Ankle sprains: the highs and the lows

The majority of ankle sprains are low sprains that can be managed conservatively, but orthopaedic referral should be arranged if a high sprain is suspected. Referral is also warranted for any patient with an ankle sprain if symptoms are not improving as expected or if concomitant injuries are present.
Ankle sprains are common, accounting for 3 to 5% of emergency department presentations.1 They are frequently caused by a sporting or dancing injury and are often the result of a twisting mechanism leading to inversion of the ankle. They are more common in patients with ligament laxity. Females experience a higher incidence of ankle sprain compared with males (13.6 vs 6.94 per 1,000 exposures).1
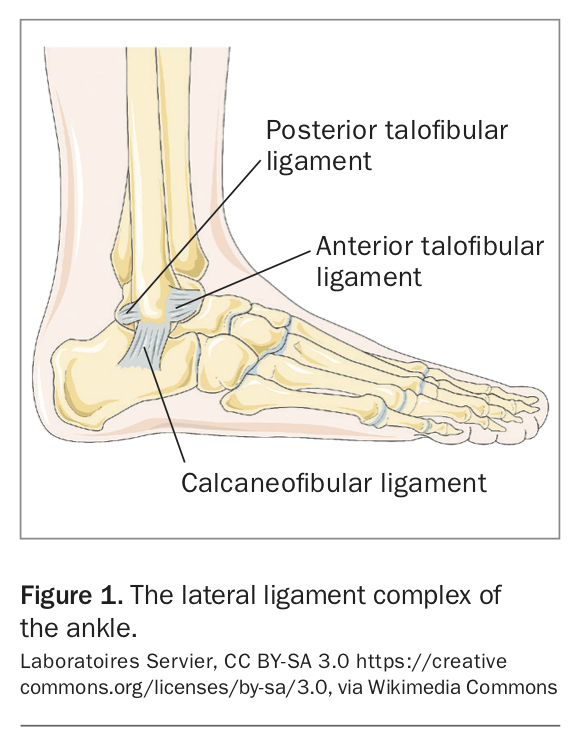
There are two types of ankle sprain: low (>90% of cases) and high. Low ankle sprains involve injury to the lateral ligament complex (Figure 1), which comprises the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL) and posterior talofibular ligament (PTFL). The ATFL is the first ligament to rupture and is very commonly injured. In more severe injury, the CFL may also be affected whereas the PTFL is the least commonly ruptured.
{kind=link}
High ankle sprains involve injury to the ligaments that connect the tibia and fibula (syndesmosis). They are much less common than low ankle sprains and take longer to heal.
History
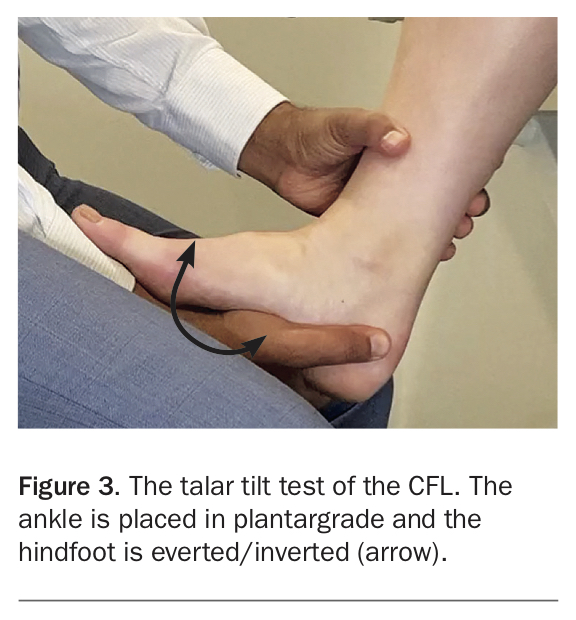
A careful history is important for the patient presenting with ankle pain after injury and will help to confirm the diagnosis. Although most ankle sprains are isolated ligament injuries, they can be associated with other injuries, such as fractures or osteochondral or tendon injuries. Important causes of ankle pain after injury are listed in the Box.
{kind=link}
It is helpful to begin by asking about the mechanism of injury. A higher energy injury is likely to result in a more severe sprain and may include damage to other structures. For example, an ankle injury sustained while walking or running on uneven ground is more likely to involve plantarflexion and inversion, resulting in a lateral ligament injury. An injury sustained while playing a contact sport – such as during a football tackle – is more likely to involve dorsiflexion and external rotation, which is more prone to fracture and high ankle sprains.
The location of the pain can help differentiate between high and low ankle sprains. If the patient points to the distal tip of the fibula (or just anterior to the distal tip), this suggests a low ankle sprain. Patients with a high ankle sprain often have pain around the anterior aspect of the ankle joint (around the syndesmosis), more proximal than the pain of a low ankle sprain and in some cases as high as the proximal fibula (lateral aspect, just below the knee). Thus, careful assessment of the knee is also required.
Injuries to surrounding structures should be suspected if there is pain in other areas. For example, pain around the proximal fifth metatarsal may indicate a fracture in that location. Pain around the medial ankle joint (different to the tip of the medial malleolus) raises suspicion of a talar dome injury.
Enquiry about weight bearing after the injury is essential. A patient who is able to weight bear immediately after, or perhaps after some rest, is likely to have a milder ankle sprain. A patient who has to be taken off the field on a stretcher and is not improving as expected warrants further assessment to exclude other potential injuries.
Asking about previous episodes gives an indication of ankle instability. This includes feelings of ‘trust’ in the ankle – that is, whether the patient can trust the ankle to perform sports or everyday activities. Patients who have frequent episodes of ankle instability are, despite appropriate physiotherapy, likely to develop ankle issues later in life.
Examination
A careful and thorough examination should be performed for a patient with a suspected ankle sprain, which should include the knee and foot. Swelling and bruising of the ankle may indicate severity of injury and should be noted and compared with the other ankle. The patient’s ability to weight bear on the injured leg should also be noted.
Careful palpation to assess tenderness at specific locations around the ankle joint is key in discerning lateral ankle sprains from other concomitant injuries. The general area will be painful or tender; however, asking the patient for the point of maximal tenderness while palpating can help delineate the possible injuries. Good patient rapport is important because it is necessary to palpate the sore area and trust between physician and patient is of great help in this regard.
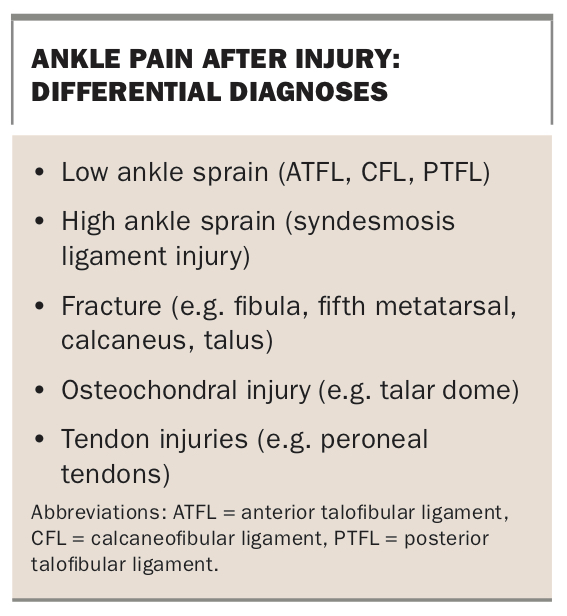
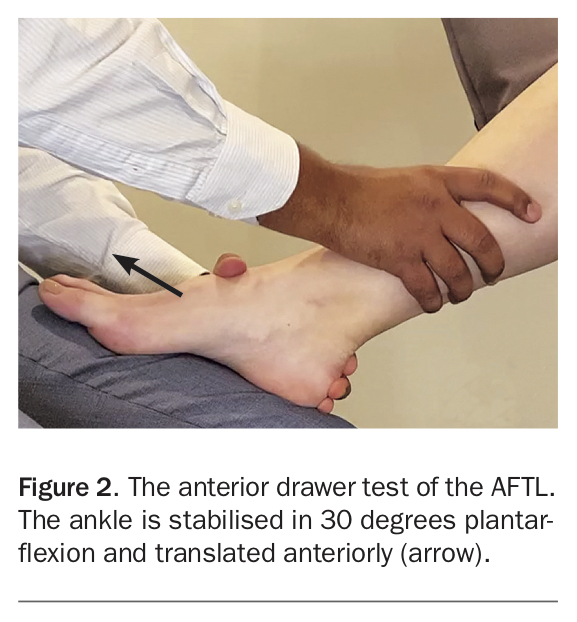
Tenderness around the distal tip of the fibula (or just anterior to the tip) is likely to be due to a low ankle sprain. The ATFL is best tested with an anterior drawer test with the ankle in plantarflexion (Figure 2). CFL competency can be tested with a talar tilt test (Figure 3) or a drawer test with the ankle in the neutral position.
{kind=link}
{kind=link}
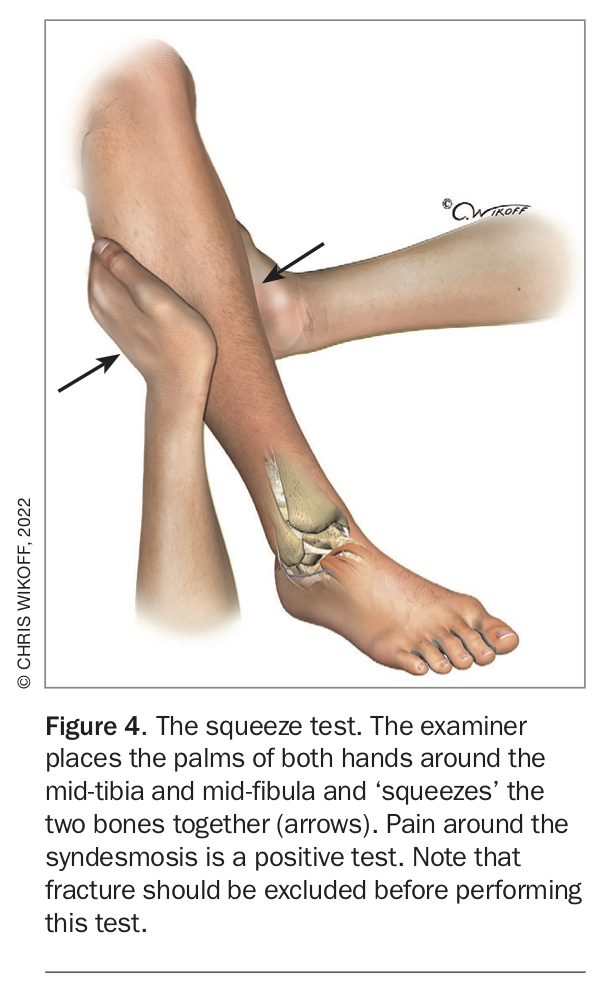
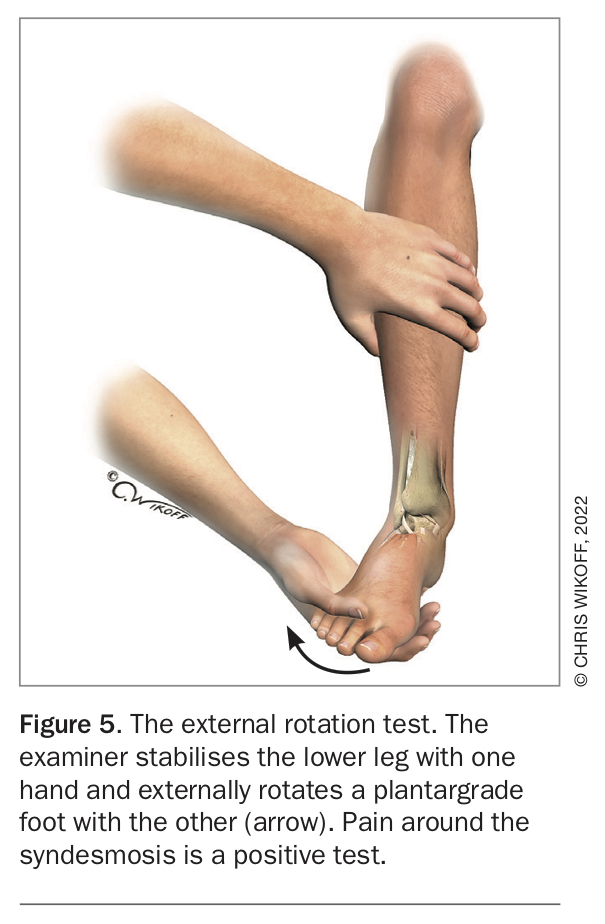
Tenderness around the anterior aspect of the ankle (proximal to the ATFL) is likely to be due to a high ankle sprain, and palpating around the entire length of the fibula will help in the assessment. Concerns for a high ankle sprain can be assessed using the tibia-fibula squeeze test (Figure 4), noting that it is prudent to exclude a fracture before performing this test.2 The external rotation test can also be used to assess the syndesmosis (Figure 5).2
{kind=link}
{kind=link}
Tenderness posterior to the fibula raises suspicion of a peroneal tendon injury. Tenderness around the tip of the medial malleolus may indicate injury to the deltoid ligament, while tenderness around the medial aspect of the ankle joint may indicate pathology such as an osteochondral injury to the talar dome. Tenderness around the proximal aspect of the fifth metatarsal is indicative of fracture.
A thorough neurovascular examination is then performed. Assessment of the peripheral pulses and capillary refill (<2 seconds) is needed to ensure no major vascular disruption has occurred. A diffuse dysaesthesia may be the result of a superficial peroneal nerve injury that may indicate a syndesmosis injury or fracture.
Imaging
X-rays (preferably weight bearing) are the first line of imaging and should be performed in line with the Ottawa ankle rules, which are available online (see, for example, https://www.mdcalc.com/ottawa-ankle-rule). However, if there is any doubt about the diagnosis then ankle x-rays are recommended.3 The ankle x-ray series includes anteroposterior, lateral and mortise views. The ankle joint itself should be assessed for widening and fractures can be determined. Areas of tenderness noted during the clinical examination should be scrutinised.
A CT or MRI is not routinely performed unless there is concern for an osteochondral injury, tendon or other soft tissue injuries, or suspicion of a high ankle sprain. This is determined by the history and clinical assessment. If there is reasonable suspicion of concomitant injury or if the history and examination findings are inconsistent then additional imaging needs to be considered. It may also be considered if the patient is not progressing as expected or if there are ongoing significant symptoms more than six weeks after injury.
Management
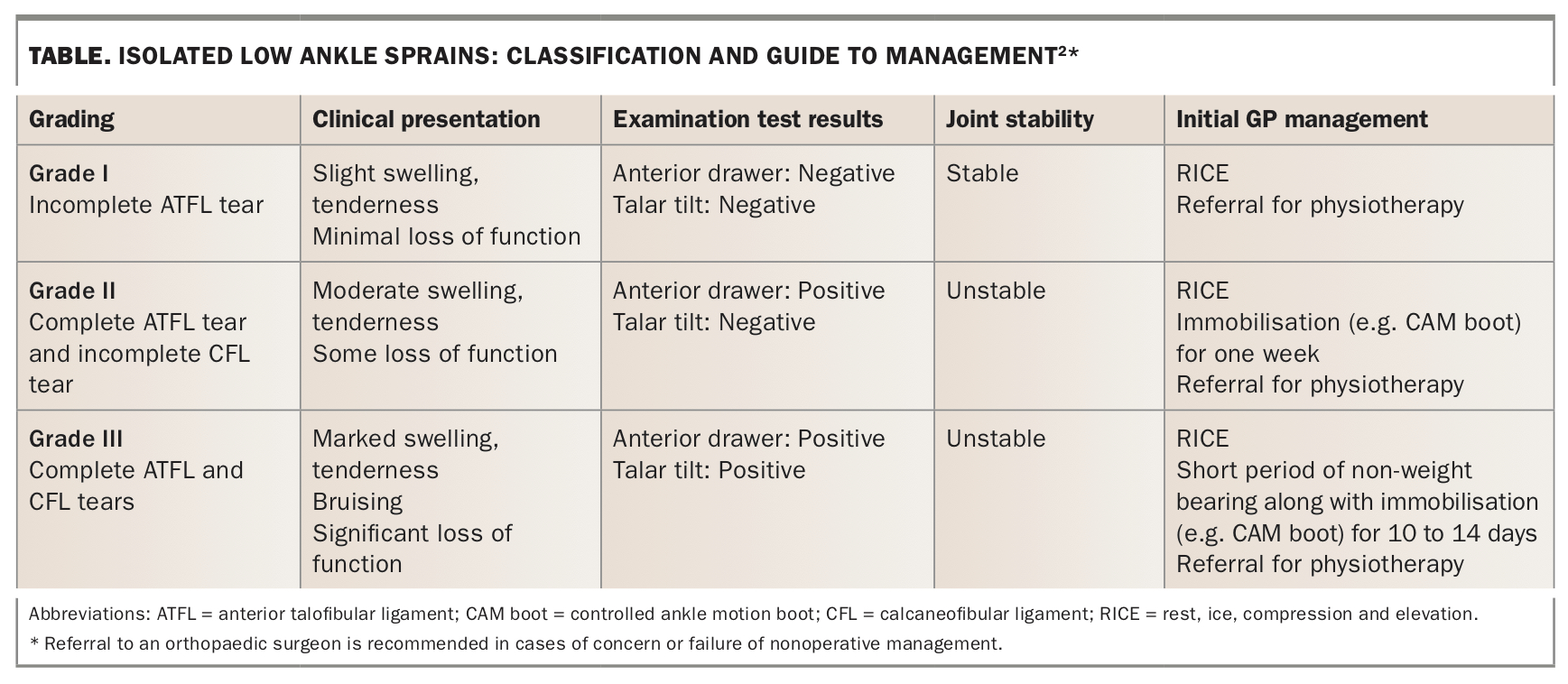
There are three grades of low ankle sprains (Table). The vast majority are managed with rest, ice, compression and elevation.4 A short course of simple oral/topical analgesia, especially anti-inflammatories, can be useful. Some patients with more severe sprains may require a period of immobilisation while weight bearing (and possibly a short period of non-weight bearing), but early mobilisation and physiotherapy facilitates a better recovery. The mainstay of physiotherapy includes range of motion exercises followed by strengthening and balance (proprioception) exercises. Patient education about ‘warm up’ exercises is helpful, as the likelihood of an ankle sprain may be reduced with preventive training programs.
{kind=link}
Surgical intervention is rarely warranted for an isolated low ankle sprain.4 Operative management is reserved for patients with chronic ankle instability or other concomitant pathology requiring surgery or, rarely, for an elite athlete. The surgery is individualised and may include an ankle arthroscopy or lateral ligament reconstruction and address other pathology that may be present.
A high ankle sprain can be treated conservatively in a controlled ankle motion (CAM) boot cast and a period of non-weight bearing if the syndesmosis is intact. However, if the syndesmosis is not intact then prompt surgical treatment is recommended for reduction and stabilisation.
The use of injections such as corticosteroids, platelet-rich plasma or hyaluronic acid along with other emerging therapies in ankle ligament injury is controversial with a lack of evidence from large randomised controlled trials.5-9 Thus, they are not recommended in the acute setting at present. Future trials may further evaluate the efficacy of such therapies.
Referral
For a patient with a simple low ankle sprain, it is important to refer to an orthopaedic surgeon if symptoms are not improving with nonoperative management as predicted or if ankle sprains are occurring repeatedly. Referral should also be made if there is concern for a high ankle sprain or other concomitant injuries.
Rarely, ankle sprains can be associated with complex regional pain syndrome. This can be difficult to treat and require a multidisciplinary team that involves allied health as well as pain specialists.
Conclusion
Ankle sprains are common, with low sprains occurring more frequently than high sprains. The mainstay of treatment is nonoperative and early functional rehabilitation, but patients with chronic ankle instability or concomitant injuries may need surgical intervention. Referral to an orthopaedic surgeon is recommended in cases of concern – including suspected high ankle sprain – or failure of nonoperative management. MT
COMPETING INTERESTS: Dr Mittal reports grant funding from the Australian Orthopaedic Association Research Foundation.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.