Fibromyalgia. Diagnosis and management in general practice

Fibromyalgia
Fibromyalgia syndrome is a prevalent and high-impact condition, characterised by a phenotype of widespread pain, fatigue, sleep disturbance and cognitive problems. A safe and accurate diagnostic approach, with exclusion of clinically important mimics, and an individualised multimodal framework for management are essential to optimising the care and outcomes of patients in the primary care setting.
- Fibromyalgia is commonly encountered in general practice and affects between 2 and 8% of the population worldwide.
- Abnormal processing of sensory information by the central nervous system results in symptoms including widespread pain, fatigue, sleep disturbance and cognitive problems.
- Diagnosis is based on the identification of typical clinical features and rational investigation for mimicking disorders and comorbid disease as guided by individual clinical assessment.
- Education, exercise and psychological strategies are the cornerstones of management, with drugs targeting pain modulatory mechanisms being useful adjuncts.
- Primary care is an ideal setting to initiate and co-ordinate a multimodal and tailored management strategy for patients with fibromyalgia, review progress and provide ongoing support.
Fibromyalgia is a common chronic pain syndrome associated with significant morbidity and societal impact.1,2 It affects between 2 and 8% of the population worldwide and is more common in women and those with other chronic illnesses.3,4 The most characteristic feature of fibromyalgia syndrome is widespread pain and tenderness, often accompanied by extreme fatigue, poor-quality sleep, cognitive dysfunction and psychological distress.
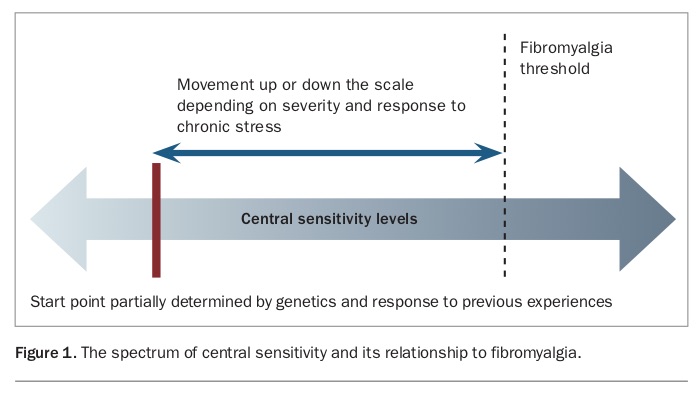
This constellation of symptoms occurs due to alterations in sensory processing pathways in the nervous system, changes collectively referred to as ‘central sensitisation’.5 Central sensitisation is a spectrum (Figure 1) with sensitivity varying between individuals and even within an individual over time. Patients with fibromyalgia develop excessive central sensitivity, resulting in normally non-noxious stimuli being amplified and experienced as painful or unpleasant. Fibromyalgia is therefore also associated with related conditions associated with sensory amplification, including irritable bowel syndrome, chronic headache, restless legs syndrome, multiple chemical sensitivities and autonomic dysfunction.
{kind=link}
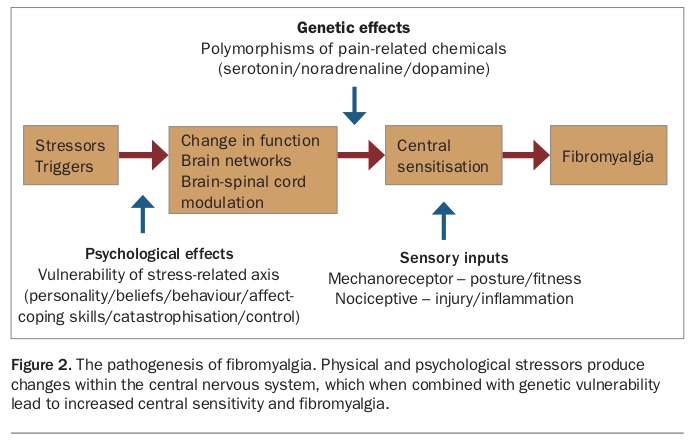
Our understanding of the pathogenesis underlying fibromyalgia and the development of central sensitisation is evolving. Genetic susceptibility and familial associations are well recognised, and up to 50% of an individual’s risk may be attributable to genetic factors, such as polymorphisms that affect neurotransmitter function.6 Additional environmental and personality factors affecting responses to physical and psychological stress augment this predisposition to increased central sensitivity,7 and in most patients, a defined triggering event (e.g. medical illness, trauma or psychological stress) can be linked to the onset of overt fibromyalgia.8 Abnormalities of sensory processing occur in the brain, spinal cord and periphery and involve dysfunction of neurotransmitters such as serotonin and noradrenaline, dysregulated central hormonal axes and neurogenic inflammation.9 The pathogenesis of fibromyalgia is summarised in Figure 2.
{kind=link}
Diagnosis
Recognition of the characteristic phenotype of fibromyalgia is important in primary care, because diagnosis is often delayed.10 Establishing a diagnosis of fibromyalgia not only allows the initiation of targeted management, but also leads to improved symptoms and reduced costs and healthcare utilisation.11,12
Although fibromyalgia can exist as a stand-alone condition, it is commonly comorbid with other chronic diseases. For example, studies have found rates of fibromyalgia to be as high as 41% in patients with rheumatoid arthritis, 18% with type 2 diabetes and 22% in those with chronic heart failure.13-15 Psychiatric diagnoses are often also comorbid; about one in five patients with fibromyalgia meet criteria for major depressive disorder and similar rates of comorbid bipolar disorder also exist (about 20%).16,17
Therefore, the diagnosis of fibromyalgia does not preclude the presence of other clinically important illnesses, nor does the presence of another disease discount a diagnosis of fibromyalgia. Fibromyalgia is not a diagnosis of exclusion.18 It should be formally diagnosed and managed alongside other comorbidities and while additional investigations or specialist evaluation are pending.
Diagnostic approach
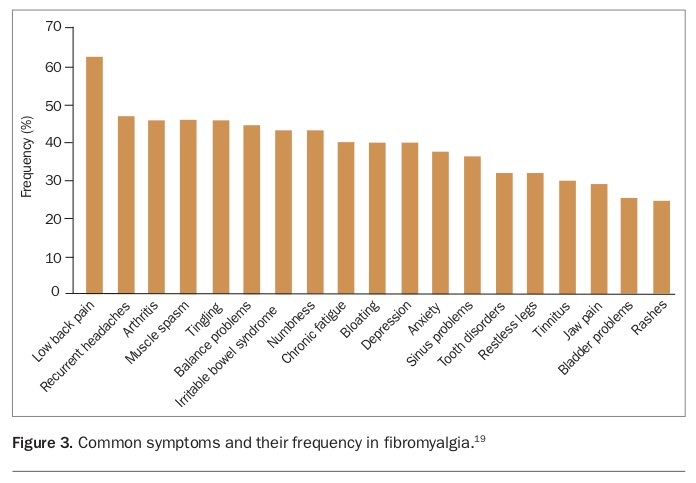
Fibromyalgia should be considered in any patient with widespread muscular pain. Other commonly reported symptoms include fatigue, joint pains, headaches, restless legs, numbness or paraesthesias, sleep disturbance and impaired memory or attention. Rates of commonly associated symptoms among patients with fibromyalgia are shown in Figure 3.19
{kind=link}
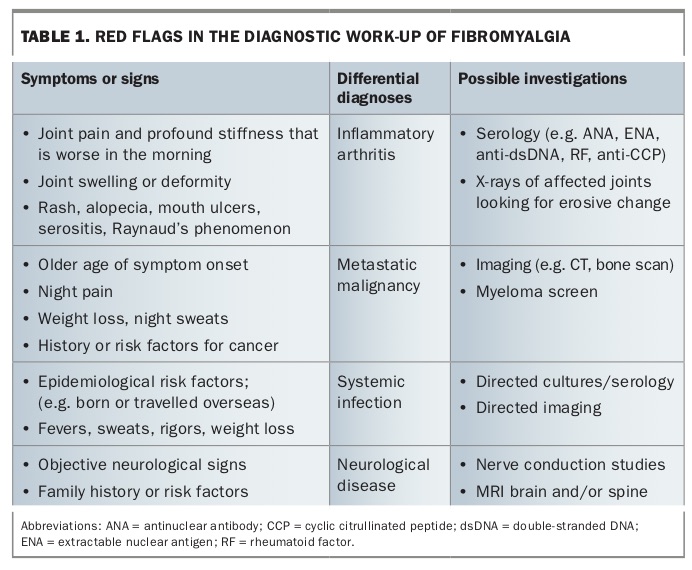
There is no single diagnostic test for fibromyalgia, and the diagnosis is established on the basis of typical clinical features and the exclusion of mimicking disorders with rational investigations directed by clinical assessment. Initial work-up of the patient should include a careful history and detailed clinical examination, focussing on other causes of widespread muscular pain. Important conditions that can mimic fibromyalgia clinically include inflammatory arthritis and connective tissue diseases, mechanical musculoskeletal problems, hormonal disorders (e.g. thyroid dysfunction, menopause), metastatic malignancy and persisting viral infections. Some examples of red flags that should prompt consideration of alternative diagnoses and further investigation are listed in Table 1.
{kind=link}
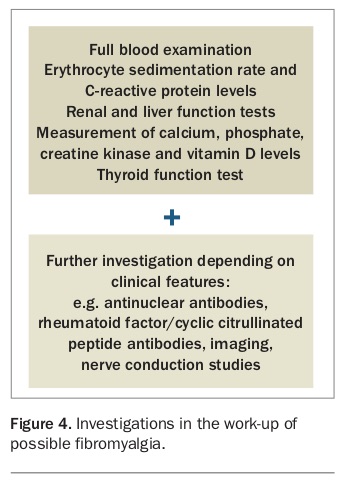
In addition to the clinical assessment, a basic panel of investigations is also indicated to exclude common abnormalities that can confound or worsen symptoms of fibromyalgia. This should include a full blood count, basic biochemistry (including electrolytes, renal and liver function), thyroid function tests, and measurement of inflammatory marker, muscle enzyme and vitamin D levels. Additional testing should be performed as guided by clinical suspicion (Figure 4).
{kind=link}
Diagnostic criteria and symptom scores
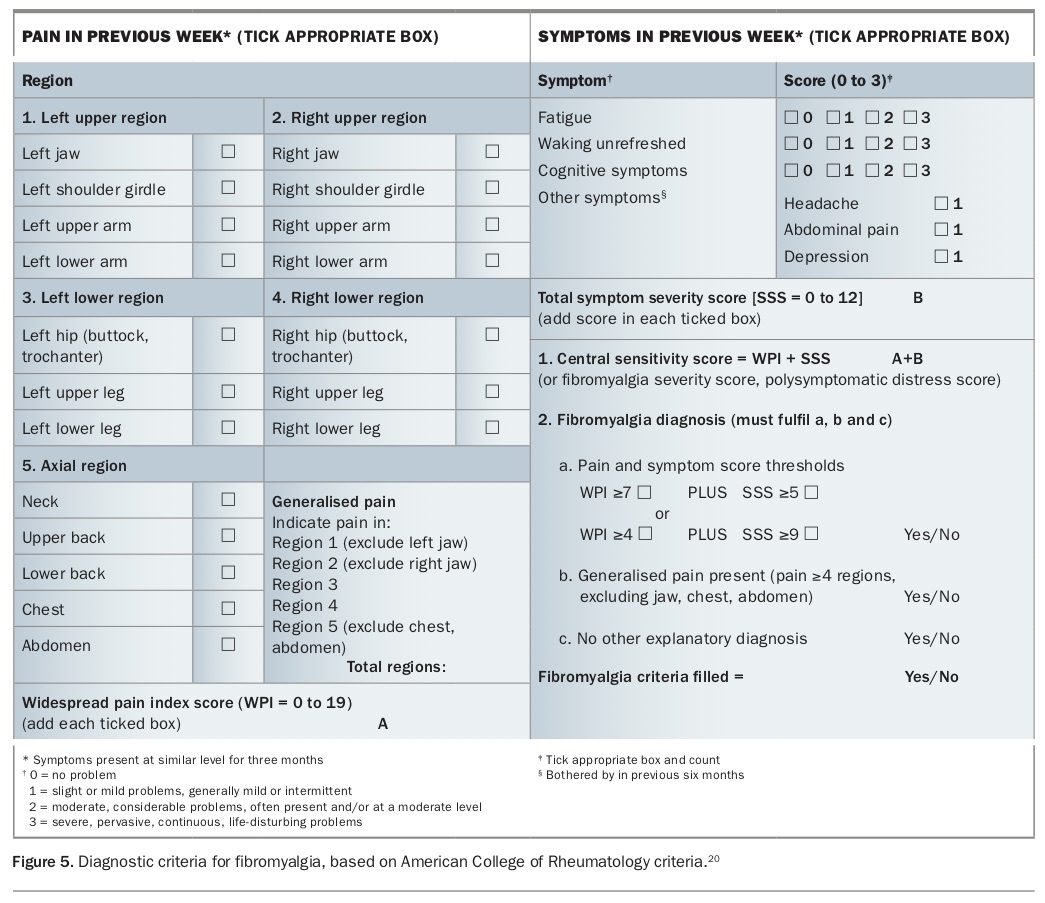
The American College of Rheumatology has developed criteria for fibromyalgia,20 which may be of aid in the diagnostic process, including in primary care (Figure 5). It includes a self-report of the number of painful regions over the past week (widespread pain index [WPI]) plus an assessment of central sensitivity symptoms (symptom severity score [SSS]), which include fatigue, sleep disturbance, cognitive symptoms, abdominal pain, headache and depression.
{kind=link}
Diagnostic criteria for fibromyalgia are met if the following are fulfilled:
- generalised pain in at least four of five regions (not jaw, chest or abdomen)
- symptoms present at a similar level for at least three months
- WPI of seven or more (maximum 19) and SSS of five or more (maximum 12) or WPI of four to six and SSS of nine or more
- a diagnosis of fibromyalgia is valid irrespective of other diagnoses.
Fibromyalgia symptom score
The WPI and SSS can be added to produce the fibromyalgia severity score (FSS), with most patients with fibromyalgia having a FSS of 12 or more. Given fibromyalgia symptoms exist on a continuum, the FSS can also be considered to be an assessment of fibromyalgia activity or degree of central sensitivity in an individual patient at a particular point in time. Therefore, in addition to diagnosis, this tool may potentially help track fibromyalgia activity in affected individuals, aiding disease monitoring over time. The WPI and SSS have replaced the previous use of tender points in the current fibromyalgia diagnostic criteria; however, these tender points are still useful in the clinical assessment of fibromyalgia.
Nonpharmacological management
There is no single treatment for fibromyalgia and effective management requires a multimodal and holistic approach, considering an individual patient’s symptom profile, treatment priorities and reversible factors exacerbating disease. The aims of management are improvement in symptoms, function and quality of life.21 Best results occur with multidisciplinary management, which may include input from medical specialists such as a rheumatologist or pain specialist and allied health practitioners such as a psychologist or physiotherapist. The need for a co-ordinated approach and long-term support places the GP in an ideal position to build a strong therapeutic relationship and act as a central point of contact for patients with fibromyalgia.
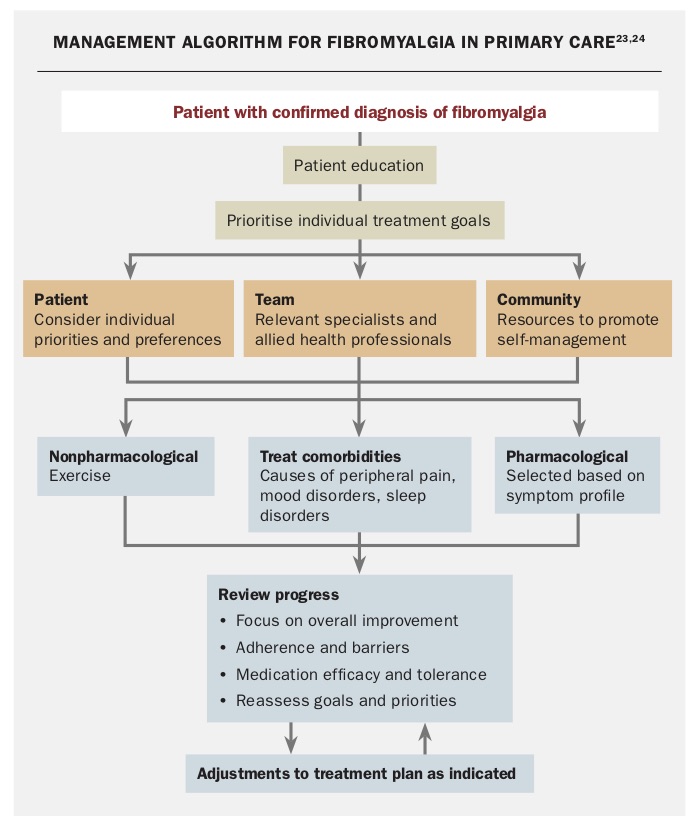
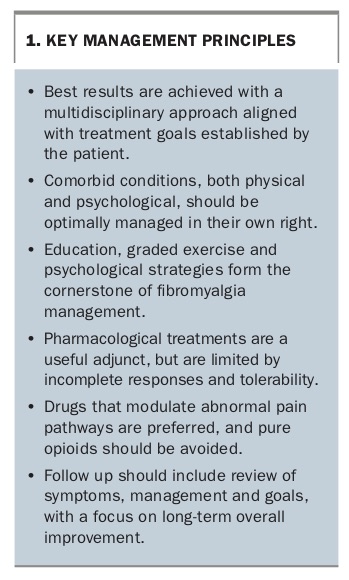
The mainstay of fibromyalgia management is nonpharmacological and includes education, graded physical activity and psychological interventions, ideally in combination.22 Some patients require the addition of pharmacological therapy for symptom management. Comorbid medical and psychiatric conditions that can exacerbate fibromyalgia should be identified and managed in their own right. The Flowchart outlines a recommended approach to management of patients with fibromyalgia and individual components of the management strategy are discussed in Box 1.23,24 These recommendations are in line with the most recent clinical guidelines, published in 2017 by the European League Against Rheumatism (EULAR).23
{kind=link}
{kind=link}
Education
Education is an essential first-line component of fibromyalgia management and should ideally include:
- discussion of the diagnosis and its underlying mechanisms
- management principles
- expected outcomes.
Family and significant others should be included in these discussions as appropriate. Similar to other chronic conditions, education in fibromyalgia aims to encourage understanding, acceptance and ownership over the disease and promote self-management,24 and has been shown to improve symptoms and functionality, particularly when combined with other nonpharmacological measures.25,26
Patients should be reassured that although the disease can be debilitating and responses to therapy only partial, it does not cause irreparable damage and is not intrinsically dangerous or degenerative. Patients should be encouraged to establish treatment priorities and goals, with an understanding that day-to-day fluctuations are to be expected, and that a realistic target is gradual overall improvement, not necessarily complete symptom elimination.
Several supplementary resources about fibromyalgia are readily available for both patients and healthcare practitioners (Box 2).
{kind=link}
Exercise
Exercise therapy is a well-studied, efficacious and widely accepted treatment modality in fibromyalgia.23 Both aerobic and resistance training, which may be land- or pool-based, have well-established benefits, including reducing pain, decreasing depressive symptoms and increasing overall improvement in wellbeing, function and quality of life.27 Activity should be built up very gradually over time, with a realistic aim being three to five sessions of 20 to 30 minutes per week. Many patients benefit from referral to a physical therapist or exercise physiologist for assessment and support in designing a tailored program, monitoring progress and maintaining motivation.
Psychological strategies
An individual’s psychological or emotional state and attitude towards pain can have a marked effect on central pain sensitisation. Psychological strategies should be focused both on managing underlying depression and anxiety, as well as promoting cognitive strategies for pain management. Formal psychiatric assessment and management of comorbid mental health diagnoses may also be required in some patients. Practical assistance for social issues that may be driving distress such as relationship, financial or work stressors should also be sought where possible.
Cognitive behavioural therapy (CBT) is the psychological intervention with the most robust evidence in fibromyalgia, with benefits demonstrated in reducing pain, depression and disability at both short- and long-term follow up.28 The most success is achieved with trained therapists and tailored programs. Other mind-body-based therapies including mindfulness, biofeedback and relaxation strategies may also be beneficial, although the available evidence for these techniques is of low quality.29
Pharmacological management
Although nonpharmacological approaches are the mainstay of fibromyalgia management, some patients require the addition of pharmacological agents to achieve adequate symptom control. Preferred drugs are those that specifically target dysregulated central pain pathways, and the choice is individualised based on troublesome symptoms (e.g. pain, poor sleep, anxiety), side effect profile and potential drug interactions.
The efficacy of pharmacological strategies are traditionally summarised by the 30/50 rule: about 30% of patients achieve 50% improvement in pain and about 50% achieve 30% improvement, with the remaining 20% obtaining less benefit. Use of typical agents and dose escalation is often limited by side effects, especially nausea, dizziness, drowsiness or cognitive dulling. Patients may need to trial multiple drugs before finding one that is helpful and tolerable. An adequate therapeutic trial with gradual dose incrementation is recommended. Combination therapy is useful in some patients, but there is limited guiding evidence.30
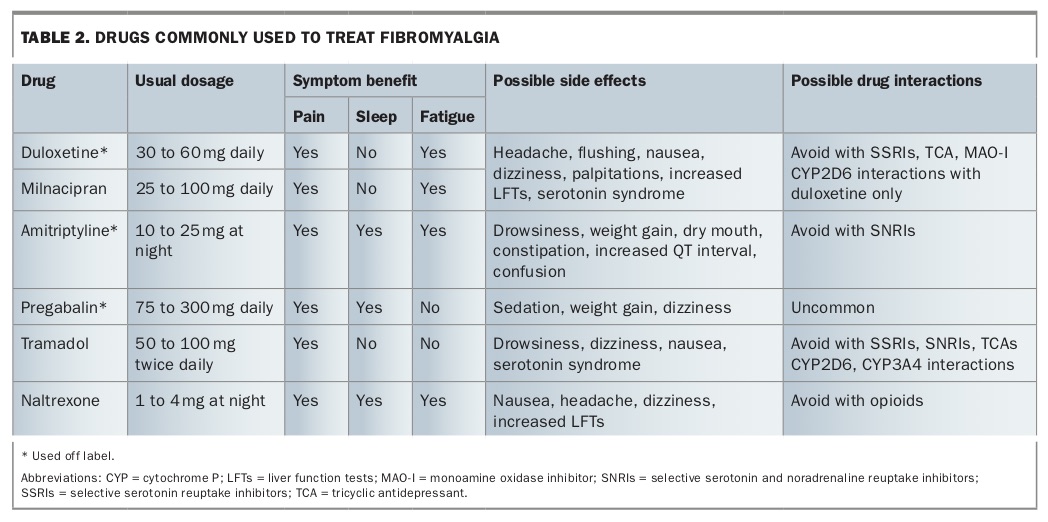
Specific medications used in fibromyalgia that are currently available in Australia are discussed below and summarised in Table 2.
{kind=link}
Serotonin and noradrenaline reuptake inhibitors
The serotonin and noradrenaline reuptake inhibitors (SNRIs) duloxetine (off-label use) and milnacipran have evidence for benefit when used in fibromyalgia. Fibromyalgia is associated with reduced functioning of serotonin and noradrenaline pathways in the central nervous system and SNRIs, which target these reduced neurotransmitter levels, have been shown to have modest benefits in improving pain and function.31 In a meta-analysis of randomised trials of duloxetine, the number needed to treat for significant pain reduction was eight,32 with similar response rates seen for milnacipran.33 SNRIs may also benefit those patients with concurrent anxiety or depressive symptoms.34 It should be noted that SNRIs and selective serotonin reuptake inhibitors (SSRIs) are not necessarily interchangeable in fibromyalgia, and SNRIs are preferred due to greater evidence.23
Tricyclic antidepressants
Amitriptyline (off-label use) also acts via modulation of serotonin and noradrenaline. In fibromyalgia, low doses of amitriptyline have modest benefits in reducing pain with a number needed to treat as low as 3.54.35 It may be particularly beneficial in those with sleep disturbance, and has also shown some effect in improving fatigue.36 Side effects of amitriptyline, particularly sedating effects, can be limiting. Nortriptyline (off-label use) is an alternative tricyclic antidepressant, with fewer studies being performed in patients with fibromyalgia.
Gabapentinoids
Pregabalin (off-label use) is commonly prescribed in multiple pain syndromes, and exerts its effect by binding to calcium channels in the central nervous system. In fibromyalgia, it has modest benefits for reducing pain and improving sleep in particular, but less effect on reducing fatigue.34 Gabapentin (off-label use) has similar mechanisms to pregabalin and is cheaper, but requires dosing three times daily and is less well studied than pregabalin in patients with fibromyalgia.23
Tramadol
Tramadol is a weak opioid with additional serotonin and noradrenaline reuptake inhibition. A small body of evidence supports its use in fibromyalgia, particularly for reduction of pain.23 Prescribers should be aware of potential drug interactions and risk of serotonin syndrome.
Tapentadol
Like tramadol, tapentadol has a dual mechanism of action as both an opioid agonist and a noradrenaline reuptake blocker, with minimal serotonergic activity. In chronic musculoskeletal pain, tapentadol has a demonstrated analgesic effect; however, there are limited data specific to its benefit in fibromyalgia.37
Naltrexone
Small studies of naltrexone, an opioid antagonist, have shown reduction in pain compared with placebo in 20 to 30% of patients.38 Formulation requires a compounding pharmacist and larger controlled trials are required before naltrexone can be recommended for routine use in fibromyalgia.
Analgesics and anti-inflammatories
Although commonly used for pain as a first-line treatment, analgesics such as paracetamol and NSAIDs have limited evidence of benefit in fibromyalgia.39 Similarly, glucocorticoids such as prednisolone have no efficacy over placebo, and come with significant risk of side effects.40 Therefore, they should not be used in patients with fibromyalgia unless a comorbid indication exists.
There is also no role for the prescription of opioids for fibromyalgia, given a lack of efficacy and evidence of significant harm.41 Longitudinal studies have shown worse outcomes in terms of pain, function and quality of life in opioid users with fibromyalgia. This is likely to be due to numerous side effects, risk of dependence and opioid-induced hyperalgesia, which can worsen rather than improve pain in this population.42
Cannabinoids
Significant public interest in the role of cannabinoids in chronic pain has emerged in recent times, and their role in fibromyalgia is under evaluation. Currently, there is insufficient evidence to recommend cannabinoids in routine practice. This is consistent with the most recent position statements published by the RACGP, the Australian Rheumatology Association (ARA) and the TGA.43-45
Complementary medicines
Several complementary treatment modalities have been investigated in patients with fibromyalgia, but studies in this area are fraught with methodological and blinding difficulties, making recommendations for or against most of these modalities difficult.23 One exception, however, is a recent prospective trial of tai chi, which found similar or greater improvement in symptoms when compared with aerobic exercise.46 Several trials of acupuncture have also shown a moderate improvement in pain when added to standard therapy,47 whereas the evidence for massage, hypnosis and nerve stimulation is less robust.23
Patients who wish to pursue alternative therapies should be encouraged to combine these with management strategies of established benefit.
Conclusion
Fibromyalgia is a high-impact disorder, frequently encountered in general practice. GPs should be cognisant of the characteristic features of fibromyalgia, to facilitate early diagnosis and institution of an individualised multimodal management strategy including a combination of educational, physical, psychological and pharmacological interventions. MT