Common and important skin rashes in primary care

Dr Blake is a Dermatology Research Fellow at St George Dermatology and Skin Cancer Centre, Sydney. Associate Professor Shumack is a Clinical Associate Professor at the Sydney Medical School (Northern), The University of Sydney, Sydney; and a Staff Specialist Dermatologist at Royal North Shore Hospital, Sydney, NSW.
Skin conditions
Many of the common and serious presentations to primary care that are related to dermatology are listed here. GPs need up-to-date information to help with initial investigation and management strategies, and recommendations for when to refer on.
- Patients with skin problems comprise 17% of general practice consultations in Australia.
- Patients can present to primary care with skin problems ranging from autoimmune and inflammatory conditions to dermatological emergencies.
- Autoimmune and inflammatory problems include dermatitis, psoriasis and acne.
- Infectious diseases such as tinea, cellulitis and scabies are also common.
- Occasionally, patients may present with dermatological emergencies such as Stevens-Johnson syndrome and toxic epidermal necrolysis.
- It is important that GPs are aware how to diagnose and manage these conditions, and know when to refer patients.
Dermatological presentations represent a large proportion of all general practice consultations in Australia, with the 2015-2016 BEACH General Practice Activity study finding that 17 out of 100 consultations are related to skin problems.1 Contact dermatitis, skin neoplasms, skin checks and acne were among the top five reasons for referral to a dermatologist.1
Autoimmune and inflammatory skin conditions
Atopic dermatitis
Atopic dermatitis, otherwise known as eczema, is one of the most common dermatological conditions – affecting up to 30% of one-year-olds in Western countries (Figure 1).2 The incidence declines with age, but this condition still affects about 2 to 5% of adults.3 Quality of life in patients with atopic dermatitis and their families is significantly affected, particularly their mental health and social functioning.4,5 The pathogenesis of atopic dermatitis is not yet fully understood, but involves a complex interplay of genetic factors, environmental triggers, skin barrier dysfunction and the skin microbiome.
{kind=link}
Nonpharmacological measures are key in the management of atopic dermatitis and should be initiated in all patients. Patients should use a bland emollient regularly and liberally. Clinicians should also advise patients to use soap-free washes, have shorter, cooler showers and consider bleach baths in patients with recurrent superficial Staphylococcus aureus infections.
Topical corticosteroids are the cornerstone of therapy and should be used at appropriate strengths for appropriate sites. Weaker strengths should be used in areas prone to possible adverse reactions (the face, axillae and groin). The most commonly used corticosteroid is hydrocortisone 1% cream or ointment. In other areas of the body, a moderate- to high-potency topical corticosteroid is appropriate – for example, betamethasone dipropionate 0.01% ointment. Corticosteroid phobia is common among patients and their families, and can often result in treatment failure.6 Ongoing strong reassurance from trusted clinicians can assist in combating this and optimising adherence.
In patients for whom topical corticosteroid therapy and optimisation of their general skin care routine is ineffective, referral to a dermatologist should be considered. Other options that may be prescribed by a dermatologist for patients with moderate to severe eczema include narrow-band ultraviolet (UV) B therapy and oral immunosuppressant therapy with medications such as methotrexate, ciclosporin, mycophenolate mofetil and azathioprine. Initially, all oral immunosuppressant therapies require close monitoring of clinical response and laboratory parameters. However, once a patient is stable on a particular medication, shared care with the GP may be appropriate. Occasionally, courses of oral corticosteroids can be useful in the management of flares. However, prolonged use should be avoided due to their significant side effects and difficulty in stopping the corticosteroids in some patients.
Dupilumab is a potential upcoming biologic therapy for atopic dermatitis, and has been approved by the US Food and Drug Administration and the TGA. It is a monoclonal antibody directed against the IL-4 receptor and, in Phase III trials, about two-thirds of patients demonstrated a 75% reduction in Eczema Area and Severity Index score at one year, with a reduction in flare frequency.7 It is not yet available on the PBS in Australia but is available through private prescription from dermatologists and immunologists. Dupilumab is associated with an increased risk of infections, particularly upper respiratory tract infections and conjunctivitis.
Other promising potential therapeutic options in the future include Janus kinase (JAK) inhibitors and interleukin (IL)-31 and IL-23 antagonists. Oral JAK inhibitors also carry an increased risk for infection, and can cause hyperlipidaemia and lymphopenia.
Psoriasis
Psoriasis is an immune-mediated inflammatory skin condition, in which unknown environmental stimuli cause the release of cytokines, causing the skin cells to rapidly divide (Figure 2). There are a number of subtypes of psoriasis including chronic plaque, guttate, palmoplantar, pustular, flexural, nail, scalp and erythrodermic. The most common of these is chronic plaque psoriasis (CPP), although patients can experience multiple subtypes concurrently.
{kind=link}
Patients usually develop CPP in adulthood, before the age of 45 years. Once affected, they rarely experience spontaneous remission, and will usually require lifelong treatment. In Australia, CPP affects about 2 to 6% of the population, and it is estimated that 19,000 Australians are living with a severe form of the disease.8,9
Guttate psoriasis is classically associated with a preceding streptococcal infection, and typically affects younger patients. It is characterised by smaller, teardrop-shaped plaques, with a generalised distribution, and usually clears spontaneously after a few months. Palmoplantar psoriasis affects the acral surfaces, and the classic plaques of psoriasis are often seen, with patchy or generalised keratoderma.
Scalp psoriasis has the same features as CPP, with erythema, scale and thickened skin across the scalp and hairline. It can be associated with hair loss in severe cases, but does not cause scarring alopecia, and hair usually regrows once the underlying disease is treated. Patients may have nail psoriasis in conjunction with other subtypes, or on its own. Characteristic features include nail plate crumbling, pitting, onycholysis and splinter haemorrhages.
Flexural or inverse psoriasis affects the axillae and groin, and usually does not have the thickening or scale associated with chronic plaque. These patients have erythematous patches in the flexural areas, which can mimic erythrasma or other infectious conditions.
Pustular psoriasis and erythrodermic psoriasis are two severe subtypes that require urgent specialist review and are usually managed in the inpatient setting. Pustular psoriasis presents with small pustules, usually on the hands and feet, but occasionally on the body. These pustules are sterile when swabbed, and can occur in discrete patches or in a generalised distribution. The generalised presentation can progress to erythrodermic psoriasis, which can be life threatening. It is often precipitated by withdrawal of corticosteroids in psoriasis patients, drugs such as lithium and antimalarials, or infection. Due to the disruption of the skin barrier, these patients are prone to dehydration, hypothermia and high-output cardiac failure. It requires aggressive treatment with topical wet wrap therapy, intravenous fluid and electrolyte replacement, and consideration of oral immunosuppressive therapy such as ciclosporin or acitretin, and patients are typically managed in an inpatient setting.
Psoriasis has a significant impact on quality of life and increases patients’ risk of inflammatory arthritis, inflammatory bowel disease, cardiovascular disease, metabolic syndrome and lymphoma.10-12
Modification of lifestyle factors, such as optimisation of weight and blood sugar, increased exercise and smoking cessation can be useful in reducing disease activity.13-15 First-line therapy for psoriasis includes topical corticosteroids, which can be combined with vitamin D analogues to better penetrate the thick, scaly plaques. Ready-made preparations include calcipotriol and betamethasone dipropionate as foam, gel or ointment. Patients who have resistant disease can be referred to a dermatologist to trial UV light therapy or oral immunosuppressives such as methotrexate, ciclosporin and acitretin. In severe and resistant disease, biologics such as TNF-α, IL-17 and IL-23 inhibitors can be useful. These agents have an excellent success rate, with 65 to 70% of patients with moderate to severe psoriasis who use IL-23 antagonists achieving almost clear or clean skin.16 These new biologics are well tolerated, with the most common side effects being increased risk of upper respiratory tract and cutaneous infections.
Alopecia areata
Alopecia areata (AA) is a nonscarring autoimmune form of hair loss and the lifetime prevalence is estimated to be 2% (Figure 3).17 Disease severity can range from a single episode of self-limiting patchy hair loss to chronic relapsing-remitting disease that may progress to alopecia totalis, a total loss of terminal hair on the scalp, or alopecia universalis, a total loss of hair all over the body. Ophiasis is a rarer subtype, in which patients experience hair loss on their posterior scalp in the occipital region, and is associated with a poorer prognosis. Patients with AA may also have nail changes, most commonly pitting. A classic clinical feature of AA is the presence of exclamation mark hairs, which are very short hairs that are wide at the top of the hair and thinner towards the end. Vellus (fine, nonpigmented) hair may also be present within patches or at the periphery.
{kind=link}
Therapy is aimed at arresting disease progression in the acute phase, and may reduce the risk of progression into chronic relapsing AA.18 Recent consensus guidelines suggest that patients with more than one patch of AA should be considered for active treatment, as more than half of these patients will go on to develop further patches in the subsequent months.18 Currently, therapies for AA are limited and usually provided in the specialist setting. For those with patchy disease, intralesional steroid injection can be useful; however, this is not feasible for extensive disease. The injections can be very painful and, in younger patients, high-potency topical corticosteroids can be used as an alternative. In patients with resistant disease, topical sensitisers such as diphenylcyclopropenone or irritants such as dithranol can be used to invoke an allergic contact dermatitis and promote hair growth.
Oral corticosteroids or steroid-sparing oral immunosuppressives such as methotrexate can also be used. Oral JAK inhibitors have shown promise in retrospective studies, but are not currently subsidised under the PBS for this condition and, therefore, their cost limits them from being widely used.19
Acne
Acne vulgaris is one of the top five reasons for dermatology referral in Australia (Figure 4).1 It is usually considered a disease of adolescence, triggered by the production of androgens; however, an increasing number of patients, particularly women, exp
{kind=link}
school children.21 It is a source of significant stress to patients, with one study reporting that 70% of acne patients feel embarrassed about their disease, and 27% had depression.22
Mild to moderate disease can be treated with topical adapalene, a topical retinoid, as monotherapy or in combination with benzoyl peroxide. For patients with resistant disease, oral tetracyclines can be trialled. However, treatment-resistant propionibacteria have been seen even in treatment-naive patients. In females, antiandrogens can be very successful – for example, spironolactone or oral contraceptives containing cyproterone acetate. If, however, the patient is nonresponsive after three to four months of treatment, referral to a dermatologist for isotretinoin should be considered.23 Patients with significant scarring at presentation, those with severe or resistant disease and those experiencing significant distress as a result of their acne should also be referred early for consideration of isotretinoin therapy.23 Isotretinoin has high efficacy and a very good safety record. A retrospective review of the adverse events associated with isotretinoin found lower doses were as effective as traditional high-dose therapy, but associated with fewer adverse events.24 The most common issues seen with isotretinoin are cheilitis (seen in 77 to 97% of patients), eczema (9 to 16%) and fatigue (7 to 20%). Mood changes were noted in up to 4 to 10% of these patients, and were dose dependent.24
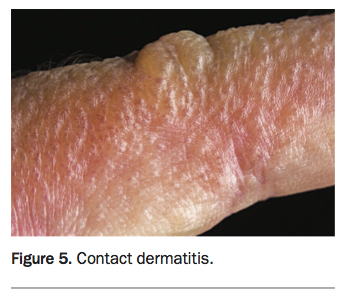
Allergic and irritant contact dermatitis
Allergic contact dermatitis is the most common skin condition to present in general practice (Figure 5).1 Common allergens include nickel, fragrance mix (containing the eight most common allergy-causing fragrances used in many products), Balsam of Peru and thimerosal.25 The disease distribution can assist with the diagnosis – for example, patients with a nickel allergy may present with a rash on their nasal bridge and temples if they wear spectacles with frames containing nickel, a rash on their earlobes and neck if they wear nickel-containing jewellery or a rash on their lower abdomen from their trouser buttons.
{kind=link}
Irritant contact dermatitis occurs with an earlier onset, and may present with a papulosquamous eruption or vesicular lesions. It often follows exposure to known allergens such as workplace chemicals or plant-based medicines and frequently affects the hands.
For localised lesions, moderate or high-potency topical corticosteroids (e.g. betamethasone dipropionate 0.05% ointment) are appropriate first-line therapy. The exception to this is lesions in areas that are more prone to possible corticosteroid side effects, such as in flexural areas or on the face, and weak topical steroids (hydocortisone 1%) or topical calcineurin inhibitors can be used in these cases. Patients with extensive disease (greater than 20%) can trial short courses of oral corticosteroids. Identification of the
causative agent is pivotal to effective management, and referral to a dermatologist for patch testing to identify topically encountered allergens should be considered in patients whose allergic trigger is not clear.
Infectious skin conditions
Tinea infections
Patients can present with tinea in many different locations. The most common is on the feet, known as tinea pedis. This infection can extend to the nails and cause localised dystrophy. Infection on the body is known as tinea corporis and classically presents with annular, scaly plaques. In children, tinea can affect the scalp, resulting in hair loss. Scalp involvement is not typically seen in adults; however, the beard and eyebrows can be affected.
Tinea pedis and tinea corporis can be managed effectively with topical therapy, such as topical terbinafine applied twice daily for four weeks.26,27 Before starting oral antifungal therapy, microscopy and culture is highly recommended. Oral antifungals such as terbinafine, fluconazole and itraconazole can be used in patients with resistant disease and those with hair loss. However, monitoring of liver function should be considered when using terbinafine.28
Cellulitis
Cellulitis is a skin infection which affects the lower dermis and subcutaneous tissue, and erysipelas is a closely related condition that affects the upper dermis (Figure 6). Patients presenting with either of these conditions usually have a well-demarcated area of erythema, local oedema and pain, often but not invariably with malaise and fever. It is frequently seen in patients with diabetes, venous stasis dermatitis, chronic kidney disease and tinea pedis. Classically, cellulitis is caused by Streptococcus pyogenes; however, other organisms such as Staphylococcus aureus and other rarer organisms may be implicated in erysipelas and atypical cellulitis presentations.
{kind=link}
Depending on the patient, stage of infection and comorbidities, classic cellulitis should be treated empirically with phenoxymethylpenicillin or cefalexin or with targeted antibiotics guided by the sensitivities.29
Clinicians should remember that there is a wide differential for cellulitis. The most common alternative diagnosis is venous stasis dermatitis, particularly when the rash is bilateral. Patients with severe venous insufficiency often have bilateral leg erythema with swelling, and careful clinical history regarding duration and concurrent infective symptoms should be taken to differentiate between this condition and cellulitis. In venous stasis dermatitis there are often other features of venous insufficiency such as haemosiderin staining, varicosities, lipodermatosclerosis or atrophie blanche. Other commonly seen differential diagnoses include tinea corporis or drug eruptions. In patients who do not respond to initial therapy, further investigation to exclude these conditions or referral to specialty care should be considered. Prolonged courses of empirical antibiotics without identification of a causative organism should be avoided.
Scabies
Scabies is a skin infestation with the Sarcoptes scabiei mite, transmitted by direct contact with affected people (Figure 7). In Australia, outbreaks are more common in tropical areas and central Australia as well as nursing homes.
{kind=link}
Diagnosing scabies can be difficult due to its varied presentation. Infestation should be considered in high-risk groups who have unexplained itch, persistent lesions resembling insect bite reactions, recurrent impetigo with itch and in older patients with new-onset dermatitis. Nursing home patients often have an atypical distribution, with the torso being the most commonly affected area.
The most commonly seen clinical features in nursing home patients are papules, followed by burrows and hyperkeratosis.30 Of note, 50% of patients in a prospective cohort study of nursing home patients with dementia did not report any symptoms of their scabies infestation.30 Clinicians should have a high index of suspicion and low threshold for treating scabies empirically in these high-risk groups.
Dermatological emergencies
Stevens-Johnson syndrome/toxic epidermal necrolysis
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are dermatological emergencies, with a mortality rate of up to 50% in TEN.31 Both are characterised by desquamation and mucosal involvement, with less than 10% of body surface area affected in SJS, 10 to 30% in SJS/TEN overlap and 30% or more in TEN. SJS and TEN are rare, with incidence estimated at one to two cases per million per year.32 SJS tends to be less severe than TEN, and is more commonly caused by infections, such as mycoplasma and herpes simplex virus. These patients typically do not have significant systemic symptoms. In comparison, TEN usually has a drug precipitant, and carries a mortality risk. In SJS/TEN overlap, it can be difficult to differentiate between the two and these cases are typically either drug induced or idiopathic.
The cutaneous findings are usually preceded by a flu-like prodrome and fever, and patients may experience dysphagia, conjunctivitis or photophobia as early features of the mucous membrane involvement. The classic feature of both is a positive Nikolsky sign, where a clinician can induce skin sloughing by applying gentle lateral pressure. The rash and mucositis usually progress rapidly from erythematous macules or targetoid lesions into bullous lesions and desquamation.
Common precipitants include allopurinol, antiepileptics, sulfonamide antibiotics, aspirin and other NSAIDs.33 A number of human leukocyte antigen (HLA) gene subtypes have been linked to an increased risk of SJS and TEN under certain conditions, such as with allopurinol use in patients with the HLA-B*58:01 allele and carbamazepine use in patients with the HLA-B*15:02 and HLA-A*31:01 alleles.33-36 Consensus is lacking regarding potentially screening high-risk patients for HLA subtypes before starting certain medications.
Patients with SJS or TEN require urgent referral for inpatient management, as the extensive skin loss can cause hypovolaemic shock, electrolyte imbalance, bacteraemia, acute renal failure and other organ dysfunction. After recovering from the acute stage of the illness, patients may have chronic eye disease, gingival inflammation and oral discomfort, vaginal dryness and dyspareunia, and bronchiectasis or chronic bronchitis, and will require ongoing outpatient monitoring.
Erythroderma
Erythroderma is a generalised, erythematous eruption that can be caused by multiple triggers (Figure 8). Drugs, infections, pityriasis rubra pilaris (PRP), lymphoma and widespread atopic dermatitis or psoriasis can all be associated with erythroderma.37 Patients present with diffuse erythema, which progresses to extensive exfoliation. Patients with PRP may also present with palmoplantarkeratoderma and islands of sparing (white areas of normal skin within the erythroderma).
{kind=link}
As the skin plays a major role in patients’ ability to control temperature and hydration, patients with erythroderma can have fever and other constitutional symptoms, hypotension due to dehydration, or high-output cardiac failure. These patients are usually managed aggressively as inpatients, with intravenous fluid replacement, electrolyte monitoring and topical corticosteroid therapy. Targeted therapy depending on the cause of erythroderma should also be started – for example, methotrexate for erythrodermic psoriasis.
Other drug hypersensitivity reactions
Drug hypersensitivity reaction is a frequent and varied presentation in general practice, and can present diagnostic dilemmas (Figure 9). Time from ingestion of the drug can vary from hours to weeks and symptoms may persist even after the causative agent is ceased.
{kind=link}
Identifying the causative agent is pivotal in managing these conditions, and creating a drug chart timeline can assist clinicians in isolating potential drug triggers. Patients with a classic maculopapular drug eruption typically develop symptoms four to 14 days after initial exposure, but conditions such as DRESS (drug reaction with eosinophilia and systemic symptoms) usually take two to eight weeks to develop.38
Withdrawal of the trigger is the most important step; however, the rash should be treated with topical corticosteroid and emollient therapy. In severe cases, oral corticosteroids may be required.
Conclusion
Patients with skin problems comprise 17% of general practice consultations in Australia. These can vary from autoimmune and inflammatory skin conditions such as dermatitis, psoriasis and acne to infectious diseases such as tinea, cellulitis and scabies to dermatological emergencies such as SJS and TEN. Therefore, it is important that GPs are aware of how to diagnose and manage these conditions, and know when to refer patients to a dermatologist or for inpatient management. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.