Foot problems in older people

Age-related fat pad atrophy, bony deformities such as hallux valgus (bunions) and hammer, claw and mallet toe, Morton’s neuroma, toe nail disorders and arthritis are common foot problems in older people. Resulting foot pain, deformity and loss of function can significantly compromise an older person’s mobility and independence.
- Most foot problems in older people can be improved by shoe modification and use of cushioned insoles.
- The most useful investigation for patients presenting to their GP with foot problems is a weight-bearing anteroposterior and lateral x-ray series; cross-sectional imaging of the foot has limited value in general practice.
- Neuritic or burning type pain radiating to the third and fourth toes is a classic symptom of Morton’s neuroma.
- Generalised numbness or pain radiating down the leg to the foot suggests either peripheral neuropathy or nerve root compression.
- Toe nails that are thick and crumbly raise the suspicion of fungal nail infection, and nail clippings should be sent for microscopy and culture.
- Rapid progression of deformity in a person with known or suspected diabetes warrants urgent referral to an orthopaedic surgeon or at-risk foot clinic.
Picture credit: info.Michaelheim-photographer.com/DepositPhotos Model used for illustrative purposes only
With our ageing population, painful conditions of the foot are becoming more prevalent. Foot pain, progressive deformity and loss of function after a lifetime of loading are seen by many as a natural consequence of getting older. However, age-related loss of natural soft tissue fat cushioning, loss of skin elasticity, bony deformity and difficulty with basic foot care can lead to significant problems that may compromise an older person’s ability to maintain their independence.1 In many cases, these foot issues contribute to multifactorial problems that can increase falls risk, with its well-documented associated morbidity and mortality.2 It is estimated that foot pain affects one in four older people, with forefoot pain affecting two- thirds of those patients.3
This article describes common conditions of the foot seen in older people and summarises the recommended general practice management, imaging, referral route and, if required, eventual surgical management.
Lesser toe deformities
Deformities of the lesser toes are among the most prevalent problems in the older population presenting to foot and ankle surgeons. These deformities may be an isolated problem or seen in combination with other forefoot deformities such as hallux valgus or first metatarsophalangeal (MTP) joint arthritis. In the early stages of development of lesser toe pathology, deformities are likely to be flexible rather than rigid, and be fully correctable. Loss of normal lesser toe function increases forefoot pressure during the late stance phase of gait, leading to forefoot pain or metatarsalgia. By the time patients seek medical attention, the deformity has usually become painful with a degree of stiffness. Often, painful forefoot deformity and metatarsalgia occur together, with pain arising from the level of the MTP joint of the toe, the metatarsal head or the interphalangeal joint deformity.
History and examination
A thorough history should include screening questions for diabetes, rheumatoid arthritis and peripheral vascular disease. Decreased sensation in the foot is common in people with diabetes and can lead to ulceration in the presence of even minor deformity. If peripheral vascular disease is present then it may be prudent to investigate this and discuss management with the vascular team before considering foot surgery to correct the deformity.
The examination should start with inspecting the feet with the patient standing, looking for deformities of the lesser toes and callosities. Lesser toe deformities include:
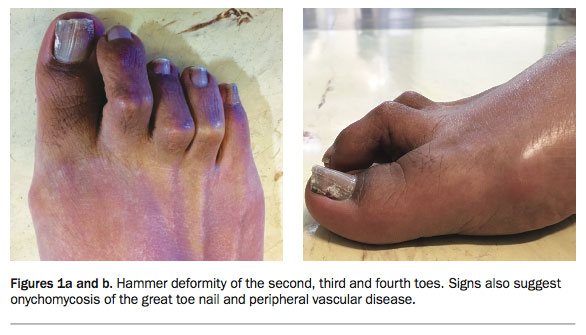
- hammertoe – a flexion contracture of the proximal interphalangeal joint (Figures 1a and b)
- claw toe – hyperextension of the MTP joint and flexion of the proximal and distal interphalangeal joints
- mallet toe – a flexion contracture of the distal interphalangeal joint.
{kind=link}
Lesser toe deformities may be associated with dorsal callus overlying the flexed joint or over the tip of the toe. A callus in the web space between the lesser toes is a soft corn, caused by pressure from the bony prominences of the neighbouring toes.
Next, the sole of the foot should be inspected with the patient sitting. Callus under the forefoot indicates a site of increased pressure or the presence of a swelling or lesion. Callosity beneath the metatarsal head and overlying the proximal interphalangeal joint may be associated with a hammer toe deformity. Callosity or corns may develop over the tip of the toe in claw toe or mallet deformity. As toe deformity progresses, the MTP joint may dislocate and thicker callus may develop. A callus that develops beneath one or more of the lesser metatarsals in this situation is termed an intractable plantar keratosis.
It is also important to assess the patient’s peripheral circulation and sensation as inadequate peripheral perfusion or lack of protective sensation can cause wound complications following corrective surgery.
Investigation
Simple weight-bearing x-rays of the foot with anteroposterior and lateral views are usually sufficient to plan treatment of lesser toe deformities. Most patients with isolated lesser toe deformity can be advised on treatment without further investigation. However, in patients who might have inflammatory arthritis as the underlying cause, a routine full blood count and measurement of erythrocyte sedimentation rate and levels of C-reactive protein and rheumatoid factor may be indicated. Patients with progressive or asymmetrical deformity should be investigated for associated central or peripheral neurological conditions, with spinal and possibly cranial MRI or nerve conduction studies as well as screening for diabetes.
Rapid progression of deformity in an erythematous, hot foot is a red flag, especially in a patient with known or suspected diabetes or other cause for peripheral neuropathy. There should be a high suspicion of Charcot neuroarthropathy, and patients require urgent referral to an orthopaedic foot and ankle specialist or a multidisciplinary ‘at-risk foot’ service.
Management
Most older patients with isolated lesser toe deformity or pain can be treated initially with nonsurgical techniques. General advice on foot care and the involvement of a chiropodist to deal with troublesome callus and corns are sufficient in many cases. This, together with education about appropriate footwear selection (shoes with a broad and deep toe box area and soft uppers), is often all that is required in older people.
If conservative options fail then referral to an orthopaedic surgeon is warranted. Patients should be counselled that surgery to treat lesser toe deformities may include lengthening of extensor tendons, flexor tenotomies, osteotomies of the phalanges and surgical fusion of the affected joints of the small toes. These procedures are simple to perform but often involve insertion of a wire or implant to stabilise the toe. After surgery, patients must wear a stiff-soled ‘postoperative’ shoe for six weeks to protect the fusion site. Patients can then return to normal footwear after removal of any wires in theatre or the clinic. Implants are not removed.
Hallux valgus (bunion)
Bunions are complex deformities that cover a spectrum from true hallux valgus to bony projections associated with arthritis of the first MTP joint, as in hallux rigidus. However, patients often use the term bunion to refer to any deformity of the medial border of the foot with a prominence over the great toe MTP joint. Bunions or hallux valgus have a reported prevalence of up to 35% in patients over the age of 65 years.4
There is a strong family history in up to 90% of patients with hallux valgus.5 The link to use of inappropriate footwear is not clear cut. Hallux valgus occurs in many populations that do not wear shoes, although with a much lower prevalence than in shoe-wearing populations.
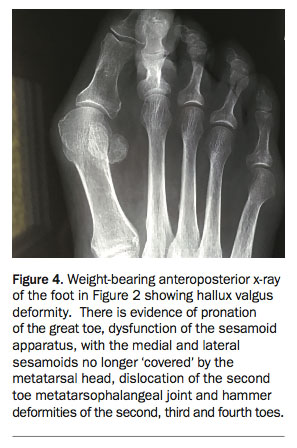
Hallux valgus is actually a complex series of deformities that lead to lateral deviation of the big toe. The change in shape of the foot and associated change in the mechanics of weight-bearing cause discomfort when the patient wears enclosed footwear. The lateral deviation and pronation of the great toe cause the normal sesamoid weight-bearing apparatus to lose function and overload the lesser toe MTP joints. This can lead to forefoot pain and often to lesser toe abnormalities such as hammer or claw toes (Figure 2).
{kind=link}
In severe cases of hallux valgus the great toe may deviate so far laterally that it causes the second toe to cross or ride over it. The term crossover toe is reserved for a medial deviation of the second toe at the level of the MTP joint, leaving a gap between the second and third toes. This can occur with or without a hallux valgus deformity (Figure 3). Crossover toe is associated with disruption to the plantar plate complex.
{kind=link}
History
It is crucially important to identify the patient’s exact symptoms and whether they have presented because of these symptoms or other reasons. Often an older person has lived with the foot deformity for many years and presents because of fear that it will progress and they will ‘end up like my mother/grandmother/aunt’ rather than specific symptoms. Older patients are also sometimes under pressure from family to have their ‘bunions sorted’. The progression of hallux valgus is slow, and if there is significant deformity then it has probably been present for many years and is likely to have been well tolerated by the patient. If deformity has progressed and is now causing local pressure symptoms or forefoot pain then surgical treatment is an option. Surgery is generally not recommended for people with asymptomatic hallux valgus.
Examination
Simply observing the patient when standing and walking provides most of the required information in hallux valgus. Do they have evidence of breakdown of the medial skin over the MTP joint? Do they walk on the lateral border of the foot to avoid weight- bearing on a painful hallux or second metatarsal as with transfer metatarsalgia? The general weight-bearing alignment of the foot should also be inspected. Hallux valgus is often seen in association with flat foot deformity in older patients. When the patient is examined sitting, is there evidence of corns or callus formation? Is the MTP joint of the great toe painful when moved passively? If so then there may be a degree of arthritic change affecting the joint.
AdvertisementInvestigation
The diagnosis of hallux valgus is clinical, but imaging can be useful to rule out arthritic processes of the neighbouring joints. Routine weight-bearing anteroposterior and lateral x-rays are all that is required to plan surgical treatment (Figure 4). Concerns about peripheral circulation and sensation should be addressed as for lesser toe deformities (see above).
{kind=link}
Management
Initial management of hallux valgus by the GP should involve advice about footwear that accommodates the patient’s deformity. If no suitable shoe can be purchased over the counter then referral to an orthotist may be helpful. The addition of bunion pads, splints and other commercial products may help in relieving symptoms. Simple orthotics that support the medial arch and offload the metatarsals may be considered, but custom orthotics have limited value.
Surgical management should be considered if nonoperative treatment has failed to resolve symptoms or if skin breakdown over bony prominences is imminent. All surgical treatments require the metatarsal and possibly the phalanx of the great toe to be cut and repositioned. There is no role for bunionectomy in the treatment of hallux valgus. Patients can generally bear weight postoperatively in a stiff-soled sandal, which must be worn for six weeks after surgery. In older patients, mobility may be compromised in the immediate postoperative period, and attention should be paid to the patient’s home and support environment before specialist referral.
Fat pad atrophy
With ageing, loss of the normal cushioning effect provided by the plantar fat pad is a common cause of foot pain. Although this occurs often in older people, it has multifactorial causes, including diabetes, rheumatoid arthritis, peripheral vascular disease, trauma and chronic corticosteroid use. The loss of this protective adipose tissue and the surrounding collagen septae can expose the underlying delicate neurovascular structures to excess load and shear forces. In the compromised neuropathic foot often seen in people with diabetes, these excess forces can lead to break down of skin and ulceration exposing bony prominences.
Investigation
The diagnosis of fat pad atrophy is essentially clinical. Thinning of the plantar fat pads allows the underlying bony structures to be more easily palpated during clinical examination. Fat pad atrophy can be distinguished from plantar fasciitis causing heel pain as the symptoms of fat pad atrophy are often bilateral with central heel pain. In contrast, plantar fasciitis typically causes medial heel pain in one foot. As with most foot pathologies, simple weight-bearing anteroposterior and lateral x-rays are useful and may help to rule out other causes for the patient’s foot pain.
Management
Offloading and cushioning of the affected area should be the mainstay of management. This is done with a variety of pads, orthotic inserts and shoe modifications, which can be obtained from a podiatrist. If imminent ulceration is a concern then the patient should be referred to an orthopaedic surgeon for assessment. Osteotomies or resection of prominent underlying bone are sometimes required.
Morton’s neuroma
Patients with Morton’s neuroma most often complain of a burning sensation in the forefoot and sometimes an associated clicking or catching sensation. The pathogenesis of the condition is poorly understood. The common digital nerve can be entrapped without inflammation in either the third–fourth or second–third web spaces secondary to several potential causes. Discomfort is often poorly localised by the patient, but pain may radiate to corresponding toes and there may be associated altered sensation or numbness. The pain is worsened by wearing enclosed or ill-fitting shoes and is reduced when walking bare foot.
Examination
Examination may reveal a slight fullness over the affected area. Gentle palpation of the affected web space often reproduces the patient’s pain. Mulder’s sign may be positive, with a painful click elicited by compression of the foot with one hand and simultaneous upward thumb pressure under the affected web space (Figure 5).6 This is caused by subluxation of the neuroma beneath the transverse metatarsal ligament.
{kind=link}
Imaging
The diagnosis of Morton’s neuroma is based on the patient’s history and physical findings. Plain weight-bearing x-rays are again helpful to assess the foot in general and to identify any underlying bone or joint disease that may be causing symptoms or may coexist. Ultrasound examination may be helpful in some situations but is often operator dependent and has too high a rate of false positive and false negative results to be relied on for diagnosis.7 MRI may be useful in some patients to rule out other pathologies but is not warranted for establishing the diagnosis of Morton’s neuroma. There is no need for electrodiagnostic studies unless peripheral neuropathy or radiculopathy is suspected because of atypical symptoms. These include bilateral generalised numbness, numbness in the sole of the foot or neuritic pain radiating from the back or buttock down the leg to the foot.
Management
Initial management of Morton’s neuroma should be conservative and directed toward the use of accommodative footwear that does not cause compression across the forefoot. A metatarsal bar or Morton’s domed insert can be requested from the orthotist, which relieves pressure on the affected common digital nerve. Ultrasound- guided corticosteroid injections to the affected web space can be beneficial. There is good evidence supporting their benefit for short-term relief but they are unlikely to cure the patient’s symptoms in the long term.8 Ultimately, surgical excision is likely to be the solution if symptom relief cannot be achieved with nonoperative treatment. Patients should be made aware that the procedure will cause an area of numbness in the affected toes that is likely to be permanent but will likely resolve the pain.
Toe nail abnormalities
Toe nail disorders are among the most prevalent causes of foot pain in older people.9 Ingrowing toe nails (onychocryptosis), hypertrophy of the nail plate (onychauxis or onychogryphosis) and fungal nail disorders (onychomycosis) are the most common of these disorders.
Examination
The patient’s description of the nail is often enough to identify the pathology. A nail in which the side of the nail plate extends farther into the nail groove causing pain or inflammation is consistent with an ingrowing nail. A thickened nail plate or one that is thickened and has a hooked appearance is likely to represent onychauxis or onychogryphosis, respectively. A thickened nail plate with a dusty yellow or brown discolouration is likely due to fungal nail infection.
Investigation
Ingrowing toenails do not require routine microbiological assessment. Most infections in ingrowing toe nails are caused by Staphylococcus aureus and, less frequently, Gram-negative bacteria (e.g. Pseudomonas spp.) and Streptococcus spp.10 Studies have shown that these infections settle without antibiotics after removal of the ingrown portion of the nail and matricectomy.11 In patients with hypertrophy of the nail plate, microscopy and culture of nail clippings are useful to rule out an underlying fungal cause.
Management
Management of an ingrown nail starts with patient education on nail cutting and hygiene. The nail should be cut square to reduce the corners digging into the nail fold. Acute infection may be treated with a short course of oral antibiotics. Should these methods fail to relieve symptoms then referral to a podiatrist or orthopaedic surgeon may be suggested to perform partial avulsion of the lateral edge of the nail followed by surgical or chemical matricectomy. With appropriate training, GPs can perform these procedures without the need for onward referral.
Fungal nail infection is treated with targeted antifungal agents administered either topically or systemically. In the absence of fungal infection, hypertrophied nails are treated with regular cutting or grinding of the nail to debulk it and reduce local pressure symptoms or nail avulsion and ablation of the germinal matrix.
Arthritis
With increasing age, the prevalence of arthritis in the foot and ankle increases. Although it is beyond the scope of this article to describe each arthritic foot complaint, initial management and investigation are similar. Weight-bearing x-rays of the affected foot should be performed. No cross-sectional imaging is required as this would add little information that is not provided by careful review of the x-rays; such imaging is best requested by the orthopaedic surgeon to answer a specific preoperative question.
Management
In older patients, the use of orthotics that support the medial arch of the foot and relieve pressure on the metatarsal heads has been shown to improve mobility and symptoms of foot pain in older women.12 Patients need to be able to accommodate the orthotics within their footwear and to transfer them between their various shoes. Any change in local pressure symptoms or imminent ulceration should prompt review of all orthotics and footwear.
If orthotics and simple oral and topical analgesics are ineffective or not well tolerated then referral to an orthopaedic surgeon should be considered. Image-guided injections of local anaesthetic and corticosteroid may be considered but are often not a long-term solution for patients with advanced arthritis.
Surgical treatment of most forefoot, midfoot and hindfoot arthritis comprises arthrodesis (fusion) of affected joints and removal of associated pressure areas. Management of ankle arthritis is more controversial, with newer joint replacement techniques and implants available (Figures 6a to c), although arthrodesis is still considered the gold standard treatment. Patients must be warned that all surgical treatments will most likely involve a period of enforced nonweight-bearing and use of a plaster cast. For these reasons, many older patients opt to persevere with nonsurgical treatment, as surgery can be more disruptive than their current symptoms.
{kind=link}
Conclusion
Foot pain is common in older people and has a variety of overlapping causes. It may significantly affect an older person’s ability to maintain their independence and mobility. Thorough history taking and focused examination are vital to establish a diagnosis and to start treatment in the general practice setting before specialist referral. GPs should maintain a high index of suspicion for diabetes, neuropathy and peripheral vascular disease and investigate appropriately before referring patients to an orthopaedic surgeon. Weight-bearing anteroposterior and lateral x-rays should be the first-line radiographic investigation for all patients with chronic foot pain and deformity.
Exploring the patient’s expectations and concerns may reduce the number of inappropriate referrals to foot surgeons. For many patients with asymptomatic foot deformities, the treatment is reassurance alone. Even in those with complex deformities, simple solutions such as wider fitting shoes, toe sleeves or spacers to stop rubbing of a painful toe may be all that is required. MT
References