentrated 0.1 mL volume) through a nasal applicator inserted into the nostril, was recently registered by the TGA. The intranasal naloxone dose has been calculated to provide a plasma concentration equivalent to the usual 0.4 mg intramuscular naloxone dose within the first two to five minutes after dosing, and has a prolonged duration of action compared with intramuscular naloxone, with effects lasting one to two hours.9 Each pack of intranasal naloxone contains two single intranasal applicators. If the patient has not recovered (overdose reversed) within two to three minutes after the first dose, a second dose should be administered into the other nostril.
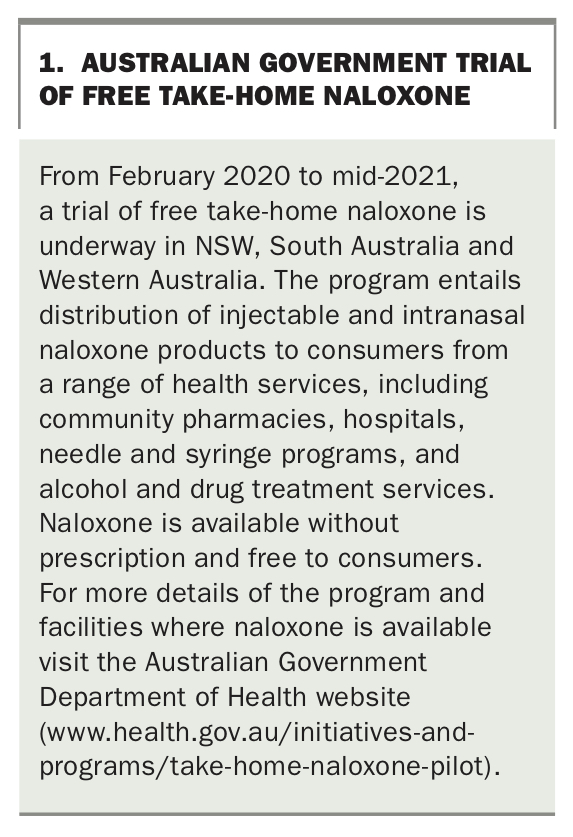
Intranasal naloxone was recently approved as a PBS-subsidised medication and thus costs $6.60 for concession card holders and $41 for general Medicare card holders on prescription. It is also available over the counter but at a higher cost to the consumer (often more than $60 per packet). However, consumers in NSW, Western Australia and South Australia can access free naloxone products from health services (including community pharmacies) participating in a pilot program (see Box 1).
{kind=link}
Although both the injected and intranasal products are effective, the intranasal product may be preferred by many patients and carers because of the PBS subsidy and ease of use, storage and training. In addition, injectable products can be difficult or stigmatising for some people to have in their possession. Studies of opioid users and carers suggest a preference for intranasal over injected naloxone formulations.10-12
A third naloxone product, naloxone ampoules for injection, is also available and is practical for use in emergencies by health professionals. However, this product is not suited to use by lay people, requires a separate supply of needles and syringes and is not recommended for use in take-home naloxone interventions.
Naloxone causes few adverse events and has no abuse potential. Patient violence or aggression due to precipitated opioid withdrawal reactions after naloxone reversal is rare when using the low naloxone doses in take-home naloxone interventions (e.g. 0.4 to 0.8 mg intramuscularly or 1.8 to 3.6 mg intranasally).
For whom is a take-home naloxone intervention suitable?
Take-home naloxone interventions should target:
- people who use opioids
- their carers (e.g. family and friends) who may witness an overdose – that is, be the ‘first responder’.
Data regarding opioid overdoses can inform who should be targeted:
- About 60 to 70% of fatal accidental opioid overdoses occur in people using prescription opioids, such as oxycodone, morphine and fentanyl, compared with about 30 to 40% in people using heroin
- Higher opioid doses are associated with increased risk of overdose
- Most overdoses occur following the use of opioids with other sedatives, most commonly benzodiazepines, alcohol, antidepressants, antipsychotics and anticonvulsants (e.g. pregabalin)
- Overdoses are more likely to occur when people resume opioid use after a period of reduced tolerance to opioids, such as after attempts at reduced opioid use (e.g. following a withdrawal or ‘deprescribing’ attempt) or interruptions in use (e.g. incarceration, travel or hospitalisation)
- Opioid overdoses are also more likely to occur when people use opioids not as prescribed, such as increased doses or by other routes (e.g. injected or oral use of a fentanyl topical patch). This pattern of use is more likely in people with a history of a substance use disorder (to opioids, alcohol or other drugs)
- Patients with respiratory, cardiovascular or hepatic impairment are also more susceptible to the risk of overdose from sedative drugs.
The US Centers for Disease Control and Prevention published guidelines in 2016 that state ‘clinicians should consider offering naloxone when prescribing opioids to patients at increased risk for overdose, including patients with a history of overdose, patients with a history of substance use disorder, patients taking benzodiazepines with opioids … (or) patients taking higher dosages of opioids (≥50 OME [oral morphine equivalents]/day)’.13 Of concern, most (78%) of a national Australian cohort of 1514 patients with chronic noncancer pain prescribed Schedule 8 opioids met this risk profile: 65% were using 50 mg OME or more daily, 38% met criteria for a substance use disorder (most commonly alcohol), 34% reported concurrent benzodiazepine use, and 17% reported a previous overdose.14 When participants in the same cohort were asked about their perspectives regarding overdose, many had a poor understanding of the signs, symptoms, potential consequences or appropriate responses to an overdose. However, after receiving information on naloxone, most participants (60%) were supportive and few (13%) were not supportive of receiving a take-home naloxone intervention from their opioid prescriber.15
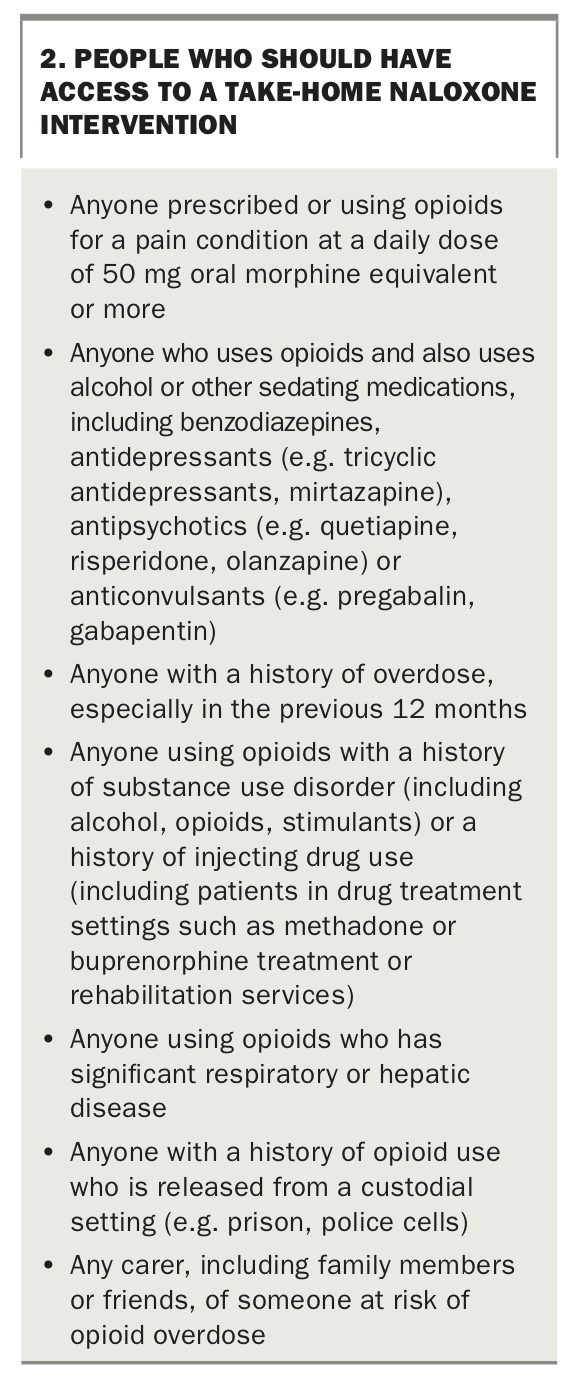
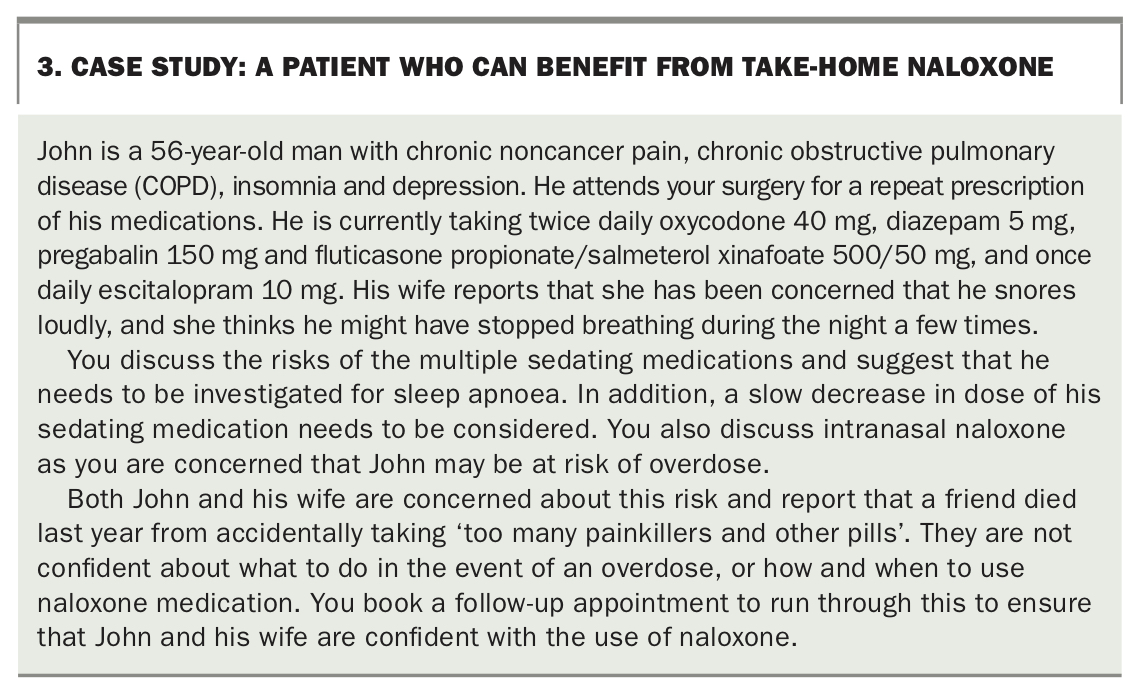
In Australia, we recommend that take-home naloxone interventions are made widely available by health providers to people at risk of overdose. People at risk of overdose who should be targeted for take-home naloxone are listed in Box 2, and an example of a patient who could benefit is described in the case study in Box 3. Carers of people who meet these criteria, including family members and friends, should also be included as candidates for take-home naloxone interventions, given they may be first responders to an overdose.
{kind=link}
{kind=link}
How to deliver a take-home intervention
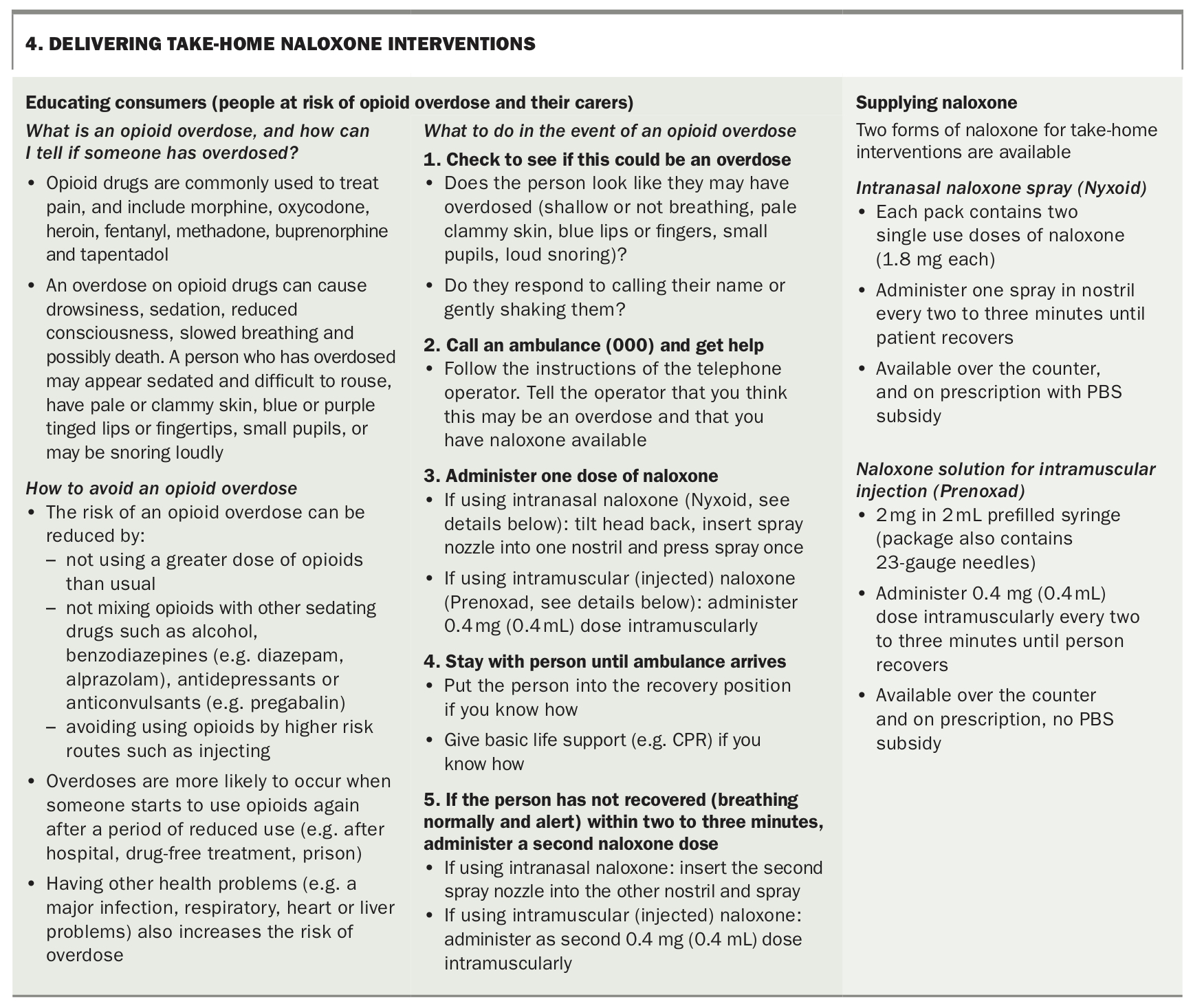
Health professionals can effectively deliver a brief take-home naloxone intervention in around five to 10 minutes. Clinicians need to be aware that discussing previous overdose can be difficult for some patients and carers. Key messages regarding consumer education and use of naloxone are shown in Box 4.
{kind=link}
Who in the health system is responsible for delivering take-home naloxone interventions?
To reach people at risk of overdose (and their carers) effectively, we need a whole-of-health-system response to providing take-home naloxone interventions. This includes:
- GPs and pain and other medical specialists who prescribe opioids to their patients
- community pharmacists who dispense opioids to their patients
- emergency department services before discharge of patients who have presented with an opioid overdose
- hospitals as part of discharge planning for patients who meet the above criteria
- alcohol and other drug treatment providers, including withdrawal, rehabilitation, counselling and opioid treatment services (methadone and buprenorphine treatment)
- health services that work with patient groups with high levels of substance use, including corrections, mental health and homeless services
- needle and syringe services and supervised injecting centres.
What else do we need to do to reduce accidental overdose deaths?
Take-home naloxone interventions are one strategy to reduce opioid-related overdose deaths. A range of other approaches are also required to achieve this goal, including: safer and more effective prescribing of opioids and other sedatives; better access to multidisciplinary treatment approaches for patients with complex conditions such as chronic pain and/or substance use disorders; better co-ordination between health care providers, including the use of shared health records (e.g. My Health Record) and prescription monitoring systems; better education of consumers and health providers regarding opioid-related harms; and co-ordination of efforts across governments, health providers, consumers and industry through the development of a national strategy to reduce opioid-related overdose deaths.
Conclusion
Take-home naloxone interventions are an effective approach to reduce opioid-related overdose deaths, which have increased in Australia over the past 15 years commensurate with the increased rates of opioid prescribing. Take-home naloxone interventions can be delivered in a five to 10 minute consultation, and should be considered as an essential part of safe opioid prescribing by medical practitioners. The introduction of intranasal naloxone on the PBS should increase the acceptability of this potentially life-saving intervention. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.