Fibromyalgia: small steps on a long journey
Although much is still unknown about fibromyalgia, its appropriate diagnosis and multimodal treatment strategies offer some hope for patients in developing good self-management of their symptoms and preserving function.
Fibromyalgia is a disorder that acquired its current name 50 years ago, although it has existed for centuries with different labels.1 It is the second most common rheumatological condition (behind osteoarthritis) with a prevalence of between 2% and 8% and can occur at any age and in diverse ethnic groups.2,3 Despite this, it has remained a topic of controversy with contested views on its clinical diagnosis, pathophysiology and treatment methods.4
Setting these contentions aside, the burden of fibromyalgia is profound and far-reaching. For the individual, fibromyalgia is associated with worse functioning, greater disability and loss of healthy years of life compared with nonaffected controls.5 The financial costs of fibromyalgia are also considerable, derived from loss of workforce and healthcare utilisation.6
Although our understanding of fibromyalgia continues to grow, its management can be challenging, particularly in patients who have symptoms on the more severe end of the spectrum of this disorder. As with other chronic conditions, such as diabetes mellitus, the GP has a central role in the longitudinal management of fibromyalgia. Key elements of this in primary care include early diagnosis, development of a long-term therapeutic relationship, a collaborative approach to lifestyle modification and goal setting, and co-ordination of a network of multimodal healthcare providers.
Pathophysiology
The pathophysiological underpinnings of fibromyalgia are complex and a matter of ongoing investigation. It is considered to be a centralised pain syndrome characterised by heightened sensitivity of central nervous system (CNS) mechanisms for processing sensory inputs, resulting in an experience of pain in settings that might otherwise be considered innocuous. It is theorised that this may represent an abnormally prolonged activation of a global stress response that in physiological circumstances is meant to protect against threats to homeostasis.7 Both functional MRI and cerebrospinal fluid studies (for example, demonstrating raised levels of substance P and glutamate) have shown quantifiable organic changes suggestive of neuroinflammation of the CNS in patients with fibromyalgia.8-10
The pain experience in fibromyalgia does not end with maladaptive central sensitivity. Alterations in posture and gait, as well as fear avoidant behaviours and deconditioning as a result of pain, predispose patients with fibromyalgia to secondary musculoskeletal injury such as bursitis and tendinopathies that, in turn, can contribute to a more severe pain experience.11
Clinical manifestations
The clinical culmination of these pathological pathways is widespread nociplastic pain, referring to pain experienced in the absence of ongoing tissue or nerve damage. This can be diffuse, concentrated in specific locations or migratory and is often characterised by both hyperalgesia (a heightened sense of pain in response to a nociceptive stimulus) and allodynia (the sensation of pain from non-nociceptive sensory inputs).2 Although fibromyalgia pain is typically musculoskeletal, it can overlap with other painful conditions such as chronic headache, abdominal pain or pelvic pain.12 Sometimes these precede the diagnosis of fibromyalgia or they may develop as a particular feature during the course of the condition.13
Fatigue is also a prominent feature of fibromyalgia and can have physical, emotional and social manifestations.14 Although fibromyalgia and chronic fatigue syndrome share many characteristics, they are overall thought to be separate conditions mechanistically and in clinical presentation, with the latter involving fatigue (especially postexertional fatigue) as the central factor limiting function.15
Sleep disturbance affects more that 90% of patients with fibromyalgia and involves more than just insomnia, also manifesting as frequently interrupted or nonrefreshing sleep, or both, even with normal or prolonged duration.16
A common and bothersome manifestation of fibromyalgia is cognitive change, often referred to as ‘fibro-fog’. Although this can take many forms, it typically involves impaired concentration and attention as well as poor memory.17 Other neurological manifestations can include sympathetic hyperactivity, resulting in tremor, tachycardia and flushing, as well as heightened sensitivity to bright lights, loud sounds or noxious smells.18,19 Mood disturbance and depressive symptoms occur often in patients with fibromyalgia and a concurrent diagnosis of major depressive disorder may be made.20 The culmination of these neuropsychiatric symptoms can be distressing and may have a profound impact on everyday functioning.
Diagnosis
With such nonspecific clinical manifestations, the diagnosis of fibromyalgia can initially appear difficult to make. In most cases, however, clarifying the diagnosis is associated with lessening of symptoms, improved health satisfaction and a decrease in healthcare costs from excess medical appointments, overinvestigation and unnecessary medications.21,22 With this in mind, it is unfortunate that the time to diagnosis for patients with fibromyalgia is often several years and is longer in those who are younger and have other potentially obscuring comorbidities such as migraine.23
The elicitation of ‘tender points’, which formed the basis of the 1990 American College of Rheumatology (ACR) classification criteria for fibromyalgia, is no longer part of the formal diagnostic criteria. Instead, the 2011 ACR Fibromyalgia Survey Questionnaire uses a patient-reported questionnaire to assess the presence of widespread pain as well as the severity of common fibromyalgia symptoms and any associated conditions. The latest iteration of this is the 2016 revision that integrates both patient- and physician-based criteria and delineates fibromyalgia from other regional pain disorders (Table 1).24
{kind=link}
Importantly, the diagnosis of fibromyalgia is considered valid irrespective of other diagnoses, and is therefore no longer a ‘diagnosis of exclusion’. Although it often coexists with other chronic conditions, its symptoms should be identified and managed on their own merits. Blood tests or imaging studies are not needed for the diagnosis of fibromyalgia and unless clinically indicated for the investigation of other conditions, these may be unnecessary and better avoided.
Prognosis
Few studies have involved long-term follow up of patients with fibromyalgia. However, it may be of some reassurance that even though fibromyalgia is often a chronic condition that may not self-resolve, it is not one of inexorable decline. Symptoms fluctuate around a relatively stable baseline and with time may even show some improvement.25,26
Management
Patient education
Patient education and engagement in self-managing fibromyalgia have a fundamental role in management, with particular importance placed on highlighting the concept of central sensitisation rather than peripheral nociception as the target of many treatment modalities.27 Each patient should be assessed initially to identify a baseline, measured by their ability to perform activities of daily living, allowing a longitudinal approach to monitoring outcomes and identifying exacerbating stressors.
There is a spectrum of symptom severity in fibromyalgia and patients on the milder end of this may experience sufficient benefit from simple interventions. Patients with more severe fibromyalgia, however, are likely to have persisting symptoms with episodic exacerbations. They are more likely to need ongoing multimodal management strategies.
All current guidelines emphasise improved quality of life, functional ability and symptom reduction as goals of care for patients with fibromyalgia. It is important to frame individual expectations and realistic outcomes within this context (for example, aiming for 30% reduction rather than complete resolution of pain).28 Online pain neuroscience education has been shown to be effective in improving patients’ knowledge of their condition, health outcomes and anxiety symptoms.29 One such reliable e-resource often used and readily accessible for patients is The University of Michigan Chronic Pain and Fatigue Research Center Fibroguide (https://fibroguide.med.umich.edu).
Nonpharmacological management
Nonpharmacological interventions form the backbone of fibromyalgia management, involving regular graded exercise, mindfulness techniques, cognitive behavioural therapy (CBT) and good sleep hygiene. Both aerobic exercise and resistance training have been associated with improvements in pain and function. Movement and flexibility practices such as tai chi, yoga and Pilates may also be helpful and often integrate relaxational and meditative practices with additional psychological benefits.30 Overall, encouraging graded exposure to regular exercise by developing an individualised and sustainable regimen is a practical approach that can be empowering for patients. It is important, however, that patients are aware of the risk of overexertion in a single exercise episode; consistency rather than intensity is the goal. Mindfulness-based stress reduction has been shown to improve symptom severity and coping mechanisms.31
CBT is useful to support patients to better understand, identify and adjust psychological and behavioural patterns that can be counterproductive.27 The development of sustainable coping skills such as distraction, relaxation and visual imagery from CBT with psychologist guidance significantly reduces pain catastrophising in patients with fibromyalgia.32
Optimisation of quality of sleep is important in managing fibromyalgia, with reinforcement of regular sleep schedules and good sleep hygiene, such as minimising screen time before bed, which may be aided by the regular exercise and meditative practices mentioned above. An Australian e-resource with patient-friendly information on sleep hygiene in general can be found at www.sleephealthfoundation.org.au/fact-sheets.html under the title ‘Good Sleep Habits’.
Pharmacological management
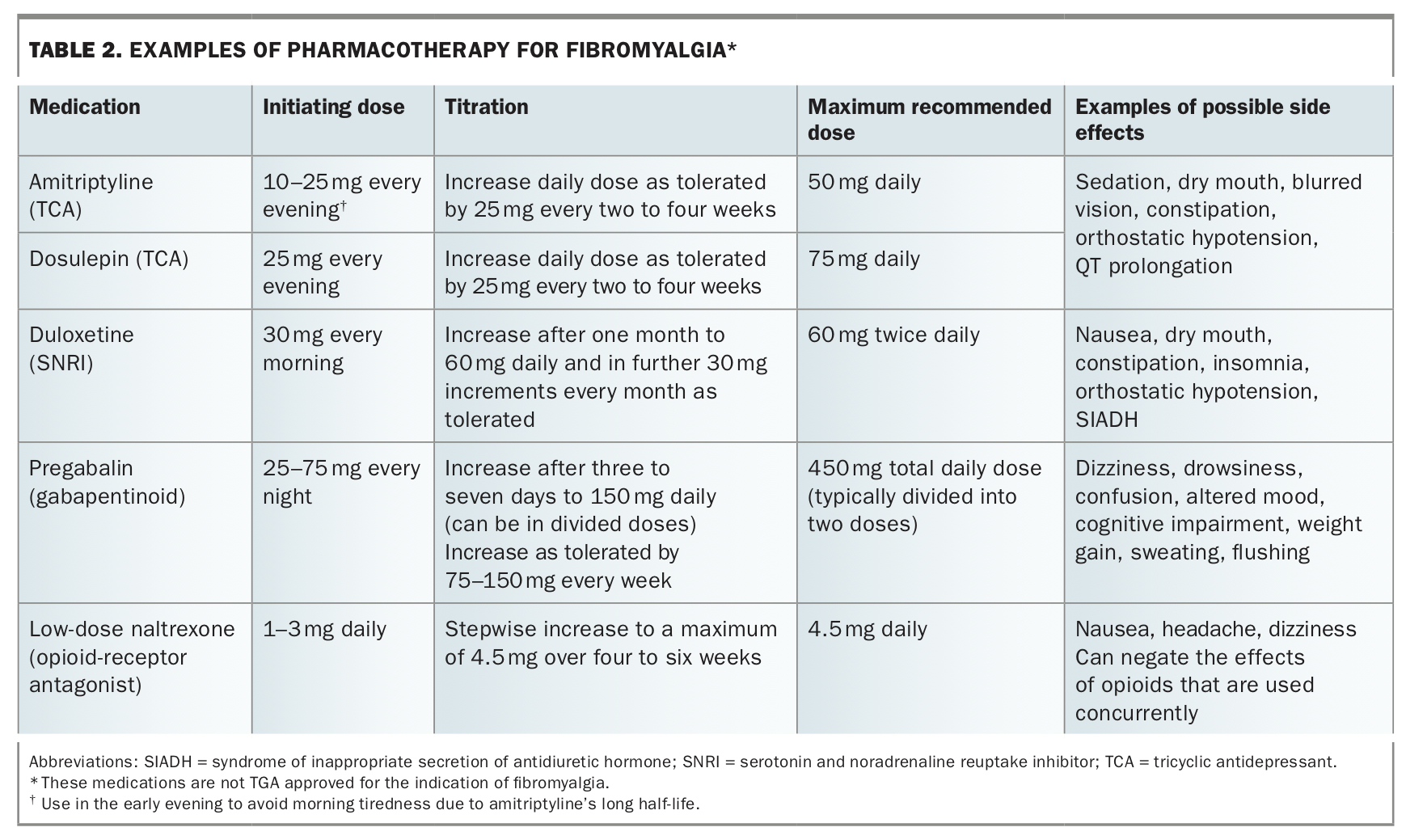
Pharmacotherapy in fibromyalgia tends to provide only modest benefit and should mainly be used to supplement, enhance and enable nonpharmacological interventions. Ideally, it should be a short-term intervention designed to reduce the impact of somatic symptoms, enabling greater focus on self-management and function. Table 2 summarises commonly used medications for fibromyalgia, although none of these are TGA approved for this indication.
{kind=link}
Tricyclic antidepressants (TCAs) such as amitriptyline and dosulepin, used in low doses, are often tried as first-line pharmacotherapy in fibromyalgia and have some evidence for effectiveness in terms of pain reduction compared with placebo.33 In practice, the reduction in pain is often small but additional sleep benefits and relative lack of major adverse effects at low doses make TCAs an attractive first-line option for many patients.
Duloxetine, a serotonin and noradrenaline reuptake inhibitor (SNRI), has been shown to reduce pain compared with placebo, with about eight patients needing to be treated (number needed to treat; NNT) for one to experience benefit of at least 50% pain reduction.34 However, SNRIs can be associated with adverse effects including nausea, sleep disturbance, weight gain and orthostatic hypotension with a number needed to harm (NNH) of 14.35
Pure serotonin reuptake inhibitors (SSRIs) have not shown efficacy for fibromyalgia pain, although they may be used for comorbid depression.36
Studies assessing the use of pregabalin have shown the NNT is 12 for moderate pain benefit in one patient, with associated improvements in quality of life and function.37 However, adverse effects including drowsiness, dizziness and weight gain occur in up to 70% of patients taking pregabalin. CNS side effects including mood change and sedation can also occur (NNH of 7.4).37 To mitigate the latter and avoid interference with daytime function, most of the dose (approximately two-thirds) should be taken in the evening. Use of pregabalin should be slowly and carefully titrated, aiming to achieve and maintain the lowest effective dose. There is also growing concern about the abuse potential of pregabalin, with overuse, dependence and diversion being recognised as possible risks of prescription.38
Low-dose naltrexone may also reduce pain in fibromyalgia, potentially through anti-inflammatory pathways targeting neuroinflammation of the CNS separate to its mechanism of opioid-receptor antagonism. It is generally well tolerated but can negate the effects of concurrently used opioids. At the doses used for fibromyalgia (0.5 mg to 4.5 mg, which is significantly lower than those used in alcohol dependence), it needs pharmacy compounding.39
Commencement of any of these agents should involve gradual and monitored titration (Table 2), aiming for a dose that is efficacious and well tolerated. This may be less than the maximum recommended dose. There is currently no rigorous evidence to support the use of combination pharmacotherapy for fibromyalgia and consideration of this usually needs specialist guidance.40
Nonsteroidal anti-inflammatory drugs and opioids
Although nonsteroidal anti-inflammatory drugs (NSAIDs) are often used by patients due to ease of access, current evidence does not support their effectiveness for the symptoms of fibromyalgia. In light of this and with a risk of adverse effects (including gastrointestinal bleeding, increased cardiovascular risk and nephrotoxicity), NSAIDs are not typically recommended as long-term options for fibromyalgia.41 However, they may have a short-term role when combined with physical therapies for the management of concurrent inflammatory pain syndromes (for example, tendonitis or bursitis) that can exacerbate fibromyalgia symptoms.
Similarly, there has been no evidence from clinical trials to support the use of opioids in fibromyalgia. Longitudinal analyses have instead shown that patients with fibromyalgia who were not taking opioids had greater improvement in pain severity scores, function and depression severity than those using opioids.42 In addition to the recognised risks associated with opioids, use in this patient group may actually have a negative effect on fibromyalgia symptoms, correlating with significantly lower self-efficacy ratings and higher pain catastrophising scores. This may be due to opioid-induced hyperalgaesia, which mechanistically may reflect worsening of central neuroinflammation.43
Cannabinoids
Cannabis has generated much interest lately in the treatment of a wide variety of medical conditions including chronic pain and fibromyalgia. It is often tried by patients for their fibromyalgia symptoms, especially in places where marijuana use has been legalised.44 Although there are observational data alluding to a possible role for cannabis,45 data from randomised controlled trials (although scant) suggest that effects on pain and other symptoms are minimal and adverse effects common. Pending further data from high-quality randomised controlled trials, use of cannabinoids should not be encouraged in people with fibromyalgia.46
Complementary and alternative treatments
In common with other chronic diseases with limited effective treatment options, a broad spectrum of complementary and alternative therapies have been promoted to people living with fibromyalgia, including physical and psychological treatments and dietary and herbal supplements.47 There is marked variation in definition and classification of these; a discussion of each is beyond the scope of this review. However, it is salient to acknowledge that their use is highly prevalent, with one longitudinal study over 14 years suggesting that almost all patients (98.1%) had used some form of complementary therapy for their fibromyalgia symptoms.48 Therefore, an important component of a thorough fibromyalgia history is to ask patients about their use of these treatments.
Conclusion
Fibromyalgia remains a condition that is poorly understood in its pathophysiology, although its profound impact on patients, society and the healthcare system is undeniable. Its heterogeneity invites a nuanced engagement with individualised patient care and the recognition that, unfortunately, treatment options are still limited and a single intervention or drug alone is unlikely to be completely effective. With the ability to form long-term therapeutic relationships with patients and access to allied health resources, GPs can have a major role in the longitudinal management of fibromyalgia. Practice points on fibromyalgia are listed in the Box.
{kind=link}
Ultimately, fibromyalgia is a disorder where each small move towards understanding the diagnosis, coping with pain and improving function represents one step on the long journey towards resilience and autonomy. The therapeutic goal is to guide patients along the way until they are empowered to independently traverse the sometimes treacherous terrain of fibromyalgia with the tools and experience they have acquired. MT
COMPETING INTERESTS: Dr Khoo and Dr Chin: None. Dr Whittle is an Executive Committee Member of Australia and New Zealand Musculoskeletal Clinical Trials Network (ANZMUSC) and his work as a developer of An Australian Living Guideline for the Pharmacological Management of Inflammatory Arthritis is supported by an ANZMUSC Practitioner Fellowship.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.