An update on gestational diabetes mellitus

GPs play a key role in identifying and counselling women at high risk of gestational diabetes mellitus (GDM) before pregnancy, organising early testing to detect diabetes in pregnancy, ensuring timely postpartum follow-up and risk-factor modification and encouraging a healthy lifestyle to reduce the effects of GDM for women and their children. The Australasian Diabetes in Pregnancy Society revised consensus guidelines remain standard of care.
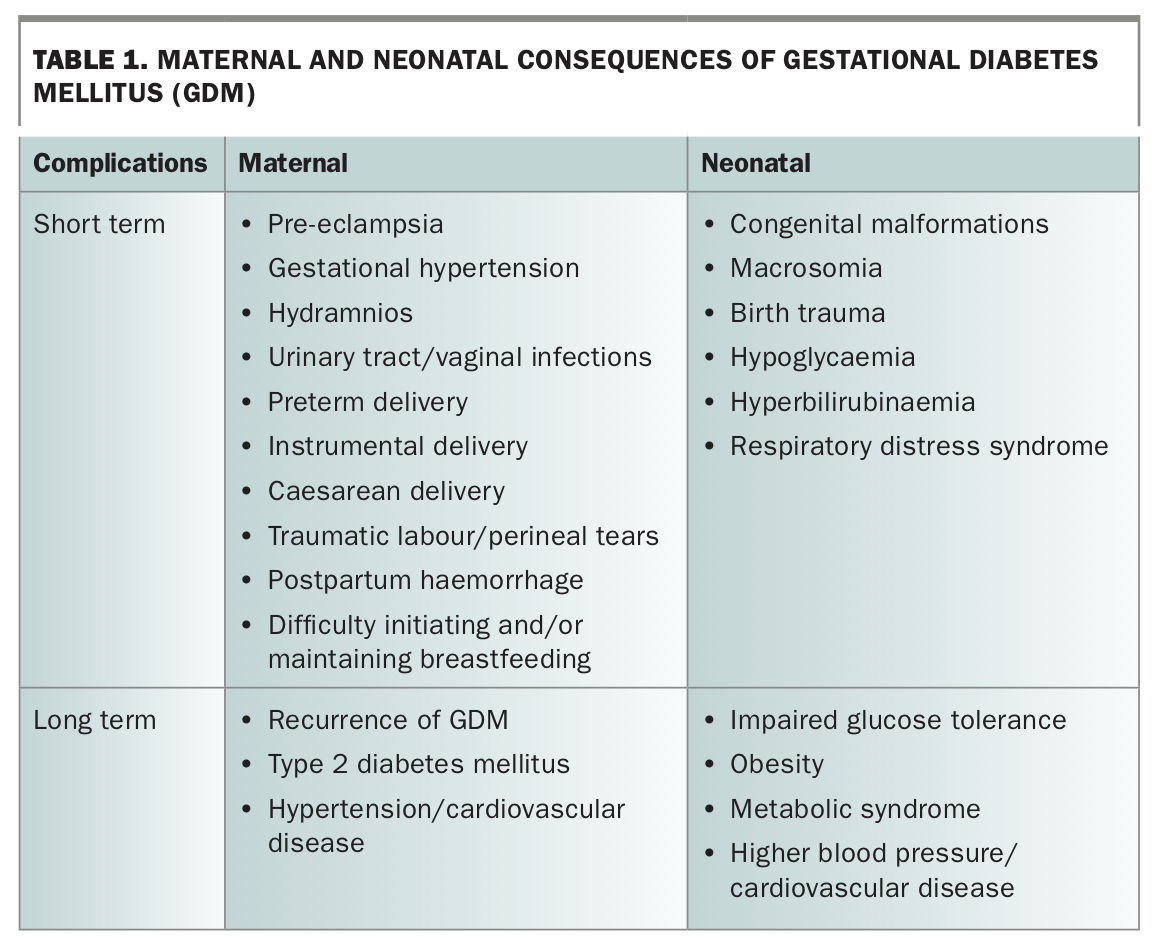
- Gestational diabetes mellitus (GDM) is associated with several short- and long-term adverse maternal and neonatal outcomes.
- The prevalence of GDM in Australia has risen with an increase in maternal risk factors such as obesity and implementation of the revised Australasian Diabetes in Pregnancy Society (ADIPS) diagnostic criteria.
- All women should be encouraged by their primary care provider to plan for pregnancy, and planning should include prepregnancy risk stratification and, in high-risk women, blood glucose assessment for detection of pre-existing glucose intolerance or undiagnosed diabetes.
- High-risk women who have not undergone prepregnancy blood glucose assessment should be tested early for diabetes in pregnancy (DIP) and receive increased antenatal monitoring to reduce the risk of pregnancy complications.
- Universal testing for GDM with a 75g two-hour oral glucose tolerance test (OGTT) at 24 to 28 weeks’ gestation is recommended.
- Treatment of GDM ideally involves a multidisciplinary approach focusing on patient education, dietary modification and physical activity.
- Women should monitor their blood glucose levels regularly, and pharmacotherapy (usually insulin) should be initiated if levels are elevated despite lifestyle optimisation.
- GPs play a crucial role in prepregnancy counselling and in identifying and screening high-risk women for DIP before pregnancy or in early pregnancy.
- GPs are ideally placed to facilitate postpartum follow-up and risk factor modification to reduce the increased risk of type 2 diabetes and cardiovascular disease in women with GDM and their offspring.
Gestational diabetes mellitus (GDM) is a common medical disorder of pregnancy and is defined as any degree of glucose intolerance with onset or first recognition during pregnancy.1 It is associated with adverse pregnancy outcomes due to maternal hyperglycaemia, conferring a lifetime increased risk of diabetes, obesity and cardiovascular disease on both mother and child.2-6
The increasing prevalence of GDM has had a significant impact on limited antenatal resources in Australia and internationally. It reflects an increase in risk factors such as maternal obesity, advanced maternal age, an increasingly multiethnic population and the implementation of the revised International Association of the Diabetes and Pregnancy Study Groups’ (IADPSG) diagnostic procedures and criteria for GDM, which are endorsed by the Australasian Diabetes in Pregnancy Society (ADIPS).2,7
On this background, GPs should encourage all women to undergo prepregnancy planning to identify women who warrant screening for diabetes before pregnancy and to target modifiable risk factors for GDM such as obesity. In addition, GPs are best placed to organise early pregnancy testing for diabetes in pregnancy (DIP) for high-risk women who were not tested before pregnancy. After pregnancy, GPs play an important role in screening for type 2 diabetes and cardiovascular disease and in promoting healthy lifestyle strategies to reduce the long-term intergenerational risk associated with GDM.
This article highlights evidence-based key practice points for GPs in the diagnosis and management of GDM and provides a guide to pre- and postpregnancy management that aims to optimise short- and long-term outcomes related to GDM.
Incidence and prevalence of GDM
The Australian Institute of Health and Welfare (AIHW) reported an overall incidence of GDM in Australia in 2016-17 of 15%.8 However, this underestimates the incidence of GDM in areas with a significant multiethnic population, with the prevalence of GDM in south-western Sydney reported to be 30%.9
The revised ADIPS diagnostic pathway and criteria have increased the number of women diagnosed with GDM in Australia, due to the recommendation for universal testing, lowering of the fasting-glucose cut-off and introduction of a 1-hour glucose cut-off for the 75 g 2-hour oral glucose tolerance test (OGTT). These changes, together with the higher 2-hour glucose OGTT cut-off, have also led to local differences in the prevalence of GDM diagnosis depending on the distribution of local population risk factors and demographic characteristics. For example, the lower fasting-glucose cut-off is strongly associated with South Asian ethnicity and prepregnancy overweight and obesity.10
Using these revised criteria, the overall incidence of GDM in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study cohort was 17.8%; however, there was a marked variation between different study centres (ranging from 9.3% in Israel to 25.5% in California).11 In a high-risk region in Australia, the prevalence of GDM increased from 14.8% to 29.6%.9 This increase in GDM was projected to lead to a greater than 30% increase in workload in Australia.12
The rising prevalence of GDM and related resource demand underscores the importance of prepregnancy planning, lifestyle optimisation and early identification of women and pregnancies most at risk for GDM and for related poor pregnancy outcomes.
Pathophysiology
GDM occurs when the maternal pancreas is unable to secrete enough insulin to overcome pregnancy-induced insulin resistance. This insulin resistance is due to gestational weight gain (GWG) and placental secretion of hormones (i.e. growth hormone, corticotrophin releasing hormone, human placental lactogen, prolactin, oestrogen and progesterone). Insulin resistance and reduced insulin secretory capacity lead to decreased glucose uptake, leading to higher circulating maternal glucose and free fatty acids (FFA).13,14 The pathophysiology of GDM is therefore similar to type 2 diabetes, with increased insulin resistance and relative insulin deficiency.
The intergenerational consequences of GDM
The Pedersen hypothesis describes the relationship between maternal hyperglycaemia and excessive fetal growth.15 Increased maternal glucose crossing the placenta causes fetal hyperglycaemia, resulting in fetal hyperinsulinaemia, which in turn leads to accelerated fetal growth and fat deposition (Figure). This increases the risk of large-for-gestational-age (LGA) offspring and macrosomia (neonatal birthweight >4000 g).15,16
The HAPO study showed a continuous positive relationship between maternal blood glucose levels (BGLs) on the 75 g 2-hour OGTT and risk for poor pregnancy outcomes including caesarean section, LGA offspring and neonatal hypoglycaemia.17 There were also no clear blood glucose cut-offs at which the risk of these pregnancy outcomes significantly increased. These results, supported by other recent large studies, were the basis for the revised IADPSG recommendations for the diagnosis and classification of GDM, endorsed by ADIPS.3,8 More recently, the HAPO follow-up study (HAPO-FUS) demonstrated that offspring exposed to untreated GDM in utero had higher rates of impaired glucose tolerance at 10 to 14 years of age.6 The short- and long-term risks associated with GDM are summarised in Table 1.
{kind=link}
Prepregnancy counselling and risk assessment
Given the rising prevalence of risk factors for GDM such as obesity in women of childbearing age, GPs should encourage all women to participate in prepregnancy planning, focusing on optimisation of lifestyle and body mass index (BMI) before pregnancy. GWG targets should be discussed.18 GPs should also review current medications and determine their safety for pregnancy, advise women to commence an iodine and folate-containing supplement one month before conception and refer to the current guidelines by the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) or the Royal Australian College of General Practitioners for prepregnancy counselling and assessment.19,20 Routine blood tests for thyroid function, iron studies or vitamin D status are not recommended by RANZCOG in the prepregnancy period. However, testing should be considered if clinically indicated, for example in women with a personal or family history of thyroid disorders or other autoimmune conditions, a previous tendency to iron deficiency, and women at higher risk for vitamin D deficiency due to low sun exposure.
Ideally, GPs should perform prepregnancy glucose assessment in high-risk women to determine if pre-existing glucose intolerance or undiagnosed type 2 diabetes is present, so that diabetes management can be initiated and stabilised before pregnancy to reduce the risk of pregnancy complications. High-risk women who have not undertaken prepregnancy glucose testing should also have early pregnancy testing organised at the initial antenatal visit with the GP and, if positive, be referred promptly to a specialised diabetes in pregnancy service.
Maternal hyperglycaemia in early pregnancy: DIP and early GDM
Early testing in pregnancy aims to detect women with previously undiagnosed pre-existing diabetes (i.e. DIP), defined as:
- fasting BGL ≥7.0 mmol/L
- random BGL of ≥11.1 mmol/L; or
- glycated haemoglobin (HbA1c) level ≥6.5% (48 mmol/mol).
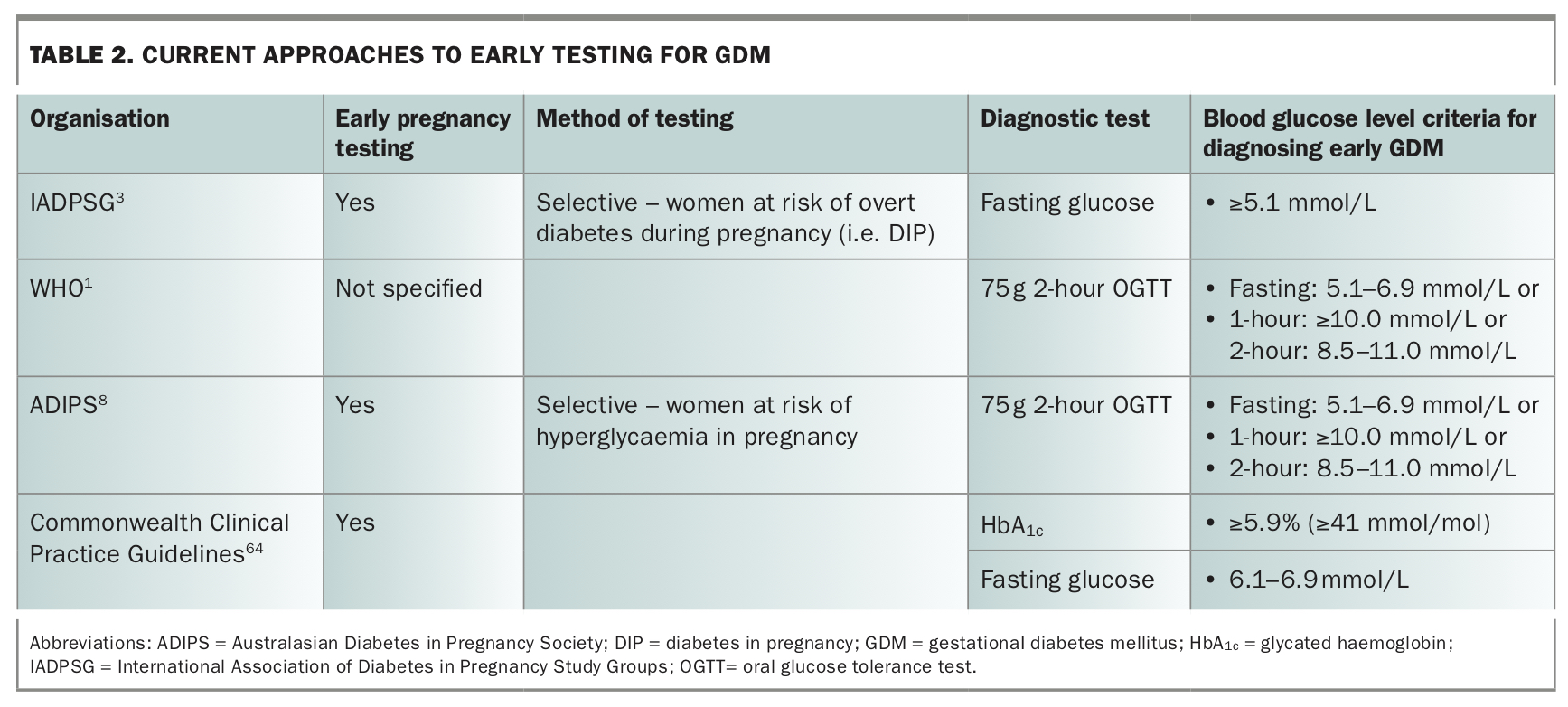
The IADPSG has highlighted the need to identify these women early in pregnancy given the potential higher risk of poor pregnancy outcomes related to their greater degree of early hyperglycaemia.3 It is important to note that DIP does not necessarily correspond to type 2 diabetes, and therefore these women must be tested after the birth to confirm their glucose status. Early testing will also lead to increased detection of milder maternal hyperglycaemia or abnormal glucose tolerance before 24 weeks’ gestation (early GDM). Retrospective studies have shown that women with early GDM are at greater risk of poor pregnancy outcomes.21 Currently, there is no consensus for either the levels of maternal glycaemia that should be used to define early GDM or the preferred early testing approach. Specific issues with early GDM include the potential for overdiagnosis if testing occurs before the natural fall in fasting plasma glucose in the first trimester of pregnancy and that the 5.1 mmol/L glucose threshold in early pregnancy is poorly predictive of GDM detected at 24 to 28 weeks’ gestation.22,23 Various recommendations for identifying early GDM are summarised in Table 2.
{kind=link}
Evidence is also lacking for whether diagnosing and treating early GDM improves pregnancy outcomes. A recent randomised controlled trial evaluating whether early diagnosis and treatment of GDM improves perinatal outcomes in obese women in the US reported that early screening did not reduce the risk of adverse pregnancy outcomes.24 However, in the early screening group, the average gestational age at GDM diagnosis was 24 ± 5 weeks compared with 27 ± 2 weeks in the routine screening group. Consequently, most women who were screened early did not receive treatment for GDM until later in pregnancy. The Australian Treatment of Booking Gestational Diabetes Mellitus (TOBOGM) Study, evaluating the impact on obstetric outcomes of immediate versus delayed care for gestational diabetes diagnosed at booking, is ongoing (ACTRN12616000924459).
Risk factors
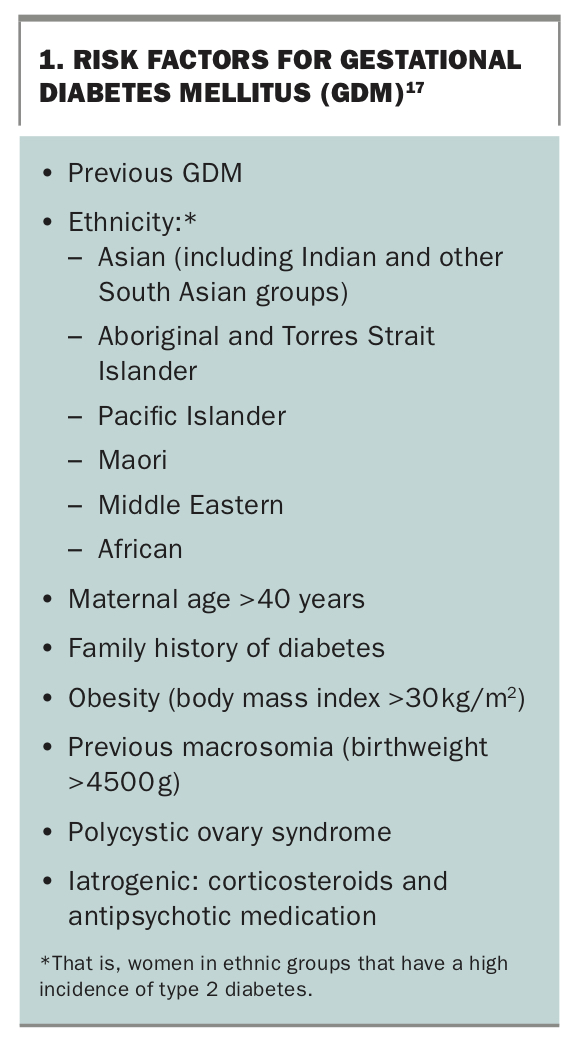
Risk factors for GDM are outlined in Box 1. As highlighted above, the primary aim of early testing is to detect women with DIP. However, ADIPS has also recommended that the presence of at least one risk factor for GDM should lead GPs to perform early diagnostic testing for GDM.8 Repeat testing using the OGTT should be performed at the time of universal testing at 24 to 28 weeks’ gestation if early testing is negative.
{kind=link}
Diagnosis of GDM
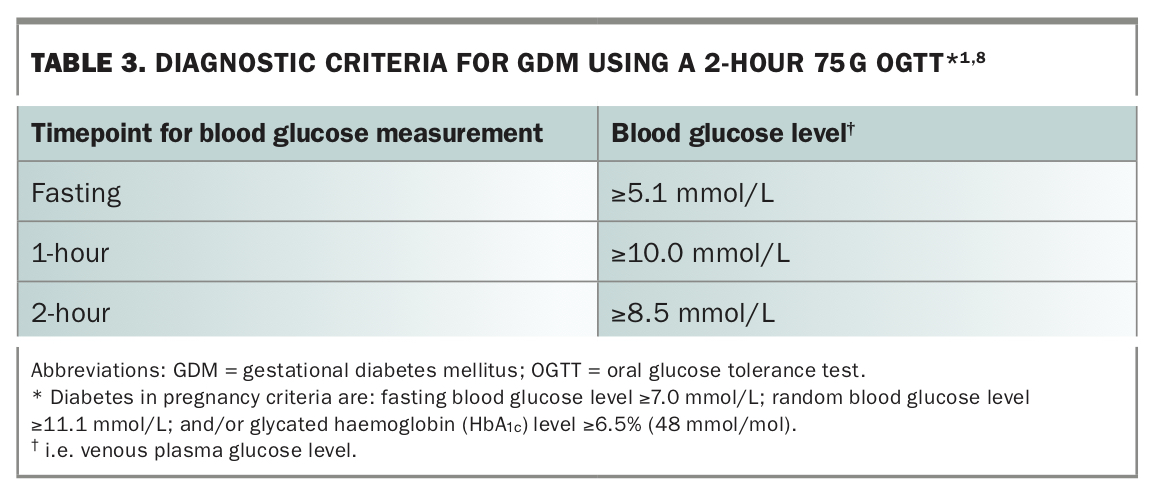
Universal testing for GDM with the 75 g 2-hour OGTT between 24 to 28 weeks’ gestation is recommended in Australia.8 The diagnostic criteria for GDM are summarised in Table 3. Only one abnormal BGL is required for diagnosis.
{kind=link}
As there were no clear glucose cut-offs for demonstrating greater risk in the HAPO trial, the IADPSG recommended diagnostic fasting, 1-hour and 2-hour glucose values for the 75 g 2-hour OGTT based on the average glucose values at which the odds of the primary outcomes were 1.75 times the odds of these outcomes occurring at the mean BGLs for the HAPO cohort.3
Treatment of GDM improves pregnancy outcomes
The Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) showed that treatment of GDM reduces the risk of macrosomia, serious perinatal complications including death and shoulder dystocia, and preeclampsia.25 The Maternal-Fetal Medicine Units Network (MFMU) Trial showed that treatment of mild GDM (defined as a fasting BGL <5.3 mmol/L) lowered the rate of macrosomia, caesarean section and gestational hypertension.26 A recent Cochrane review that included these two main trials showed that intensive treatment for GDM, which included dietary intervention and insulin therapy if required, reduced a composite outcome of perinatal morbidity (neonatal death, shoulder dystocia, bone fracture and nerve palsy), macrosomia and pre-eclampsia compared with standard antenatal care.27 Intensive treatment was, however, associated with greater likelihood of neonatal intensive care admission and induction of labour.
Interestingly, the ACHOIS and MFMU follow-up studies showed no difference in the rates of childhood obesity and glucose intolerance in the offspring of treated women compared with controls, despite treatment for GDM reducing the risk of macrosomia at birth.28,29 Both studies were underpowered to assess these long-term offspring outcomes. These data are nevertheless supported by other studies suggesting that the offspring of women with GDM, even when treated, are at greater risk of obesity, type 2 diabetes, the metabolic syndrome and cardiovascular disease from early childhood and adolescence.30 This may indicate that earlier intervention is required to address this persisting risk.
Evidence supporting the new diagnostic criteria for GDM
There is yet to be a randomised controlled trial evaluating pregnancy outcomes in women diagnosed with GDM based on the revised ADIPS diagnostic criteria. A retrospective Australian study in a high-risk population suggested that outcomes were similar between (untreated) women diagnosed with GDM by the revised ADIPS criteria and those who were diagnosed and treated for GDM based on previous criteria.9 In contrast, a larger Australian retrospective study reported that women with GDM based on the revised ADIPS criteria (i.e. untreated) had an increased risk of gestational hypertension, pre-eclampsia, induction of labour, caesarean section and LGA compared with women without GDM, although the revised criteria were ultimately an independent predictor only for induction of labour and LGA.31 Similarly, most international studies have shown that women who would now be diagnosed with GDM, but who were previously classified as having normal BGLs, were at increased risk for several adverse pregnancy outcomes compared with women who had normal BGLs based on the revised criteria.32,33 The evidence to date would therefore seem to support the identification of women with ‘milder’ GDM based on the revised ADIPS diagnostic criteria.
Management
The main objective in the treatment of GDM is to achieve normal maternal BGLs, thus reducing maternal and neonatal complications associated with even mild elevations of maternal BGLs. Patient education is key, and several online resources are available (e.g. ndss.com.au). Women should be supported by a multidisciplinary team including a diabetes educator, dietitian, endocrinologist, obstetric care provider and GP. The role of GPs in managing GDM is particularly important in smaller centres, remote and rural areas and for women at lower risk of adverse pregnancy outcomes. Women should be regularly reviewed for ongoing support and for assessment of their diet and blood glucose control.
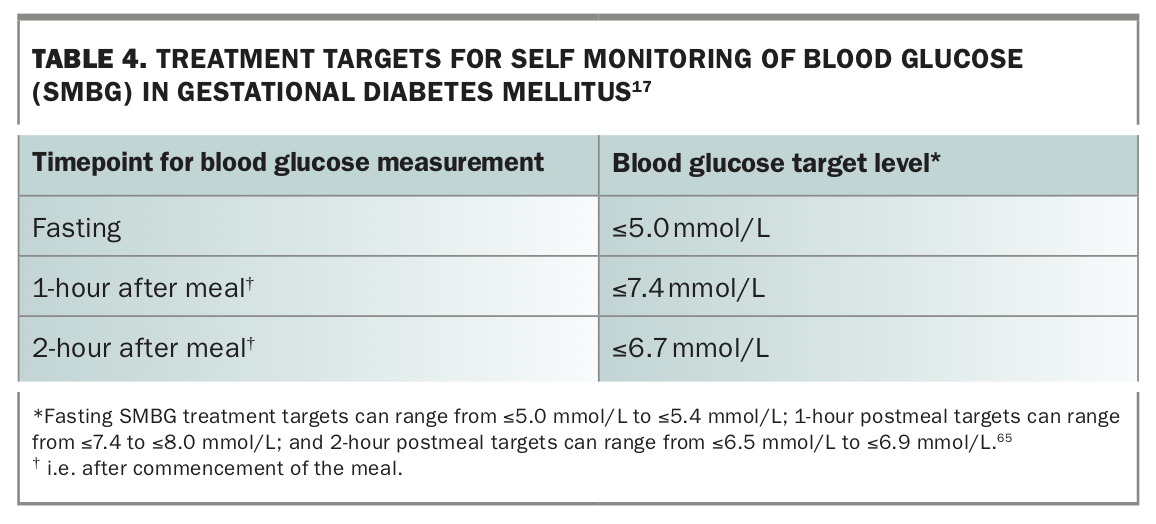
Self-monitoring of BGLs
Treatment targets based on self-monitoring of blood glucose (SMBG) are summarised in Table 4. Women with GDM should monitor their fasting and postmeal BGLs with blood glucose meters, usually four times daily. Either the 1-hour or 2-hour postmeal peak glucose measurement may be used, although the HAPO study demonstrated that the 1-hour BGL was more strongly associated with perinatal outcomes than the 2-hour BGL on the OGTT.17 The 1-hour postmeal BGL also corresponds to the peak glucose rise in pregnancy in women without diabetes and is associated with fetal abdominal circumference in women with type 1 diabetes.34,35
{kind=link}
The pattern or trend of maternal glucose is more important than occasional elevated BGLs in determining whether escalation of treatment is needed. HbA1c level may also be a useful tool for assessing blood glucose control.36,37
Lifestyle intervention
Dietary intervention
Nutrition therapy is first-line treatment for GDM, although the optimal dietary intervention for GDM remains unclear. A GDM diet should consist of 2000 to 2500 kcal per day, with a total daily carbohydrate intake of at least 175 g.38 Caloric restriction (<1200 kcal or 50% of total daily energy intake) may increase ketosis, and inadequate GWG (<5 kg) may increase the risk of small-for-gestational-age (SGA) offspring in women with overweight/obesity.39,40 Restriction should be suspected if there are clinical symptoms such as weakness, dizziness or nausea, low postmeal BGLs or weight plateau or loss during pregnancy and should be managed by further dietary education and closer antenatal monitoring.
Carbohydrate is the main determinant of postmeal BGLs, so an even distribution of preferably complex carbohydrates/ low glycaemic index food across the day is recommended to lower postmeal BGLs and avoid excessive GWG.38,41 Low-carbohydrate diets (<45% total daily energy intake) are not currently recommended in pregnancy due to the potential risk for nutritional deficiencies, and from the corresponding increase in intake of saturated fat, as maternal triglycerides and FFAs are associated with excessive fetal growth and LGA offspring.42,43 Low carbohydrate and/or hypocaloric diets also increase the ratio of glucagon to insulin, promoting oxidation of FFAs to beta-hydroxybutyrate and other ketones.44 A clinical correlation has been shown between persistently increased maternal beta-hydroxybutyrate and FFA levels in women with and without diabetes in pregnancy and lower offspring mental development and intelligence, demonstrating the potential negative effects of maternal ketonaemia on fetal brain development.45
Exercise
Exercise improves insulin sensitivity and reduces GWG. Regular moderate intensity exercise, such as walking for 20 to 30 minutes three to four times weekly, is recommended if there is no obstetric contraindication.46 Walking for 10 to 15 minutes after meals can also decrease the postmeal glucose peaks.
Gestational weight gain
The Institute of Medicine (IOM) has published general recommendations for weight gain during pregnancy based on prepregnancy BMI;18 however, there are no specific recommendations for weight gain in women with GDM. A recent large meta-analysis evaluating specifically the relationship between GWG and GDM showed that excessive GWG was associated with an increased risk of hypertensive disorders of pregnancy, caesarean section, LGA offspring, macrosomia and need for pharmacotherapy.47 Importantly, GWG below the IOM recommendations reduced the risk of LGA offspring and macrosomia without increasing the risk of SGA offspring.47 This suggests that GWG targets in GDM may need to be lower than the current recommendations for normal pregnancy.
Insulin
Targeted insulin therapy should be initiated if BGLs are consistently elevated at any one timepoint despite appropriate diet and postmeal activity. This is generally undertaken under specialist supervision and requires frequent review for individualised insulin dose titration. Depending on glucose targets and timing of diagnosis, 30 to 50% of women with GDM require medication, usually insulin therapy, to maintain normal BGLs, with a combination of evening intermediate-acting insulin if fasting BGLs are elevated and mealtime rapid-acting insulin when indicated.21,48 Additional daytime intermediate-acting insulin may also be needed to control prelunch or predinner hyperglycaemia.
Decreasing insulin requirements in the third trimester often reflect the physiological increase in maternal insulin sensitivity at this stage of pregnancy. However, significant insulin dose reduction, recurrent maternal hypoglycaemia and/or clinical evidence of placental dysfunction such as slowing of fetal growth or pre-eclampsia may indicate underlying pathophysiological placental insufficiency and therefore may impact on the timing of delivery and intensity of obstetric monitoring.49
Metformin
The use of metformin in the treatment of GDM remains controversial because of concerns over possible long-term effects of placental transfer of metformin to the fetus. The Metformin in Gestational Diabetes: The Offspring Follow-Up (MiG TOFU) two-year follow-up study found that children exposed to metformin had increased subcutaneous fat localised to the arm compared with children whose mothers were treated with insulin alone.50 By nine years of age the children exposed to metformin were larger overall.51 These findings are consistent with a recent follow-up study of metformin therapy in pregnant women with polycystic ovary syndrome, which showed that children exposed to metformin in utero had higher BMI and rates of overweight and obesity at 4 years of age.52 Practically speaking, many women treated with metformin still require the addition of insulin therapy to meet glycaemic targets in pregnancy, with the Metformin in Gestational Diabetes (MiG) trial showing that almost 50% of women treated with metformin required the addition of insulin therapy.48
Obstetric management
Women with GDM, particularly those diagnosed with early GDM, require increased obstetric monitoring. Serial fetal growth ultrasounds, particularly assessing fetal abdominal circumference, have been proposed as being potentially useful in guiding the intensity of maternal blood glucose targets and need for insulin therapy;53 however, this was not supported by a recent Cochrane review.54 Nevertheless, fetal ultrasound may identify intrauterine growth restriction or SGA offspring and prompt consideration of relaxing SMBG targets. Conversely, it may identify LGA offspring, accelerating growth and/or polyhydramnios, which should trigger review of glycaemic management and SMBG targets as well as factors such as excessive GWG.
The optimal timing of delivery for women with GDM has not been definitively established. Current guidance states that delivery can involve induction of labour from 39 weeks’ gestation guided by maternal glucose control, need for medications and relevant obstetric factors. Any decision for caesarean delivery should be determined by obstetric indications. Delivery is recommended by 40+6 weeks’ gestation in women with GDM managed with diet alone, and from 39+0 to 39+6 weeks’ gestation for women with GDM well controlled with therapy.55,56
\Women with GDM require intensive monitoring and control of blood glucose during labour to reduce the risk of neonatal hypoglycaemia.57 Intravenous insulin-glucose infusions are, however, only infrequently required, especially for women in whom BGLs have been within target range during pregnancy with lifestyle management alone.
Insulin therapy should be ceased immediately after delivery and neonates should be monitored for hypoglycaemia, respiratory distress and jaundice. Early breastfeeding may reduce the risk of neonatal hypoglycaemia.58 Women who required insulin treatment in pregnancy should have their BGLs checked by day three after delivery to ensure blood glucose has normalised before discharge.
Postpartum follow up: role of the GP
Women with significantly abnormal BGLs in early pregnancy may have pre-existing type 2 diabetes and should undertake an OGTT six to 12 weeks after the birth to assess their glucose status. Up to one-third of women with GDM will have postpartum type 2 diabetes or impaired glucose tolerance; however, less than 60% are ever formally tested.59,60
Women with GDM are at significant risk of recurrence of GDM in future pregnancies, with reported rates of 30 to 84%.4 GDM is also a risk factor for type 2 diabetes and cardiovascular disease, including hypertension. For example, GDM is associated with a sevenfold increased risk for developing type 2 diabetes, with a lifetime risk of around 50%.61 Women with previous GDM should therefore have regular testing for diabetes with a repeat OGTT annually if planning for further pregnancy. Alternatively, for longer term follow up, measurement of fasting glucose and HbA1c levels should be performed every one to two years. It is worth noting that neither test is particularly sensitive in detecting impaired glucose tolerance, and thus tracking any progressive rise over time may be more useful (i.e. a rising HbA1c of around 6.0% [42 mmol/mol] may warrant proceeding to OGTT to determine if impaired glucose tolerance is present). Women with GDM also have a twofold higher risk of clinical cardiovascular disease compared with women without GDM and should undergo regular cardiovascular risk assessment.5
Women and their families should also be encouraged to maintain a healthy lifestyle with a balanced diet and regular exercise to mitigate the intergenerational effects of GDM. Optimising weight after pregnancy has been associated with a reduced risk of developing GDM in subsequent pregnancies and of long-term complications. For example, studies have shown that up to 75% of obese women with previous GDM developed type 2 diabetes compared with less than 25% of women with previous GDM who achieved a normal BMI in the postpartum period.62 Furthermore, in overweight and obese women with GDM a reduction in BMI of 2.0 kg/m2 or more between pregnancies reduced the risk of GDM by 74%.63
Conclusion
The revised ADIPS guidelines lower the glucose thresholds for diagnosis and treatment of GDM, reflecting increasing evidence that links GDM to multiple adverse maternal and fetal outcomes even at low levels of maternal hyperglycaemia. As the prevalence of GDM continues to increase in Australia and the intergenerational effects of the disease become increasingly known, it is imperative to reduce this burden through effective prepregnancy counselling and risk assessment as well as early identification and better risk stratification of women at greatest risk of poor pregnancy outcomes to triage service delivery most effectively.
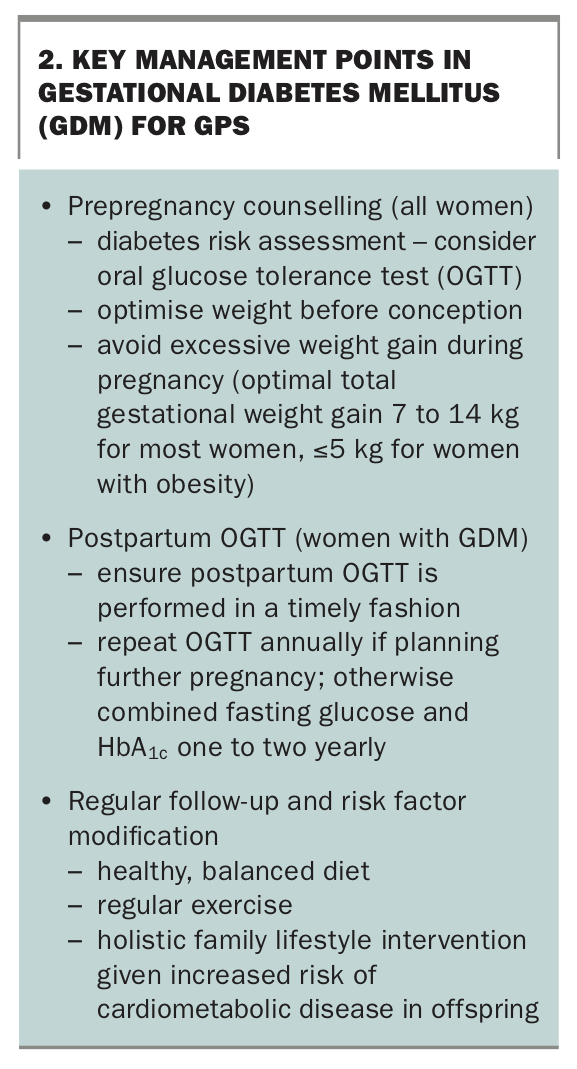
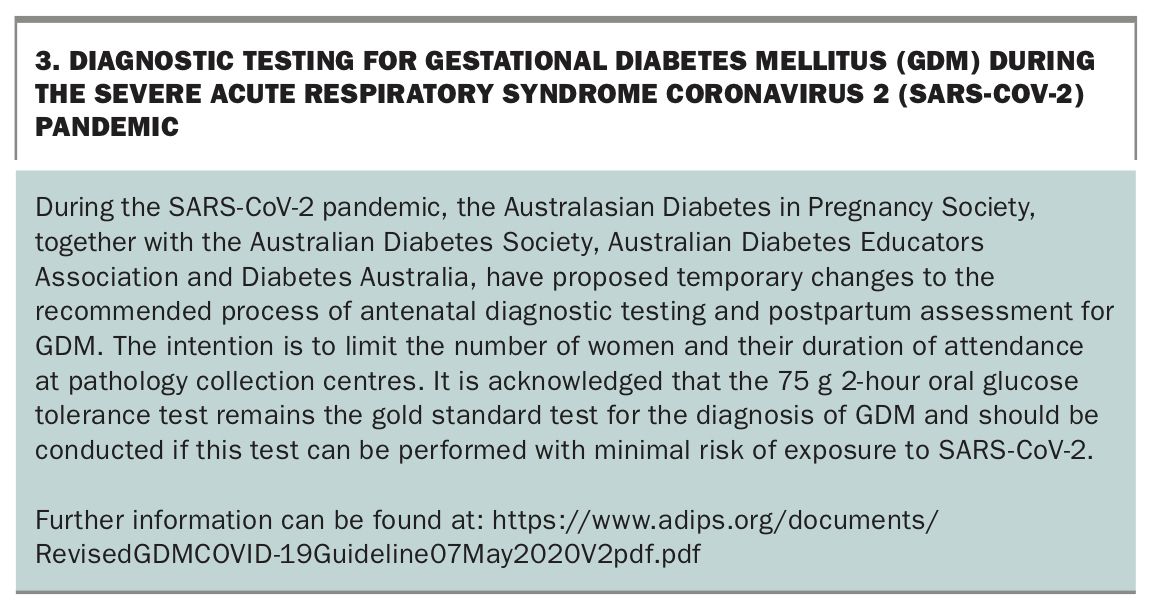
Key management points for GPs are summarised in Box 2, and proposed temporary changes to the recommended process of antenatal diagnostic testing and postpartum assessment for GDM in light of the current severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic are outlined in Box 3. GPs play a crucial role in early identification of GDM and undiagnosed pre-existing diabetes, thereby reducing maternal and neonatal morbidity. They are also well placed to support women with GDM management, given many women find the diagnosis and initial management of GDM stressful as they adapt to more regimented dietary choices and regular glucose monitoring. Further, a diagnosis of GDM provides a critical opportunity to highlight women at risk of future diabetes, enabling GPs to engage in targeted monitoring and early lifestyle interventions in the postpartum period to reduce not only maternal risk, but also potentially lower their offspring’s future risk of obesity and abnormal glucose tolerance. MT
{kind=link}
{kind=link}