Treating alcohol dependence: managing withdrawal and preventing relapse

Alcohol
One in 25 adults in Australia becomes dependent on alcohol at some stage. GPs play a key role in earlier detection of alcohol dependence and can provide treatment for withdrawal (where safe to do so), relapse-prevention medicines and support.
- GPs are the first point of contact with the health system for most problem drinkers.
- GPs can provide earlier detection of problem drinking and deliver brief interventions to raise motivation for change.
- Many alcohol-dependent people can safely undergo withdrawal from alcohol at home, supervised by their GP with daily-dispensed diazepam.
- Medications such as naltrexone, acamprosate and disulfiram can be prescribed by the GP after withdrawal is complete to reduce cravings for alcohol and prevent relapse.
- Relapse-prevention medicines can be combined with individual or group relapse-prevention approaches.
- A small number of alcohol-dependent people will require (or accept) referral to an addiction specialist or to inpatient detoxification services.
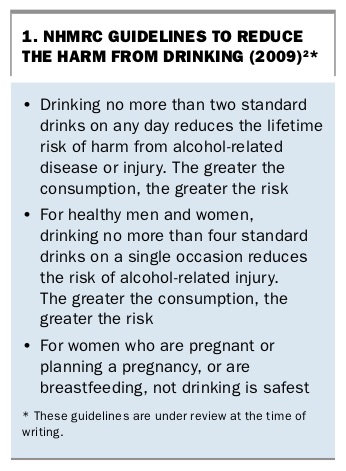
Around the world, alcohol is the leading cause of loss of healthy life-years for people aged 15 to 49 years.1 Although many of the harms of alcohol occur in nondependent drinkers, dependence on alcohol can have severe short-term and long-term effects on physical and mental health. It also affects family and the community. Many people drink at risky levels episodically, for example on a Saturday night or at football grand finals. Some may drink 15 to 20 standard drinks at these times. Those who drink more than four standard drinks on an occasion are at increased risk of acute harms such as injury. Others regularly exceed recommended limits, sometimes most days of the week (Box 1).2 Any regular use of alcohol of more than two small drinks per day increases the risk of long-term harms from alcohol, such as hypertension and cancer (e.g. breast or colon cancer).
{kind=link}
The harms multiply when a person is dependent on alcohol. One in 25 Australian adults becomes dependent on alcohol at some time in their life, therefore every GP needs to be comfortable with its prevention and management.3 In its most severe form, alcohol dependence can behave like a chronic disease, with remissions and relapses. Knowledge of treatment of alcohol dependence has advanced greatly in the past 20 years. Multiple randomised controlled trials have shown that treatment can make a difference to outcomes.4-6 The earlier that treatment is offered, the better the prognosis.
This article reviews what a GP can do to prevent and treat alcohol dependence. This includes screening and brief intervention, outpatient withdrawal management and prescribing medicines to support relapse prevention. Many patients who drink alcohol at unhealthy levels will not attend a specialist alcohol and drug service, so their GP may be the best-placed health professional to offer assistance.
Patients who ask for help or are detected by screening
There is a continuum between low-risk drinking and dependent drinking. People can slip into hazardous, harmful or dependent drinking without realising they have done so. Others may know they are having difficulties with their drinking but may be ashamed to ask for help or not know that their GP can offer assistance.
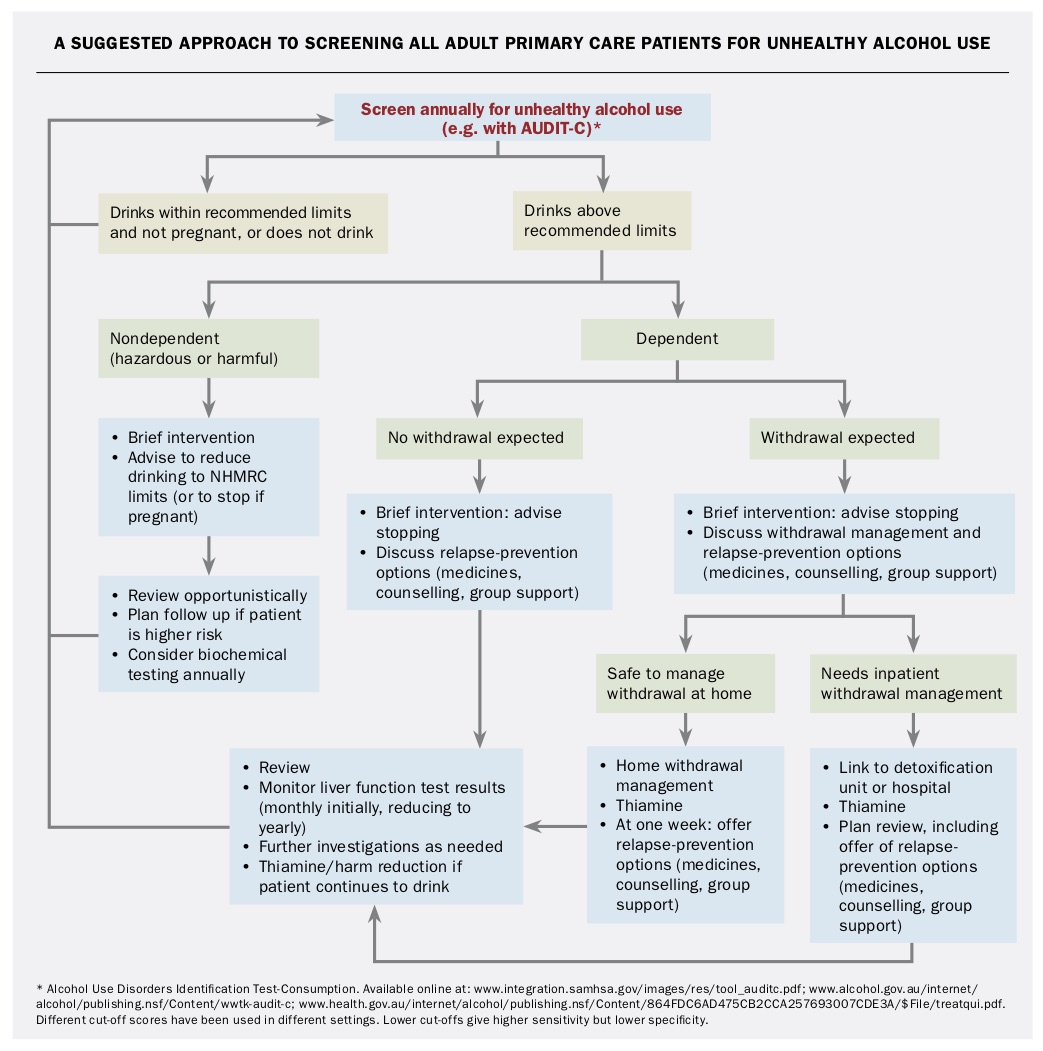
Unfortunately, drinking problems are highly stigmatised in Australia. On average, people with alcohol dependence have symptoms for 18 years before accessing help.7 The GP can lessen this delay by diagnosing alcohol dependence early and initiating treatment promptly. Alcohol use should be assessed in every adult patient as part of preventive health care, and also when presentations may be alcohol related, such as in cases of hypertension, insomnia, mental health conditions, abnormalities in liver enzyme or triglyceride levels, injuries or family violence (Flowchart).
{kind=link}
When is a drinker dependent?
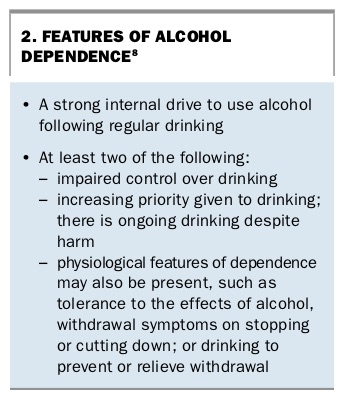
Some people drink regularly at risky levels (not necessarily every day) and start to find that drinking is no longer fully under their control. They may develop a strong internal drive to drink, and may have physiological features of tolerance and/or withdrawal. Alcohol may start to take an increasingly high priority in their life (Box 2).5,8
{kind=link}
A person who is finding it difficult to control their drinking may plan not to drink but find that they still do so. They may plan to stop at one or two drinks but find themself continuing until all the alcohol has gone. Some (but not all) of these drinkers may experience withdrawal symptoms such as insomnia and tremors when they stop drinking or cut down.
Alcohol intake is determined by a mix of genetics and environment (50:50).9 Identified risk factors for unhealthy drinking include a thrill-seeking personality, any mental illness and the genetics of a person’s reward centre (e.g. dopamine or opioid receptors). Occupations with easy access to alcohol may increase risk.
Investigations
Brief intervention should be offered by the GP at the time unhealthy drinking is discovered, rather than waiting for investigation results, as the patient may not return. Measurement of liver enzyme, electrolyte, urea and creatinine levels are useful, as well as a full blood examination and INR. Up to 70% of people who drink six or more drinks per day have normal blood test results.10 Normal blood test results do not rule out alcohol dependence or end organ damage, but a baseline test is useful. Evidence of elevated liver enzyme levels can be helpful in raising a patient’s motivation to stop drinking, and results that decrease with alcohol cessation provide valuable positive feedback. If a patient’s liver enzyme levels are markedly deranged, their INR is raised or they have severe or longstanding alcohol dependence, consider ultrasound and/or FibroScan (transient elastography). If results are consistent with cirrhosis, consider referral to a hepatologist, and an alpha fetoprotein level and a triple-phase CT scan to exclude hepatocellular carcinoma.
Brief interventions for unhealthy drinking
For people who drink at hazardous or harmful levels who are not dependent on alcohol, a simple brief intervention is usually all that is required. For those who are dependent, brief intervention can be used to build motivation and help engage the person with further treatment.
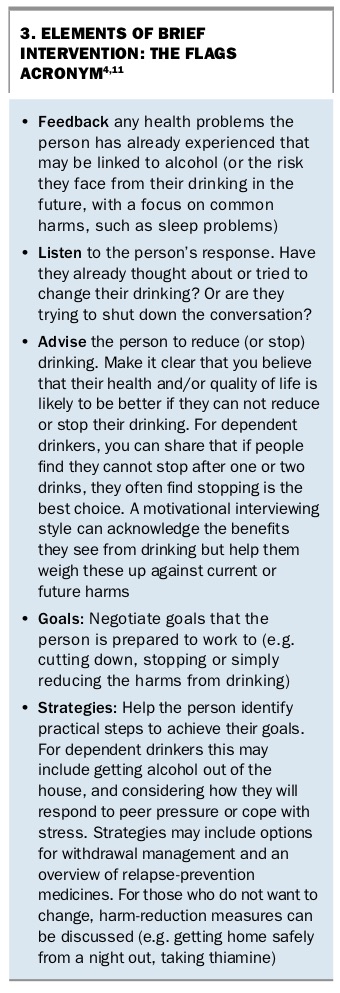
A brief intervention is simply a five- to 20-minute conversation about drinking alcohol that typically has elements summarised by the acronym FLAGS: feedback, listening, advice, goal setting and strategies (Box 3).4,11 It aims to engage the patient and help motivate them to change their drinking, and find ways to do so.
{kind=link}
Treatment for dependence
Because of the strong internal drive to drink associated with dependence, stopping drinking often becomes the only way to regain control. Individuals who are dependent on alcohol may need support to change and may benefit from medicines to help them stop and to stay abstinent.
Who needs withdrawal management?
Sweats, tremor (‘grog shakes’) or insomnia for the first few days after a person stops drinking are likely to reflect alcohol withdrawal. An alcohol-dependent person who has never stopped drinking for any length of time may notice a slight tremor or stress that settles with the first drink of the day.
For regular, heavy drinkers who experience severe withdrawal symptoms, stopping alcohol suddenly without appropriate medication can be dangerous and sometimes life-threatening. This is particularly the case for people who have had seizures or delirium during alcohol withdrawal. Ensuring early treatment of withdrawal can reduce its risks and increase completion rates. If a complicated withdrawal is expected, inpatient treatment is the safest option.
Management of withdrawal
For many people who experience simple alcohol withdrawal (without seizures or delirium) and who are relatively healthy, withdrawal can be managed at home (‘home detox’), provided the patient:
- is sensible and motivated
- has a suitable supported environment (not surrounded by other problem drinkers; no violence)
- does not have a history of benzodiazepine misuse
- does not have a current other substance-use disorder (except nicotine and perhaps cannabis use)
- does not have a history of seizures, as alcohol withdrawal lowers the seizure threshold
- does not have a history of complicated withdrawals (e.g. seizures, delirium)
- does not have unstable liver disease or unstable medical conditions such as type 1 diabetes.4,5
Maximising safety of home withdrawal
The safety of patients undergoing withdrawal at home can be optimised by the following:
- Careful patient selection. If people do not meet the above criteria for withdrawal at home, they are best to seek inpatient or residential withdrawal management
- Daily dispensing of diazepam. This can be done via a pharmacist or practice nurse (e.g. the week’s medicines are put into a Webster pack, stored at the practice and the appropriate strip is dispensed daily by a nurse). A person who presents intoxicated should not receive any diazepam
- Advice to avoid driving and using machinery while on diazepam or while in marked withdrawal.
Dependent drinkers who are unsuitable for a primary care supervised home detoxification could be referred to an addiction specialist or for detoxification in hospital.
A suggested patient handout is provided on page 33.
Treatment regimens for withdrawal management
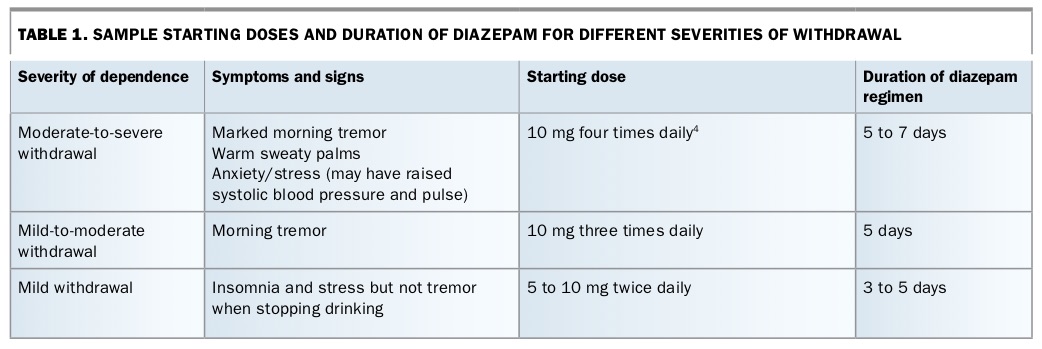
The starting dose of diazepam can be adjusted to fit the expected severity of withdrawal. Severity is assessed based on the person’s past experience of withdrawal (Table 1); or, for a person who has never stopped drinking, based on symptoms before the first drink of the day. Diazepam is then weaned to nothing within a week. This is important to avoid the risk of creating benzodiazepine dependence.
{kind=link}
When possible, the person is checked daily (e.g. by a practice nurse using an alcohol withdrawal scale).5 If tremor, insomnia, agitation, raised pulse and blood pressure are not controlled by diazepam a dose increase may be needed. However, it is important to keep in mind the possibility of concurrent diagnoses (e.g. cerebellar tremor, chest infection). If the withdrawal fails to come under control, referral to hospital is indicated.
It is often convenient to begin a home detoxification on a Monday to ensure help from a health professional is available. Dependent drinkers could be advised to try to slightly reduce levels until the detoxification can commence. Marked reductions should be avoided if the person has a history of seizures.
With moderate-to-severe withdrawal, symptoms tend to be worse in the first 48 hours, so dose reduction can start on day three (e.g. changing from 10 mg four times daily to 10 mg three times daily, then each day 10 mg can be reduced from the dose).
Before and during withdrawal it is good to discuss with the patient what steps they will take to help them stay ‘dry’ afterwards. This can include removing alcohol from the home, avoiding friends who drink alcohol, keeping busy and planning treats that do not include alcohol. Relapse-prevention medicines may be commenced at the end of the withdrawal syndrome (at about one week). Patients can be offered counselling or group support, when available.
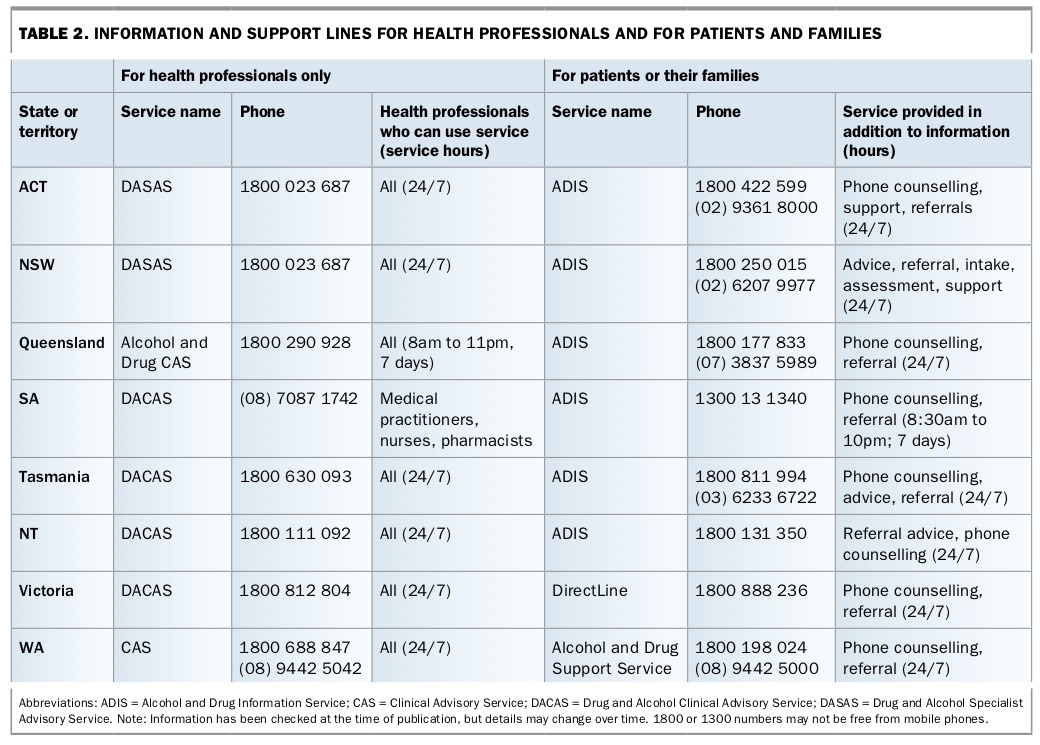
If a person has severe and refractory dependence or a very difficult living environment, they can consider live-in rehabilitation programs. Many such programs require withdrawal from alcohol before admission. The client can find programs via the Alcohol and Drug Information Service (Table 2).
{kind=link}
Relapse prevention
In Australia three medicines are approved for use in relapse prevention in alcohol- dependent people: acamprosate, naltrexone and disulfiram. Only acamprosate and naltrexone are on the PBS. None of these medicines are addictive and all can be prescribed by a GP. However, none can be used in pregnancy. Disulfiram is associated with greater risks, so prescribing guidelines should be read carefully and advice sought if there is still uncertainty regarding its use. Advice on prescribing these medicines can usually be obtained through a regional drug and alcohol specialist phone advisory service. Such services exist around Australia (Table 2).
If one relapse-prevention medicine is not effective, another can be trialled or two or more medicines may be combined. As each works via a different mechanism, acamprosate and naltrexone can be readily combined.
Relapse risk is highest in the first three months after withdrawal. Medicines are usually continued for three months, but if the patient perceives they are helpful they can be continued for as long as desired.
Other medicines have been trialled as relapse-prevention agents (e.g. baclofen, topiramate), but any use for alcohol dependence is off label, and each has associated risks. We recommend specialist advice before using these medicines for alcohol dependence. Long-term diazepam is ineffective and hazardous as a treatment for alcohol dependence. Antidepressants are ineffective as a treatment for alcohol dependence.
Support, counselling and groups
None of the relapse-prevention medicines are magic bullets and none replace the need for the patient to make a strong effort and to receive support and, when available, skilled, practical counselling. Such counselling may be available through local drug and alcohol counsellors, psychologists with an interest in addiction and psychiatrists. Initially counselling typically focuses on practical ways to avoid drinking and to deal with cravings or risk situations, and to maintain motivation.
A Mental Health Treatment Plan helps with affordability of private counselling. In some parts of the country, there are free groups to support change and there are also web resources to support change (Box 4). If a patient’s whole life has revolved around alcohol, helping them think about alternative activities or social networks is valuable.
{kind=link}
Acamprosate
Acamprosate is easy to prescribe. The main contraindication is renal failure. It has few drug interactions. Most patients feel completely normal while taking acamprosate. Craving for alcohol is reduced if it is effective. Some patients taking acamprosate have self-limited diarrhoea or rash.
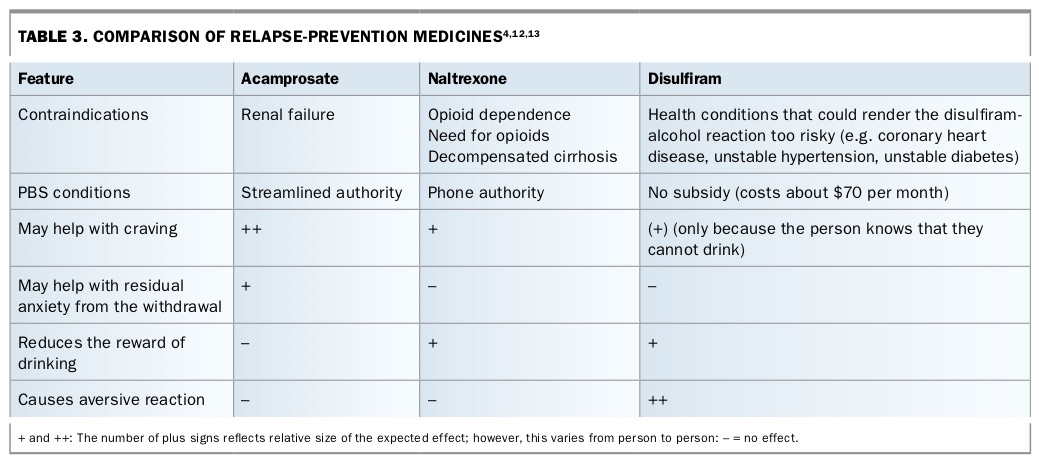
Acamprosate works by partially reversing the neuroadaptation to alcohol. It seems to reduce overactivity at the N-methyl-D-aspartate receptor. There are no clear evidence-based guidelines on which medicine to choose for which patient, but clinical experience suggests that acamprosate may be better for those who have significant neuroadaptation, such as those who experience marked withdrawal symptoms (Table 3).4,12,13
{kind=link}
Acamprosate can be started as soon as diazepam for withdrawal management is ceased. It can take up to two weeks to reach its maximal effect. One drawback of acamprosate is that the dosage is two tablets three times daily (with lunchtime and evening doses reduced to one tablet in people weighing less than 60kg). The three times daily dosing may be more difficult to remember. Acamprosate is available under a PBS streamlined authority.
Naltrexone
Naltrexone appears to work by blocking the ‘reward’ or ‘feel good’ effect of alcohol. Alcohol indirectly acts on opioid receptors, and naltrexone blocks that action. If a person slips up and has a drink, this blocking effect may make it easier for them to stop.
Naltrexone has advantages because it is given as one tablet per day. Clinical experience suggests that it can also be useful for drinkers for whom the enjoyment of drinking (rather than withdrawal relief) is a strong driver. If a person says they want to stop but appears ambivalent, naltrexone may reduce the ‘pull’ of alcohol. Naltrexone can also be a good choice for episodic heavy drinkers, who are dependent but may not drink every day and may have little or no withdrawal symptoms. The genetics of the person’s reward centre may influence whether or not naltrexone will work well, but there is no practical way to test this in advance.
The chief contraindication to naltrexone is chronic opioid use or the need to take opioids for pain. Naltrexone can precipitate severe opioid withdrawal. There is a rare risk of increased liver enzyme levels from naltrexone. But this risk has to be balanced against the common risk of alcohol causing liver problems. If a person has decompensated cirrhosis (jaundice, ascites) naltrexone should be avoided.
It is important to advise patients that naltrexone blocks strong painkillers. If surgery is planned, they need to stop taking naltrexone at least 48 hours in advance. If emergency analgesia is needed, high-dose opioids or nonopioid alternatives such as nerve block or ketamine may be required.
Most people feel normal on naltrexone. Some experience nausea soon after starting treatment. For that reason, it can be helpful to start on half a tablet (25mg) for a day or two, before increasing to a full tablet (50mg) daily.
The person can start on naltrexone at any time, but typically it is commenced when the withdrawal is almost finished. One reason for this is that alcohol withdrawal can cause nausea, and naltrexone may exacerbate this. There has been limited research trialling the use of naltrexone while someone is still drinking. Such an approach should be avoided in people who have seizures, as alcohol reduction could trigger a seizure.
Naltrexone is available under the PBS, under authority. Like acamprosate, the requirement of the subsidy is treatment of alcohol dependence with a goal of abstinence.
Disulfiram
Disulfiram has been used in relapse prevention for many decades, but is not subsidised under the PBS so is more expensive for the patient than acamprosate and naltrexone. Sometimes supply can be limited, and the patient may need to access a compounding pharmacy. Disulfiram inhibits aldehyde dehydrogenase, leading to acetaldehyde accumulation after drinking alcohol. Acetaldehyde is associated with many unpleasant symptoms.
After only a sip or two of alcohol, the person taking disulfiram typically experiences headaches, palpitations, flushing, nausea, vomiting and low blood pressure.12 The reaction can be severe enough to result in hospitalisation. Because of the severity of this reaction, the risks and potential benefits of disulfiram need to be carefully weighed up. It is typically reserved for situations when the person has had so many adverse effects from alcohol that they risk losing their job or spouse, or ending up in prison; or when all other treatments have failed and dependence is severe. The patient needs careful education to avoid medicines or foods that might contain alcohol.
Disulfiram works best when the patient asks someone (typically a family member) to observe the daily dose. If no one else is available, a pharmacist may be recruited to do this. As disulfiram does not directly reduce craving, this support and supervision is important; without it, the success rate is low. Disulfiram cannot be started until 72 hours after the last drink, because alcohol is metabolised at an average rate of one standard drink per hour.
Thiamine
All dependent drinkers should be advised to take thiamine at a dose of at least 100mg daily to prevent Wernicke’s encephalopathy. Once the person stops drinking, they can continue on a 100mg tablet daily for one month, then stop. Thiamine is subsidised under the PBS for Aboriginal and Torres Strait Islander patients. If there are signs of poor nutrition, consider giving parenteral thiamine immediately (e.g. 100mg intramuscularly). Acute onset of confusion, ataxia or eye signs such as nystagmus (when sober) or paralysis of lateral gaze could be Wernicke’s encephalopathy. This is a medical emergency, requiring prompt IV thiamine.
Treatment of concurrent anxiety and/or depression
Concurrent anxiety and/or depression is common with alcohol dependence. Most mood disorders improve when the person stops drinking, so unless the depression is severe, medical treatment of depression is usually deferred for a month after alcohol cessation. If an antidepressant is required, choose one that is less likely to cause anxiety as a side effect (e.g. mirtazapine). Mental Health Care Plans can be used to refer patients to psychologists for alcohol-relapse prevention (including motivational interviewing and specific relapse-prevention techniques) and for comorbid mental health conditions.
Rural and remote settings
Sometimes the nearest residential detoxification or rehabilitation service may be many hours’ drive away, and the person seeking treatment may go into withdrawal en route.
Home detoxification can be conducted in remote areas, and telehealth services can be used to refer patients for consultations with addiction specialists. Contacts are listed on the Australian College of Rural and Remote Medicine Telehealth Provider Directory (www.ehealth.acrrm.org.au/provider-directory?term=&type%5Bconsultant%5D=consultant). Advice is also available through drug and alcohol clinical/specialist advisory services.
When possible, any patient with a history of seizures should have withdrawal managed as an inpatient. If this is not possible, early initiation of diazepam (typically 10mg four times daily) helps prevent seizures. Diazepam can be started when the person is no longer intoxicated but before withdrawal symptoms start, as withdrawal seizure can precede tremor. Patients whose withdrawal is expected to be complicated (e.g. those with unstable epilepsy) are best transferred for supervised detoxification in hospital.
Conclusion
Many dependent drinkers are reluctant to seek help or a specialist alcohol treatment service. The GP plays a key role in earlier detection, building motivation for change and increasing access to treatment for dependence. Alcohol withdrawal can be managed by GPs in carefully selected cases and specialist support is available from phone advisory services. Relapse- prevention medicines can be prescribed by GPs and improve prognosis in alcohol dependence. They can be combined with individual or group support or behavioural treatments. MT