Diagnostic approach to thyroid nodules

Thyroid nodules are a common finding in clinical and radiological (mainly ultrasonographic) examinations. Although most are benign, a small percentage of thyroid nodules have the potential to become malignant or are malignant. This article aims to assist GPs with the evaluation of thyroid nodules and providing timely referral when appropriate.
Thyroid nodules are radiologically distinct lesions within the thyroid parenchyma. They are palpable in 4 to 7% of the population during routine physical examination and detected in up to 67% through high-resolution ultrasonography.1,2 Thyroid nodules are clinically relevant, as about 4 to 6.5% of nodules are malignant and are associated with significant morbidity when the diagnosis is missed.1,3 Furthermore, the high prevalence of thyroid nodules has led to excessive investigations, leading to significant economic burden on the healthcare system. This article aims to assist GPs in developing a diagnostic approach for evaluating thyroid nodules by determining the probability of a malignant nodule, developing a management plan and making timely referrals.
Initial evaluation of thyroid nodules
The presentation of thyroid nodules is diverse. They may be noticed by patients themselves, or detected by the GP during routine physical examination or through imaging modalities such as neck ultrasonography, computed tomography or positron emission tomography scanning while investigating for unrelated conditions. Nonpalpable nodules, or incidentalomas, have the same risk of malignancy as palpable nodules of the same size;4,5 however, the clinical course of papillary microcarcinoma, which often is identified incidentally, is usually very indolent.
History and physical examination
A detailed history and physical examination are vital in forming a risk assessment of a thyroid nodule. Symptoms of upper airway compression, such as dyspnoea, dysphonia, dysphagia or globus pharyngeus should raise suspicion of an underlying malignancy, although these features are reflective of late-stage presentations, owing to invasion, or large benign tumours having locoregional compressive effects. Other features of the history may also suggest an increased likelihood of malignancy. These include rapid growth of a neck mass, childhood head and neck irradiation, a family history of thyroid cancer, or syndromes associated with thyroid cancers including multiple endocrine neoplasia type 2, familial adenomatous polyposis, Cowden syndrome or Gardner syndrome.1 Physical examination findings of a fixed, hard neck mass or ipsilateral cervical lymphadenopathy are suspicious of malignancy.
Blood tests
Serum thyroid stimulating hormone (TSH) levels should be assessed in all patients presenting with thyroid nodules. If the TSH level is suppressed (defined as <0.1 mU/L) the nodule is likely to be hyperfunctioning and has a very low risk of malignancy.1 If TSH is suppressed, then free thyroxine (FT4) and free triiodothyronine (FT3) should be measured, if not already done, alongside thyroid scintigraphy and referral to an endocrinologist.
The use of serum calcitonin level in evaluation of thyroid nodules is controversial. The American Thyroid Association (ATA) guidelines note the uncertainties surrounding calcitonin measurements and have not taken a stance for or against calcitonin screening.1 However, there may be a role for calcitonin screening when there is suspicion of medullary thyroid carcinoma.6,7 Serum thyroglobulin level should not be requested for the evaluation of thyroid nodules, as it is neither sensitive nor specific for diagnosis of malignancy.1
Thyroid ultrasonography
Thyroid ultrasound should be performed in all patients when there is clinical suspicion of a thyroid nodule, a palpable neck nodule on physical examination or an incidental finding of thyroid nodules on other imaging modalities (including carotid ultrasound, CT or MRI scans). High-resolution ultrasound machines are highly sensitive and are able to detect nodules as small as 1 to 3 mm.
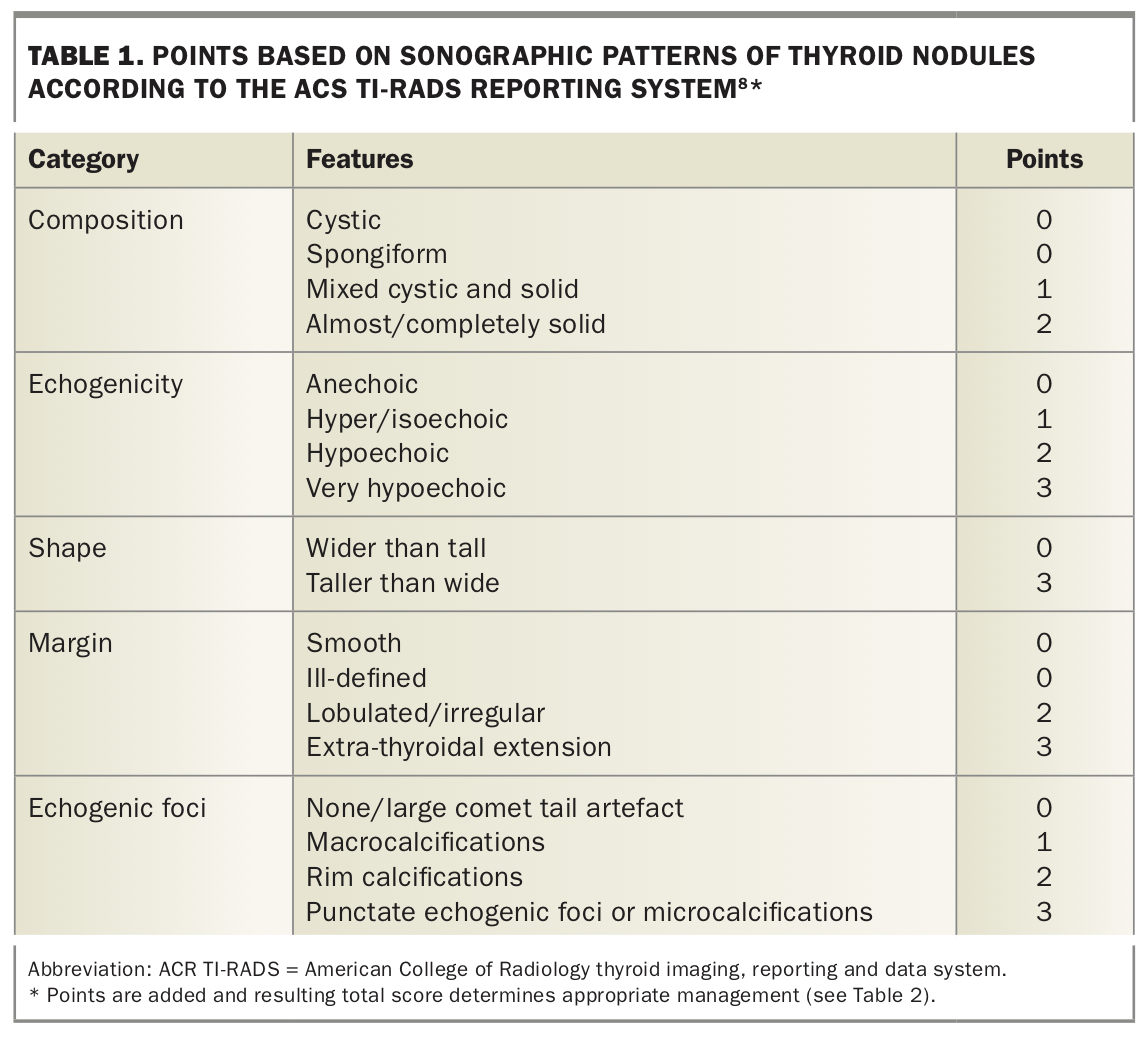
Thyroid ultrasound provides assessment about the size and sonographic features of the nodules and adjacent structures in the neck, forming the basis of risk stratification and guidance for fine needle aspiration (FNA). Based on the American College of Radiology thyroid imaging, reporting and data system (ACR TI-RADS) guidelines, which are widely adopted by Australian radiologists, thyroid nodules are scored and categorised into five groups based on the sonographic pattern to provide an estimate of the malignancy risk.8 This is supported by the fact that there is increasing evidence that the presence of suspicious ultrasound features is more predictive of malignancy than nodule size alone. Given that ultrasonographic reports do not consistently contain risk stratification of nodules, it is important for GPs to be aware of features that are suspicious of an underlying thyroid malignancy. These include solid composition, hypoechoism, microcalcifications, irregular margins, a taller-than-wide shape (with greater anteroposterior diameter) and extra-thyroidal extension (Table 1).
{kind=link}
Subsequent evaluation of thyroid nodules
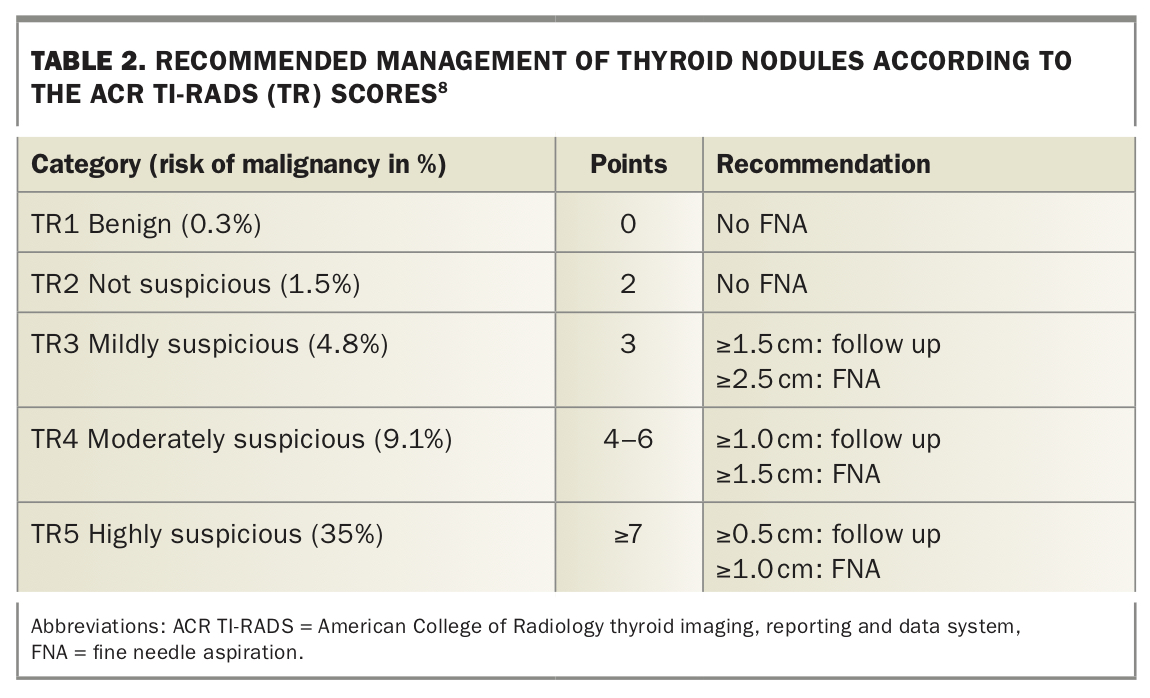
Subsequent evaluation of thyroid nodules is dependent on the patient’s TSH level and ultrasonographic features of the nodule, which would be guided by the ACR TI-RADS grade of the nodule(s) (Table 2 and Flowchart 1). In cases of low TSH levels, thyroid scintigraphy should be ordered, and referral to an endocrinologist should be considered.1
{kind=link}
Thyroid scintigraphy
Thyroid scintigraphy is a radionuclide test that uses iodine-123 or technetium-99m pertechnetate to determine the functional status of a nodule. Hyperfunctioning (or hot) nodules, which absorb larger amounts of radionuclide compared with normal thyroid tissue, often do not warrant FNA as these are very rarely malignant. Hypofunctional (or cold) nodules, which conversely absorb lower amounts of radionuclide compared with normal thyroid tissue, may require evaluation by FNA.10 However, it should be remembered that thyroid scintigraphy is an adjunct investigation in cases of TSH abnormality, which itself suggests that nodules may be metabolically active and hence amenable to nonsurgical management. The decision to perform FNA, therefore, would largely be guided by radiological features on thyroid ultrasound. Additionally, scintigraphy may be useful in patients with multiple thyroid nodules to determine hypofunctional nodules that may require FNA.9 This test is contraindicated during pregnancy. According to the Australian Radiation Protection and Nuclear Safety Agency 2008 Guidelines, if scintigraphy using technetium is performed in a woman who is breastfeeding, she should stop breastfeeding for 26 hours after the injection with the tracer and breastmilk should be regularly expressed and discarded during this time.11
In cases of normal or high TSH levels and thyroid nodules with suspicious ultrasonographic features, an FNA biopsy is the next step in evaluating thyroid nodules and identifying patients who may require surgical resection.1 Patients with high TSH levels should be evaluated for hypothyroidism, and nodules that do not have suspicious ultrasonographic features warranting FNA should be monitored.
Fine needle aspiration biopsy
FNA is a valuable tool in the evaluation of thyroid nodules with suspicious ultrasonographic features and has been instrumental in reducing the number of unnecessary thyroidectomies. The diagnostic accuracy of FNA biopsies is about 95% when done by an experienced proceduralist. All cytology results are reported using the Australian Modified Bethesda classification system for thyroid nodules, which will then provide an estimate of malignancy risk and recommendation for management.12,13 If a patient has multiple nodules, ultrasonographic features of each nodule should be assessed independently to determine the need for FNA. If there are multiple nodules, the two with the highest ACR TI-RADS scores should be sampled, rather than the two largest.8
Management
The primary goal for GPs in evaluating thyroid nodules is to distinguish between benign and malignant nodules. FNA results according to the Bethesda classification play an important role in determining the most appropriate management and follow up (Flowchart 2).
Patients with thyroid nodules that do not have suspicious ultrasonographic features and who do not undergo a biopsy should be monitored with repeat ultrasounds at differing intervals depending on the individual nodule features as defined by the 2017 TI-RADS (TR) guidelines:
- TR1 nodules: no follow-up ultrasound required
- TR2 nodules: no follow-up ultrasound required unless any clinical concern
- TR3 nodules: follow-up ultrasound in one, three and five years
- TR4 nodules: follow-up ultrasound in one, two, three and five years
- TR5 nodules: annual follow-up for five years.
Surveillance imaging of nonbiopsied nodules can be stopped after five years if there is no change in size, as stability over that time span reliably indicates that a nodule has a benign behaviour.14 If a nodule’s ACR TI-RADS category increases on follow-up and does not meet the FNA recommendations, the next surveillance ultrasound should be done in one year.
Most nodules biopsied through FNA have benign cytology and are similarly monitored with repeat thyroid ultrasound at differing intervals (Flowchart 2). Patients with a nondiagnostic result should have a repeat ultrasound-guided FNA and be referred to a high-volume thyroid surgeon or endocrinologist.1
Otherwise, patients with all other cytology results according to the Bethesda classification should be referred for further assessment and management. Any patients with suspected or confirmed malignancy should be referred to a high-volume thyroid surgeon for surgical intervention. Management of thyroid nodules of indeterminate ultrasonographic features and/or cytology is often complex and such cases should be referred to an endocrinologist, as many have experience in interpreting and performing thyroid ultrasound and FNA in patients with this particular diagnosis.1
Managing paediatric patients
Paediatric patients who present with thyroid nodules should ideally be managed in multidisciplinary settings, including paediatricians, thyroid surgeons and possibly clinical geneticists. Evaluation of paediatric thyroid nodules is similar to evaluation of nodules in adults, although with a few important distinctions according to the 2015 ATA guidelines.1 FNA should be considered based on clinical history, examination and sonographic features rather than nodule size. If FNA is required, a general anaesthetic may be indicated, depending on the age of the child. Furthermore, FNA result of indeterminate cytology should be referred to a high-volume thyroid surgeon for hemithyroidectomy instead of a repeat FNA. This is largely because the overall thyroid malignancy rate in children is noted to be about 26%, compared with 4 to 6.5% in adults.15
Conclusion
Thyroid nodules are common presentations encountered in general practice. Serum TSH level and thyroid ultrasound should be the initial investigations done by GPs. FNA biopsy is performed according to the risk of malignancy seen on thyroid ultrasound, with thyroid scintigraphy reserved for patients with suppressed serum TSH levels. Most thyroid nodules are benign and can be monitored at regular intervals. Suspected or confirmed malignancies from FNA biopsy should be referred to a high-volume thyroid surgeon, whereas indeterminate ultrasonographic or cytological findings should be referred to an endocrinologist, as management of these nodules can be complex. MT
COMPETING INTERESTS: None.