Walking away from heel pain

Although heel pain usually occurs due to biomechanical factors, the aetiology is multifactorial. The most common causes are plantar fasciitis and Achilles tendinopathy. Management strategies revolve around pain reduction, adjustment of load and strengthening.
- Heel pain usually occurs due to biomechanical factors.
- The most common causes of heel pain are plantar fasciitis and Achilles tendinopathy.
- Heel pain can occur secondary to an underlying inflammatory arthropathy, in which case referral to a rheumatologist is recommended.
- Most cases of heel pain can be diagnosed clinically.
- Depending on the underlying aetiology, a guided exercise program may be warranted for the management of heel pain.
- The prognosis of plantar fasciitis and Achilles tendinopathy is favourable.
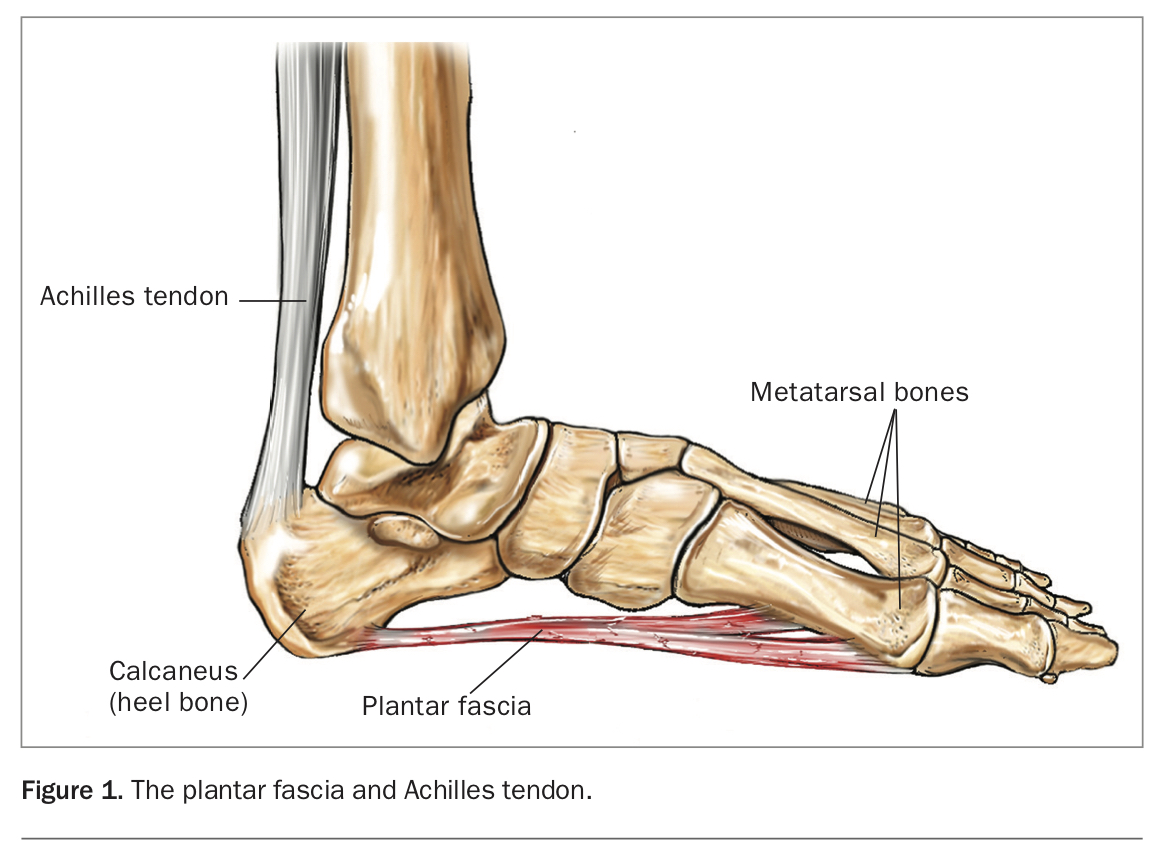
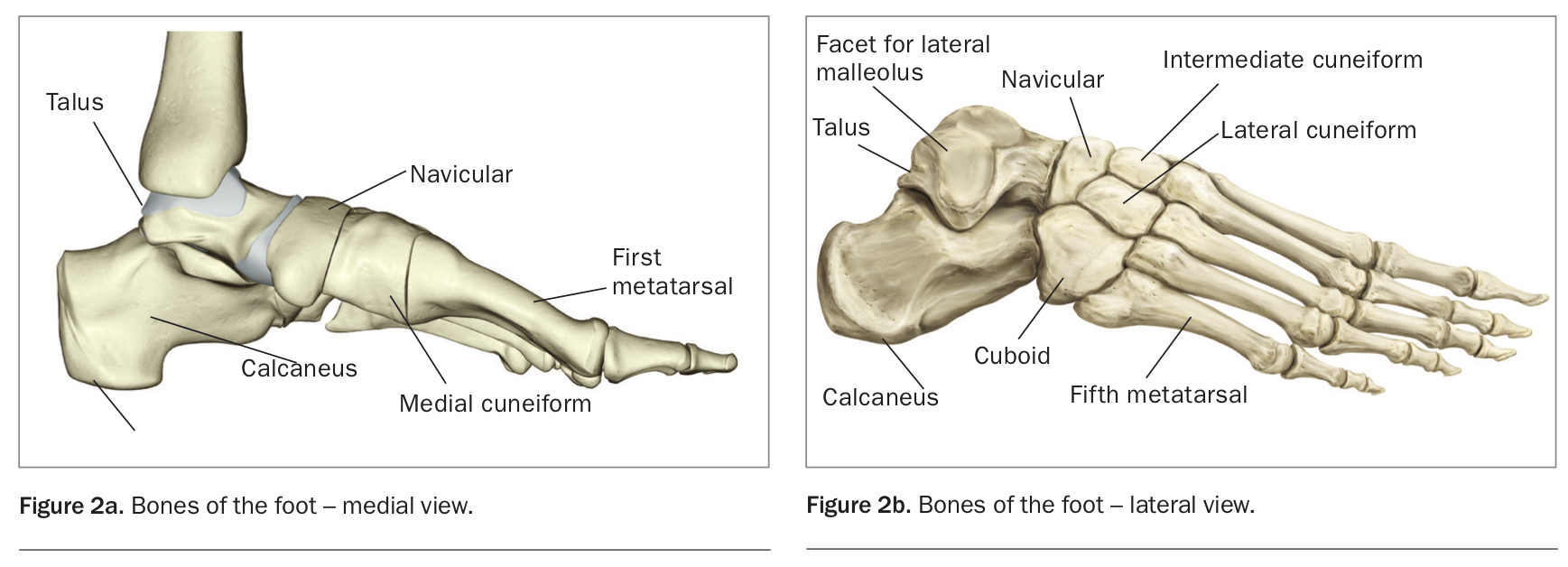
Foot pain is common and can significantly impact on quality of life by causing discomfort and disability.1 It most often affects the forefoot, followed by the midfoot and hindfoot, respectively. The hindfoot bones include the talus and calcaneus (heel bone), as seen in Figure 1 and Figure 2.2 This article will focus on heel pain.
{kind=link}
{kind=link}
The timely and appropriate management of heel pain relies upon an accurate diagnosis, and often the identification of a trigger. It is important to take a detailed history and to perform a focused examination. The most common causes of heel pain are plantar fasciitis and Achilles tendinopathy. Less common causes of heel pain include fat pad atrophy, posterior tibial nerve entrapment (tarsal tunnel syndrome), stress fractures and inflammatory arthropathies.
Functional anatomy
The calcaneus is the largest bone in the foot.3 It functions as a point of attachment for muscles that enable movement of the toes, structures that provide arch support to the foot, such as the plantar fascia and the long plantar ligament, and the Achilles tendon.3 The calcaneus receives its blood supply from branches of the posterior tibial and fibular arteries, and its nerve supply from branches of the tibial and sural nerves.3 The subtalar joint, comprised of the talus and calcaneus, enables inversion and eversion of the ankle. The talocrural joint, comprised of the talus and tibia, enables dorsiflexion and plantarflexion of the ankle.3
History
A detailed history is integral in determining the patient’s diagnosis and management strategies. The history should characterise the heel pain as well as its impact on function.
Location of pain
Plantar aspect of heel
This usually affects the medial process of the calcaneal tuberosity where the plantar fascia attaches proximally, and is suggestive of plantar fasciitis.4
Posterior aspect of heel
This is broadly divided into two areas:5
- pain at the Achilles insertion on the calcaneus is suggestive of Achilles enthesopathy or retrocalcaneal bursitis
- pain at the Achilles musculotendinous junction (a few centimetres above the Achilles insertion) is suggestive of Achilles tendinopathy, a tear or posterior impingement.
Medial aspect of heel
Pain extending from the medial aspect of the ankle to the region of the navicular is suggestive of tibialis posterior tendon dysfunction. If there is referral of pain to the big toe, the flexor hallucis longus may be involved. If there is associated paraesthesia in the region of the medial malleolus, tarsal tunnel syndrome is a possibility.6
Onset of pain
Generally, the onset of heel pain is gradual. It is important to clarify whether there have been any changes to load on the foot. This may include: a change in footwear; an increase in physical activity (e.g. running distance, running pace); a change in sport; a previous injury; and weight gain.5 A change in load over a short period of time is suggestive of a load injury such as a tendinopathy. If no loads have changed, and the patient has had a gradual increase in pain, other causes include osteoarthritis of the subtalar or talocrural joints.
A sudden onset of pain in the context of exercise or trauma may be secondary to a calcaneal fracture or a tendon tear.
Exacerbating and relieving factors
Pain on taking the first steps of the day or following prolonged rest is suggestive of plantar fasciitis.7
Pain in the morning after having done activity the previous day is suggestive of a load injury such as a tendinopathy.
Associated features
If there is pain affecting the heels bilaterally or if other joints are involved, an inflammatory arthropathy needs to be considered. Early morning stiffness of more than 30 minutes duration is also suggestive of an inflammatory arthropathy.
Impact on function
Heel pain commonly has an impact on activities such as walking, sport and ability to work, and the use of walking aids or orthoses may be considered to alleviate the pain.
Examination
A focused examination is used to confirm the provisional diagnosis based on the history and to rule out differential diagnoses. It follows the principles of look, feel and move (including assessment of function), as well as special tests.
Look
Ask the patient to stand. Look for hallux valgus, swelling, dactylitis and the extent of arch pronation and supination. Look for the integrity of the tibialis posterior tendon by using the ‘too many toes’ sign. This is positive if more than two toes are visible on the lateral border of the affected foot when observing from behind.8 Look at the knee and assess whether there is a varus or valgus deformity, which can affect the distribution of force through the foot.
Feel
Ask the patient to lie supine with their ankles hanging off the edge of the bed. Identify tender landmarks as discussed above. While they are in this position, do the Simmonds–Thompson test as described below.
Move
Compare the active and passive range of motion of the ankle on plantarflexion, dorsiflexion, inversion and eversion to the contralateral side. Assess the range of motion of the joints above (knee) and below (midfoot and first metatarsophalangeal joint) the ankle to identify any factors that may increase load on the ankle complex.
Extension of the big toe to 60 to 65 degrees is needed to create a rigid lever for the foot, which is important for gait propulsion.9 If a patient does not have this range, a common compensatory mechanism is to externally rotate the hip during the big toe push-off phase of gait, thereby increasing the load on the medial tendons of the foot (e.g. tibialis posterior, flexor hallucis longus, flexor digitorum longus).
Functional tests are helpful in identifying any asymmetries and global movement patterns that can contribute to pathology.9 It is important to assess the gait, single-leg squats, single-leg calf raises and knee-to-wall ankle mobility (see below).
Gait
Antalgic movement patterns can reflect pain avoidance from a current injury or adapted movement patterns from a previous injury.
Assess arch position and control. Arch types include neutral, planus (flat foot) and cavus (high arch). Check if the arch collapses or remains rigid. A rigid arch can decrease shock absorption and increase the load on the plantar fascia.
Single-leg squats
Assess global balance. Look for the Trendelenburg sign with respect to the presence of a contralateral hip drop. This implies proximal weakness, which can increase the distal load.6
Single-leg calf raises
The patient should aim for 10 single leg repetitions. Observations to be made include the Trendelenburg sign, height of the ankle, inversion and eversion of the ankle, and whether there is reproduction of pain.
If there is a significantly reduced height of the ankle, consider tibialis posterior weakness, an Achilles tendon tear or plantar fasciitis.
Knee-to-wall test
The knee-to-wall test (Figure 3) assesses how much dorsiflexion a patient has in their ankle, which is relevant to activities such as walking down stairs and inclines. While the patient keeps their heel flat on the ground, ask them to bend their knee to touch the wall. Keep moving their foot further back until they have pain, or until they lift their heel off the floor. Measure the distance from the wall to the big toe. A functional range is more than 9 cm. A decreased range may indicate a higher risk of sustaining a lower extremity injury.10
{kind=link}
Special tests
The Simmonds–Thompson test is used to assess the integrity of the Achilles tendon. It involves passively squeezing the gastrocnemius muscle and observing for the presence of corresponding ankle plantarflexion. If this does not occur, an Achilles tendon tear needs to be considered.
Passive end-range ankle plantarflexion with overpressure will identify whether there is a posterior impingement.
Tinel’s sign is used to assess nerve compression (e.g. tibial nerve). It involves percussion of the nerve four to six times to elicit paraesthesia.
Investigations
Most cases of heel pain can be diagnosed clinically. If symptoms are atypical or persist beyond the expected time frame, further investigation and referral may be required.
If a systemic aetiology is suspected, blood tests that may be useful include those for inflammatory markers (e.g. C-reactive protein, erythrocyte sedimentation rate) and genetic markers (e.g. HLA-B27).
If a stress fracture is suspected, a plain x-ray should be ordered in the first instance. If a fracture is not identified but the suspicion remains high, a CT or MRI scan may be considered.11 Although often not required, ultrasound may be useful in confirming plantar fasciitis and heel fat pad atrophy.11 MRI scans may be useful in diagnosing tarsal tunnel syndrome, stress fractures and tumours, but are most useful in identifying the more common condition of tibialis posterior tendon dysfunction, which presents with a painful flat foot.11
Differential diagnoses
Plantar fasciitis
Plantar fasciitis is the most common cause of heel pain in adults.2,12 The plantar fascia is a band of dense connective tissue that extends from the ball of the foot to the calcaneal tuberosity. It supports the arch of the foot, and aids with foot propulsion and shock absorption. Injuries are caused by an increase in intrinsic and extrinsic loads. Intrinsic factors may include excess weight, pes planus, excessive pronation and degenerative changes such as increased stiffness of the plantar fascia and heel fat pad atrophy. Extrinsic factors include inappropriate footwear, overuse in training and poor training technique.13
Plantar fasciitis is often characterised by pain on taking the first steps of the day, or on standing from a seated position.2 Pain can be provoked with palpation of the medial process of the calcaneal tuberosity and along the plantar fascia.2,14
The management of plantar fasciitis is discussed in more detail below. The prognosis is favourable, with more than 80% of patients having symptom resolution within one year.15
Achilles tendinopathy
The Achilles tendon is the combined tendon of the gastrocnemius and soleus muscles, and attaches distally onto the calcaneus.14 Pain can occur during or after activity, and tends to worsen with increasing physical activity or application of pressure to the area.14 Intrinsic factors include male sex, older age, excess weight, steroid use, fluoroquinolone use, hypertension, diabetes and inflammatory arthropathies. Extrinsic factors include inappropriate footwear, overuse in training and poor training technique.12
Noninsertional Achilles tendinopathy responds more favourably to conservative measures than insertional Achilles tendinopathy.2 The management of Achilles tendinopathy is discussed in more detail below. The prognosis is favourable, with 84% of patients having full recovery of their activity levels, and 94% of patients being asymptomatic at 8 years of follow up.13 However, 41% of patients report symptoms of overuse in their uninvolved Achilles tendon, highlighting the importance of early intervention to prevent compensatory patterns.13
Fat pad atrophy
The fat pad of the heel, composed of tightly packed columns of adipose tissue, serves as a shock absorber.11,12 The pain of fat pad atrophy tends to be deep and diffuse, involving much of the weightbearing region of the calcaneus.12,14 Contributing factors may include older age, excess weight, trauma and previous steroid injections.2,14 The underlying bone may be palpable in extreme cases.2 Management strategies include rest, icing, footwear modification and heel cups.2,11,14
Posterior tibial nerve entrapment (tarsal tunnel syndrome)
The tarsal tunnel refers to a compartment beneath the flexor retinaculum.2,14 Entrapment of the tibial nerve in the tarsal tunnel causes neuropathic pain in the posteromedial ankle and heel.2,11,12,14 This can occur for a variety of reasons, including pes planus, trauma, space-occupying lesions and systemic disease.2,12,14 Pain can be provoked with percussion (Tinel’s sign) or compression (dorsiflexion and eversion of the foot) of the tibial nerve.2,12,14 Although tarsal tunnel syndrome is uncommon (unlike the very common carpal tunnel syndrome), it may be secondary to a ganglion compressing the neurovascular bundle. In this situation, an MRI scan is the preferred initial investigation. Electrophysiological studies can be useful in confirming the diagnosis.11,14 Management strategies include activity modification, footwear modification, arch supports, NSAIDs and steroid injections.11,14 If conservative measures fail, surgical intervention may be considered.11,14
Inflammatory arthropathies
Most cases of heel pain have a biomechanical aetiology. If patients have symptoms that are atypical or persist beyond the expected time frame, concomitant arthralgias, or are symptomatic in the heels bilaterally, they may have an inflammatory arthropathy. Referral to a rheumatologist is recommended to assess for conditions such as psoriatic arthritis, reactive arthritis, rheumatoid arthritis and gout.
Management of plantar fasciitis and Achilles tendinopathy
The transition of a tendon from normal to pathological can be conceptualised as a continuum of three overlapping stages: reactive tendinopathy, tendon dysrepair and degenerative tendinopathy (https://bjsm.bmj.com/content/43/6/409.full).16 The approach to management differs depending on where the patient is on this continuum.
Reactive tendinopathy
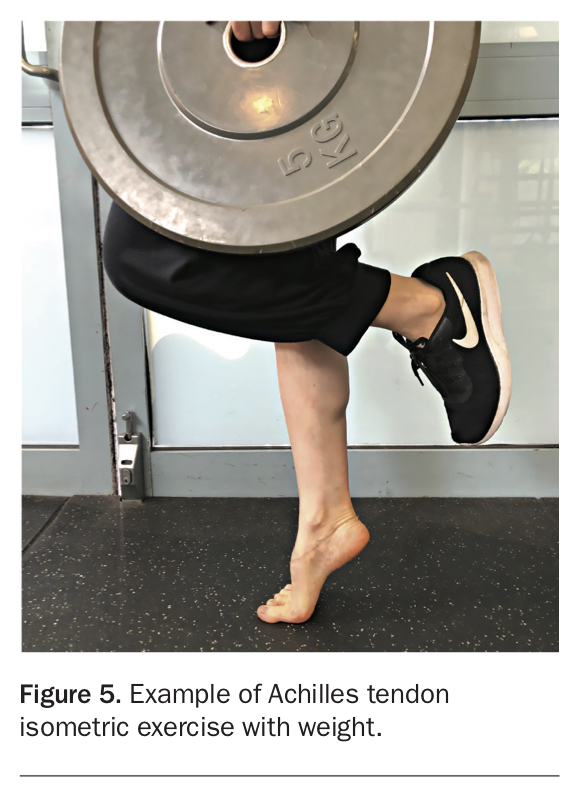
In acutely overloaded tendons, there is a noninflammatory proliferative response of the tendon cell and matrix.14 This leads to short-term tendon thickening.14 As pain is often heightened, interventions are targeted at relieving it. These include temporarily reducing acute loads, strapping, supportive footwear, NSAIDs, intrinsic exercises (Figure 4) and isometric exercise training (Figure 5). Stretching of the calf is no longer recommended in acute reactive Achilles tendinopathy due to the compressive load on the tendon. Manual release of the calf is recommended for both plantar fasciitis and Achilles tendinopathy. Heel cushions can be helpful for patients who have pain on heel strike in the context of plantar fasciitis. Heel lifts can serve to reduce stress on an acutely irritable Achilles tendon. Although steroid injections may be beneficial in reducing pain, adverse outcomes such as tendon atrophy, tendon rupture and decreased tendon strength have been reported.14 Thus, steroid injections should only be used with great caution. Weight loss should be encouraged in patients who are overweight.
{kind=link}
{kind=link}
Tendon dysrepair
Chronically overloaded tendons undergo a process of cell activation, leading to disruption of the extracellular matrix.3 There may be some reversibility through load management and exercise therapy (e.g. eccentric exercise training, heavy load training).15 Referral to a physiotherapist or an exercise physiologist to provide guidance through an appropriate exercise program is recommended.
Degenerative tendinopathy
If treatment is not given, a degenerative tendinopathy can arise. This occurs in the context of significant collagen disorganisation and cell death, which is irreversible.3 In such patients, rehabilitation is geared towards a progressive tendon loading program for the remaining nondegenerative fibres, and addressing any weaknesses in the global movement chain. If conservative measures fail, surgical intervention may be considered.17
Conclusion
Heel pain is a common presentation. Although there are a variety of underlying aetiologies, a thorough history and examination will usually lead to a diagnosis. Overall, the prognosis is favourable. If the case is complex or if there is suggestion of an underlying inflammatory arthropathy, referral to a rheumatologist is recommended. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.