Male genital dermatology. Part 1: Inflammatory dermatoses

Men's health
Male genital disease mostly comprises noninfectious skin disease, with the most common inflammatory condition being dermatitis. Uncircumcised males have a much higher risk of genital disease. The negative psychological, social and sexual impact of genital disease on a male patient is often considerable. The time taken to make a diagnosis and implement a treatment plan demonstrates not only your care for your patient but is an important part of the therapeutic process.
- Most diseases of male genitalia are common inflammatory skin diseases.
- Many male patients have an underlying fear of a sexually transmissible infection (STI) or genital cancer.
- The clinician’s knowledge of the range of common variants of male genital anatomy and the range of inflammatory dermatoses and noninflammatory lesions of male genitalia is key to effective management.
- Uncircumcised males have a much higher risk of genital disease.
- Pathological phimosis is most commonly caused by lichen sclerosus.
- Irritant dermatitis is the most common genital skin disease.
- Topical corticosteroids are the mainstay of treatment for most genital dermatoses.
- Nonsexually acquired infections include pyogenic bacterial infections (e.g. impetigo), candidiasis, erythrasma, tinea and scabies.
- Important STIs of genital skin include genital warts, herpes genitalis, syphilis (increasing incidence throughout the world) and scabies. Infestation with pubic lice is becoming less common.
Many male patients with genital disease often have an underlying fear of either a sexually transmissible infection (STI) or genital cancer. Male genital disease mostly comprises noninfectious skin disease. The presence of a foreskin (prepuce) is associated with a much higher risk of genital disease. An assumption that genital disease is an STI often leads to poor management. If investigations exclude an STI, often no diagnosis is made and the patient is left confused and untreated, often still fearful of an STI or genital cancer. Treating doctors need to know the range of common variants of male genital anatomy and the range of inflammatory diseases and noninflammatory lesions of male genitalia.
The first part of this review of male genital dermatology covers inflammatory male genital dermatoses. The second part of this review in Medicine Today’s May issue will cover noninflammatory male genital diseases, including premalignant and malignant diseases.
Diagnosis
Genital dermatoses (infective, inflammatory and neoplastic) often have a nonspecific appearance especially in an uncircumcised male patient (with the foreskin present). Diagnosis of genital skin disease is based on history, clinical examination, confirmatory investigations and interpretation. Diagnosis is also based on known prevalence of male genital disease in the particular community and probability.
It is often difficult to clinically differentiate a single or multiple red papules or plaques on the glans penis, especially in an uncircumcised patient. Single or multiple red papules or plaques of the male genitalia (glans penis, foreskin, penile shaft or scrotum) may be due to psoriasis, dermatitis, lichen sclerosus, lichen planus, plasma cell (Zoon’s) balanitis, penile intraepithelial neoplasia (in situ squamous cell carcinoma [SCC]) or even early invasive SCC.
Clinical history and examination
It is important for clinicians to take a history before examining any patient who presents with concern of a genital disease and for the patient to be allowed to tell his story. Taking time to obtain a history demonstrates you are listening and that you care. A helpful approach is to begin with open questioning and then ask more focused questions. Enquiring about any possible fear of either an STI or genital cancer are important.
Patients have often used many topical treatments (both prescribed and over-the-counter) in an empirical fashion without a specific diagnosis ever being made. Current and recently used topical treatments should be noted.
The impact of genital disease is often greater than for disease at other anatomical sites. Respect for your patient’s modesty when examining the anogenital region is crucial. Carefully examine under the foreskin (prepuce), inspect the perianal region and other relevant sites (oral mucosa, scalp, flexures, elbows, knees and nails). Careful examination is key as ‘more mistakes are made by not looking than by not knowing’.
Diagnostic tests
Investigations are limited and based on testing of a clinical provisional diagnosis. Investigations to consider include:
• skin swab for microscopy and culture if candidiasis or a bacterial infection is suspected
• skin swab for polymerase chain reaction (PCR) testing for herpes simplex virus if vesicles or erosions are present
• urethral swab for PCR testing for Neisseria gonorrhoeae and Chlamydia trachomatis if there is a urethral discharge
• skin scrapings for fungal microscopy and culture, which are important if tinea of the groin (tinea cruris) is suspected
• skin scraping from any suspected scabies burrow for microscopy, which is recommended to confirm a diagnosis of scabies
• skin patch testing, which is only recommended if allergic contact dermatitis is suspected
• skin-prick testing, which is only of value if immediate contact sensitivity, such as latex allergy, is suspected.
Genital skin biopsy
Skin biopsy is not a substitute for lack of a clinical diagnosis. Histological examination of genital skin biopsy has limitations, particularly differentiating inflammatory skin diseases. However, it is essential to take a genital skin biopsy if genital malignancy cannot confidently be clinically excluded. Most male patients are apprehensive about genital biopsy but usually consent to this procedure once reassured the pain of administering a local anaesthetic is short lived.
The most useful genital skin biopsy techniques are punch biopsy and shave biopsy. A 3mm or 4mm punch biopsy provides adequate tissue for most inflammatory or neoplastic genital disease. A shave biopsy is preferred for pigmentary disorders or a small plaque. A clinician should only biopsy genital skin (in either sex) if confident with the procedure and aware of the risks. A clinician who explains the procedure and projects confidence helps to put anxious patients at ease.
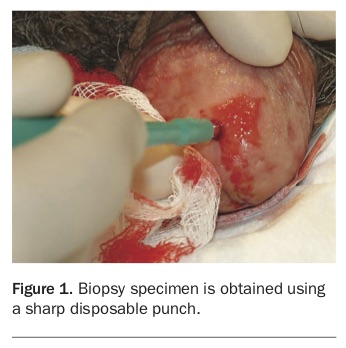
Steps for punch biopsy of the glans penis are:
• Explain the procedure to the patient, including the risk of a permanent scar.
• Obtain consent from the patient.
• Once consent is obtained, proceed quickly as delay only increases anxiety. Talk therapy and distraction therapy (squeezing a soft ball) help alleviate potential anxiety.
• With the patient supine, mark the intended biopsy site.
• Using a small gauge needle (30G), slowly infiltrate a small volume (0.2 to 0.3mL) of 1% (or 2%) lignocaine with 1:200,000 adrenaline that achieves anaesthesia quickly.
• Using a sharp disposable punch, remove the specimen by gentle rotation of the punch with minimal pressure (Figure 1).
• Carefully elevate the biopsy to avoid crushing the specimen with the infiltrating needle (‘shish kebab’ technique).
• Cut off the biopsy specimen at the base.
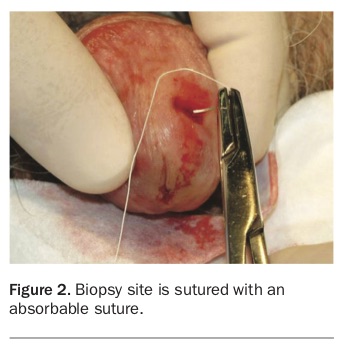
• Suture the biopsy site with an absorbable suture (Figure 2).
{kind=link}
{kind=link}
If there is a discrepancy between the clinical and histological diagnoses, it is important to discuss it with the reporting histopathologist or confer with experienced colleagues.
Common variants of male genitalia
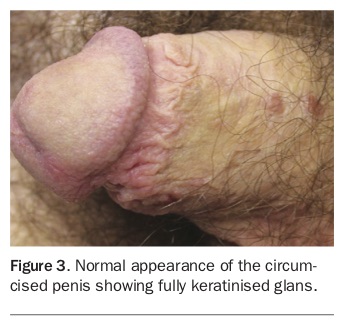
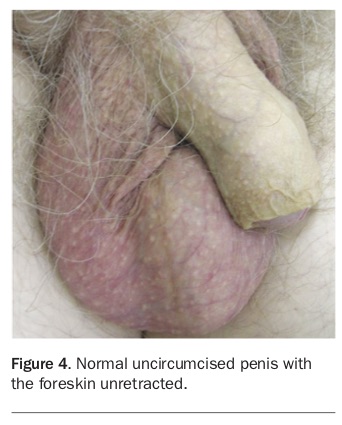
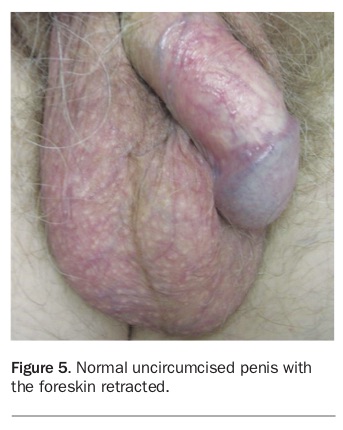
The appearance of genitalia varies greatly between circumcised and uncircumcised males. The glans of a circumcised male is fully keratinised (Figure 3). Under the foreskin of an uncircumcised male the skin of the distal penile shaft often appears thinner, redder and more translucent with visible blood vessels (Figure 4 and Figure 5). Confusion may arise between the normal appearance, dermatitis and corticosteroid atrophy if a topical corticosteroid preparation has been applied to irritated skin. Variation in colour of male genitalia is considerable.
{kind=link}
{kind=link}
{kind=link}
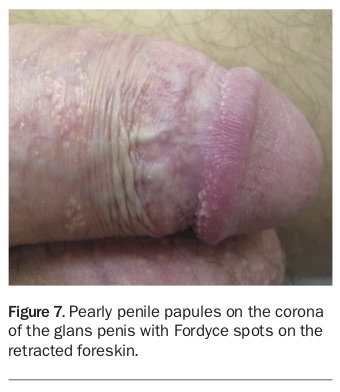
Pearly penile papules, ectopic sebaceous glands (Fordyce spots) and angiokeratoma of Fordyce are common variants that need to be recognised. Pearly penile papules are small 1mm to 2mm diameter asymptomatic pink papules arranged in single, double or triple rows on the corona of the glans penis in up to one-third of males (Figure 6). Pearly penile papules may cause concern at puberty and be misdiagnosed and treated as genital warts. The preferred treatment is reassurance only.
{kind=link}
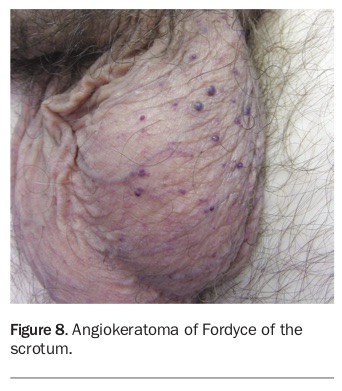
Fordyce spots are ectopic sebaceous glands (not associated with hair follicles) and appear as yellow-white micropapules on the internal surface of the foreskin, occasionally on the glans and penile shaft (Figure 7). Genital Fordyce spots may also be confused with genital warts, even in nonsexually active males. Angiokeratoma of Fordyce are benign, small asymptomatic red to purple papules of the scrotum, varying in number from a few to many (Figure 8). They usually spare the penile shaft and occasionally bleed. Bleeding can be treated with light electrocautery (or vascular laser). Angiokeratomas of Fordyce have no systemic associations. As for Fordyce spots, the preferred treatment of angiokeratoma of Fordyce is reassurance only.
{kind=link}
{kind=link}
Inflammatory male genital diseases
General management
Management of inflammatory male genital disease includes explaining the diagnosis and alleviating any patient fear of a possible STI or malignancy. General measures include avoiding use of soap, regular use of a moisturiser and use of lubricant for sexual activity.
Topical corticosteroids (TCS) are the mainstay of treatment for most genital dermatoses. Mild-to-moderate TCS are extremely effective and well tolerated in the anogenital region. Side effects from use of TCS are rare. Clear instructions should be provided to the patient. Treatment with a TCS should be continued while symptoms are present and ceased once symptoms resolve and the skin disease has cleared. TCS should be used only on visible skin disease. Fear of overuse of TCS on genitalia by doctors, pharmacists and patients makes overuse unlikely (and is rare in the experience of the author).
Topical calcineurin inhibitors (pimecrolimus and tacrolimus; off-label use) are steroid-sparing agents and alternatives to TCS. Topical calcineurin inhibitors are useful for ‘steroid-phobic’ patients but are not more effective than TCS. Topical vitamin D analogues (e.g. calcipotriol) and tar preparations are other alternatives. Low-strength topical tar preparations are useful for persistent perianal psoriasis and chronic dermatitis (lichen simplex chronicus) but may cause irritation on the scrotum or groins.
Light treatment (phototherapy) is contraindicated for all male genital dermatoses due to the theoretical risk of inducing SCC of the scrotum. Systemic agents are rarely used for treatment of dermatoses confined to genitalia but are beneficial for resistant or more widespread dermatoses.
Long-term follow up is essential for chronic dermatoses and when a definitive diagnosis is not possible. Reporting to health authorities and notification of partners is necessary if an STI is confirmed.
Phimosis
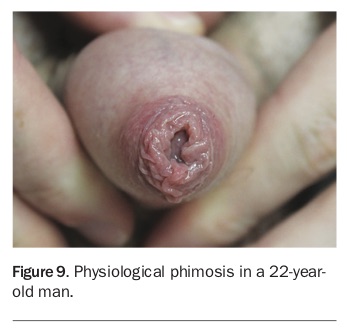
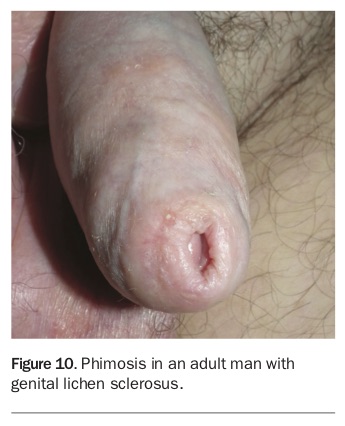
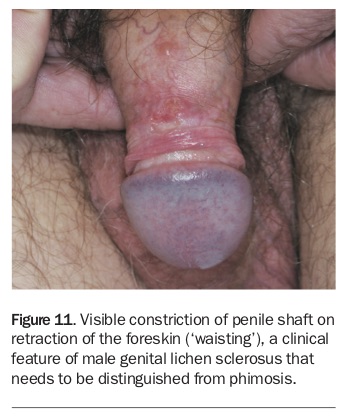
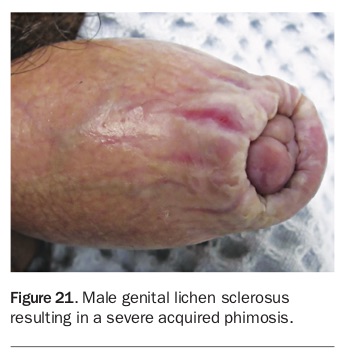
The presence of a foreskin (prepuce) is associated with a higher risk of genital disease. Phimosis is the inability to easily and painlessly withdraw the foreskin over the glans penis. It is important to differentiate physiological phimosis from pathological phimosis. Physiological phimosis is normal at birth (only 4% of male infants have a retractable foreskin at birth) but usually resolves by puberty (99% of males at 17 years of age can painlessly retract their foreskin; Figure 9). Pathological phimosis is best defined as phimosis extending beyond puberty or acquired after puberty that is of concern to the patient. The most common cause of acquired (pathological) phimosis in both boys and men is lichen sclerosus (Figure 10). Phimosis needs to be distinguished from ‘waisting’, a visible constriction of the penile shaft on retraction of the foreskin that is a clinical feature of male genital lichen sclerosus (Figure 11).
{kind=link}
{kind=link}
{kind=link}
Paraphimosis occurs when the foreskin is fixed in the retracted position, resulting in swelling and oedema of the foreskin. Thickening and whitening of the foreskin may be seen and scarring across the coronal sulcus may be visible.
Balanitis and balanoposthitis
Balanitis is a clinical sign of inflammation or redness of the glans penis alone whereas balanoposthitis is inflammation or redness of both the glans and foreskin, without reference to aetiology. Balanitis and balanoposthitis are clinical signs and not diagnoses. Causes include infection (e.g. candidiasis), autoimmunity (e.g. lichen sclerosus), environmental factors (e.g. irritant dermatitis), ingested drugs (e.g. fixed drug eruption), diseases of unknown cause (e.g. plasma cell or Zoon’s balanitis), penile intraepithelial neoplasia (in situ SCC) and invasive neoplastic disease.
Dermatitis (eczema)
Variants of dermatitis (eczema) are the most common inflammatory diseases worldwide so it is not surprising that dermatitis is also the most common male genital skin disease. Variants of male genital dermatitis include irritant dermatitis, allergic contact dermatitis, atopic dermatitis, seborrhoeic dermatitis, chronic lichenified dermatitis (lichen simplex chronicus) and papulonodular dermatitis (nodular prurigo).
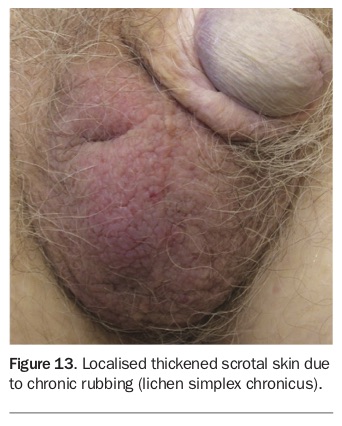
The most common form of dermatitis of uncircumcised males is irritant (contact) dermatitis (Figure 12). Irritant dermatitis is more common than allergic contact dermatitis. Common irritants include soap, sweat, friction and topical medications. Genital atopic dermatitis occurs in the setting of generalised atopic dermatitis so is rarely a diagnostic problem. Chronic rubbing or scratching due to chronic itch leads to chronic localised dermatitis (lichen simplex chronicus). On male genitalia, lichen simplex chronicus presents as a pruritic hyperkeratotic plaque or lichenification of the anterior surface of the scrotum (Figure 13). Nodular prurigo (a papule or nodule on chronic dermatitis) may occur on the shaft of the penis. A single nodule makes skin biopsy essential to exclude SCC. Multiple pruritic nodules on the penile shaft or scrotum are almost pathognomonic for scabies. Genital seborrhoeic dermatitis is an uncommon disease (author’s observation) whereas widespread seborrhoeic dermatitis should alert the clinician to possible underlying HIV infection or other causes of immunosuppression.
{kind=link}
{kind=link}
Management
Mild-to-moderately potent TCS are the mainstay of treatment for genital dermatitis. A mild-to-moderately potent TCS should be applied while the skin is itchy or lichenified and ceased once the itch resolves. More potent TCS may be necessary for chronic eczema (lichen simplex chronicus) for a limited period. Topical calcineurin inhibitors (pimecrolimus and tacrolimus; off-label use) are alternatives to TCS that are useful for patients fearful of the use of TCS but they are not clinically superior in efficacy to TCS. Topical calcineurin inhibitors may cause irritation on genital skin that may limit their use. Systemic agents may be necessary for more widespread dermatitis. Nonsedating antihistamines are useful to control daytime itch, and low-dose doxepin (10 to 20mg) taken with the evening meal is useful to help control nocturnal pruritus, particularly if it is disturbing sleep.
Psoriasis
Psoriasis is a common inflammatory dermatosis affecting up to 3% of the world’s population. It is now recognised as a systemic inflammatory disease with predominantly cutaneous features. Psoriasis is characterised by symmetrically arranged, red, scaly cutaneous plaques, located on extensor aspects of the elbows, knees, scalp and natal (intergluteal) cleft.
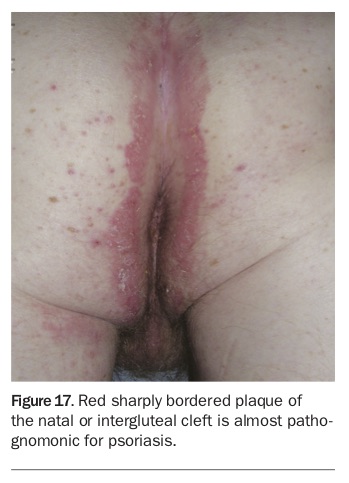
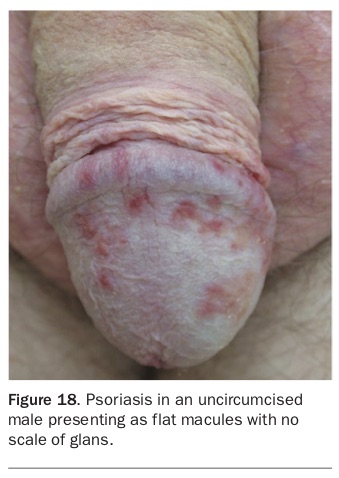
Two-thirds of patients with psoriasis experience genital involvement at some stage of their disease. Symptoms include itch, irritation, dyspareunia and embarrassment, resulting in a marked negative impact on psychological and sexual quality of life. Genital psoriasis may present as flat papules on the glans penis (Figure 14), plaques on the penis or scrotum (Figure 15) or diffuse redness of the glans and inner aspect foreskin as balanoposthitis (Figure 16). Psoriasis of the natal cleft is common. A red sharply bordered plaque of the natal (or intergluteal) cleft is almost pathognomonic for psoriasis (Figure 17). Scale may be absent in the natal (or intergluteal) cleft. The clinical appearance of psoriasis on the glans penis is altered if the patient is uncircumcised and if TCS have been used. In uncircumcised males, scale is often absent on the glans and psoriasis may present as flat macules (Figure 18). Evidence of psoriasis at other sites helps in making a diagnosis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Management
TCS are effective and well tolerated for genital psoriasis. Start with a more potent TCS cream (for four to six weeks) and then reduce to a milder TCS to be used only as needed. This method usually results in more rapid clearance of anogenital psoriasis. Treatment with TCS should be ceased once psoriasis is no longer visible. Systemic agents (methotrexate, ciclosporin, acitretin, mycophenolate or targeted therapies) are rarely needed for psoriasis confined to the anogenital region. Phototherapy to genitalia should be avoided because of the increased risk of SCC of the scrotum. Failure to achieve improvement within four to six weeks necessitates a review of the original diagnosis and assessment of compliance with treatment. If there is no response to treatment with TCS, skin biopsy is necessary to exclude in situ SCC (penile intraepithelial neoplasia).
Male genital lichen sclerosus
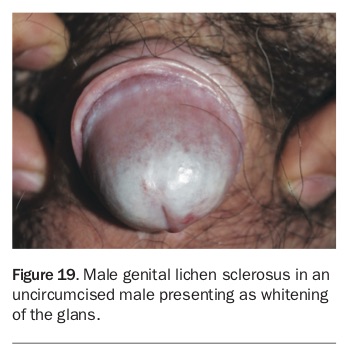
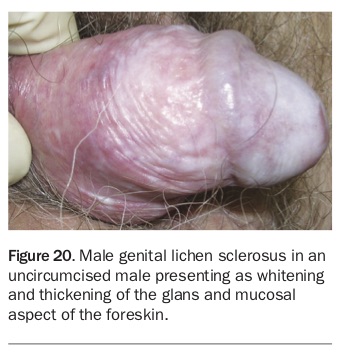
Lichen sclerosus is a chronic inflammatory skin disease mainly involving genital skin. Male genital lichen sclerosus occurs in uncircumcised young boys and men, resulting in whitening or purpura with thickening of the glans (Figure 19) and foreskin (Figure 20). Sometimes there is paradoxical thinning (atrophy) with telangiectases and purpura. The cause is unknown but male genital lichen sclerosus is probably an autoimmune disease. Genital lichen sclerosus may be asymptomatic or may result in phimosis, causing significant sexual dysfunction with painful erections and dyspareunia (Figure 21). Male genital lichen sclerosus (like female vulval lichen sclerosus) is probably a premalignant disease for SCC of the glans penis but the exact risk of malignant transformation is not accurately known.
{kind=link}
{kind=link}
{kind=link}
Management
Treatment of male genital lichen sclerosus is aimed at maximising normal function, improving cosmetic appearance and detecting development of early SCC of the glans. Treatment with a potent TCS for six to 12 weeks with a gradual tapering is safe and usually effective. Once improvement is achieved a less potent TCS can be used. If treatment with a potent TCS fails to improve male genital lichen sclerosus then circumcision should be discussed. Urologists refer to lichen sclerosus with phimosis as ‘balanitis xerotica obliterans’ and usually recommend circumcision as first-line treatment. Circumcision is not always curative for male genital lichen sclerosus. Treatment after circumcision with a potent TCS is necessary if there is persisting lichen sclerosus of the glans.
Topical tacrolimus (a calcineurin inhibitor) is an alternative to treatment with a TCS but may cause irritation. Topical tacrolimus is not clinically more efficacious than potent TCS. Concerns regarding the safety of calcineurin inhibitors on premalignant genital skin disease (in both sexes) have been raised.
Occasionally surgical correction of urethral meatal stenosis or penile urethral involvement in patients with genital lichen sclerosus is necessary. Follow up of patients is essential to assess the response of male genital lichen slerosus to treatment and to detect possible early SCC.
Plasma cell (Zoon’s) balanitis
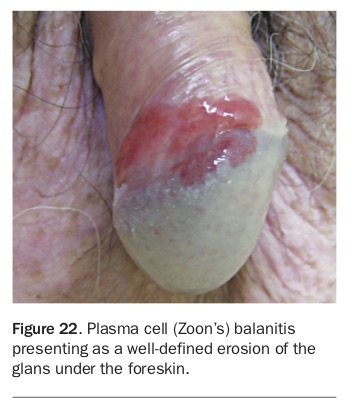
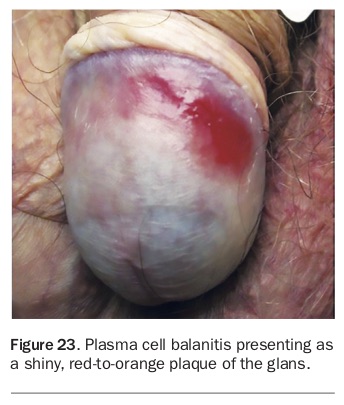
Plasma cell (Zoon’s) balanitis occurs in uncircumcised, middle-aged to older men as a well-defined eroded plaque of the glans under the foreskin (Figure 22) or a shiny, red-to-orange plaque of the glans penis (Figure 23). Both the glans and under surface of the foreskin may be involved as ‘kissing’ lesions. Tan brown spots (‘cayenne pepper’ spots) may be visible.
{kind=link}
{kind=link}
Plasma cell balanitis is thought to arise from irritation or mild trauma of the moist environment under the foreskin. Plasma cell balanitis is often asymptomatic. Possible symptoms include burning, itch, discharge or bleeding. Plasma cell balanitis tends to run a chronic, benign course. Taking a genital skin biopsy is important to help confirm the clinical diagnosis, although the histopathology is not always specific. Histopathologic examination helps to exclude in situ SCC (penile intraepithelial neoplasia) that may appear similar clinically.
Management
Although the most effective treatment is circumcision, symptomatic treatment may be appropriate for elderly or infirmed patients. Elderly men with plasma cell balanitis may be unconcerned about their disease, particularly if asymptomatic, and may be reluctant to be circumcised. Illness and infirmity are mitigating factors against circumcision. Clinical improvement is usually achieved with a potent TCS cream combined with a topical antibiotic. Topical tacrolimus is an alternative topical treatment. The combination of a potent TCS with a topical antibacterial cream often induces a temporary remission that may be acceptable management to the patient.
Genital lichen planus
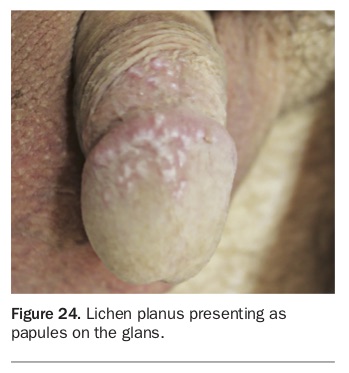
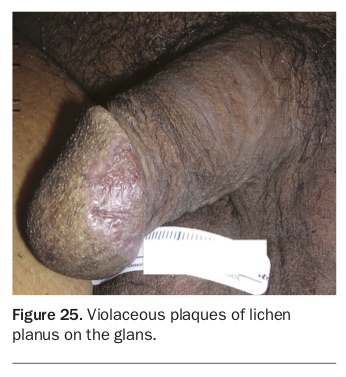
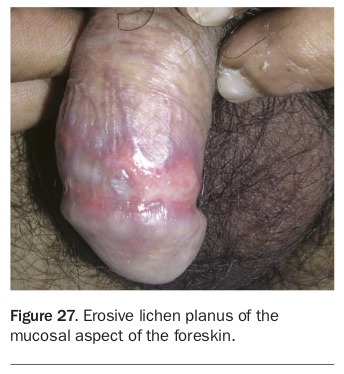
Lichen planus is a chronic cutaneous inflammatory disease of uncertain aetiology involving the skin, hair, nails and mucosal surfaces. Genital lichen planus has features similar to male genital lichen sclerosus, but with some differences. Lichen planus of the glans, foreskin or penile shaft may present as papules (Figure 24), plaques (Figure 25), annular lesions (Figure 26), a lace-like pattern or erosive disease (Figure 27). The erosive form occurs in uncircumcised males, involving the glans and foreskin of the preputial recess (or subprepuce). Whereas lichen sclerosus is predominantly an anogenital disease, genital lichen planus may be associated with lichen planus at other sites. Genital lichen planus may be asymptomatic but itch, irritation, discomfort or pain are all symptoms. Peno-gingival lichen planus has been reported, similar to the vulvo-vaginal-gingival syndrome in female patients. Confirmation of the clinical diagnosis with skin biopsy is important.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Management
Preferred treatment of male genital lichen planus is with a potent TCS. Alternative treatments tried include use of a topical calcineurin inhibitor (pimecrolimus, tacrolimus). A persistent plaque of hypertrophic lichen planus may require treatment with an intralesional corticosteroid. More recalcitrant lichen planus may require treatment with systemic immunosuppressive agents including oral corticosteroids, methotrexate or acitretin (a retinoid). Treatment of severe erosive lichen planus may require a systemic agent combined with circumcision. Postinflammatory hyperpigmentation is a common complication of genital lichen planus.
Nonsexually acquired infections
Genital infections are both sexually and nonsexually acquired. Nonsexually acquired infections include viral infections (e.g. molluscum contagiosum), pyogenic bacterial infections (e.g. impetigo), candidiasis, erythrasma, tinea and scabies. Examination of all groin and flexural eruptions with a Wood’s (UVA) lamp is important. A skin swab (e.g. for suspected impetigo, candidiasis) or skin scraping (e.g. for suspected tinea cruris, scabies) are useful investigations when indicated. Consider skin biopsy for more chronic or resistant flexural eruption to exclude rarer flexural diseases (e.g. Hailey-Hailey disease, Darier’s disease) or unusual malignancies (e.g. extramammary Paget’s disease).
Molluscum contagiosum is usually a nonsexually acquired disease in children but may be sexually acquired in adults, especially if involving the genitalia. Treatment of genital molluscum contagiosum is not always easy. Cryotherapy (liquid nitrogen treatment), topical imiquimod and topical cantharidin are all useful treatments for molluscum contagiosum in adults. Curettage under local anaesthesia (with a sharp, disposable curette) is the best treatment for resistant genital molluscum contagiosum in adults. Curettage provides tissue for histological confirmation of the diagnosis. Atypical molluscum contagiosum or molluscum occurring at different sites (e.g. face) should prompt consideration of possible underlying immunosuppression, particularly HIV infection.
Pyogenic bacterial infections and candidiasis are confirmed by microbiological examination. Pyogenic bacterial infections are best treated with either topical or oral antibiotics, guided by bacterial sensitivities. Candidiasis may be primary or secondary to irritant dermatitis. Treatment with either a topical imidazole, topical terbinafine or an oral azole (e.g. fluconazole) is effective. If more extensive candidiasis is encountered, diabetes should be excluded.
Erythrasma is a symmetrical, slightly scaly, red-brown flexural eruption of the axillae and groin due to Corynebacterium minutissimum. Examination with a Wood’s lamp produces a characteristic coral-pink fluorescence, pathognomonic for erythrasma.
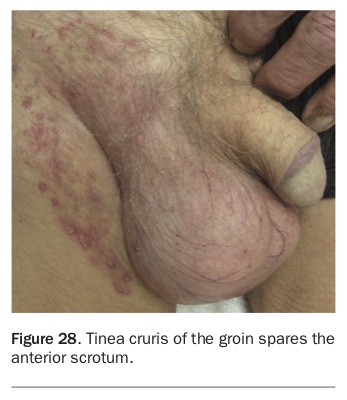
Tinea cruris (a superficial skin fungal infection of the groins) usually spares the anterior scrotum and penis (Figure 28). A skin scraping for microbiological examination confirms the diagnosis. Treatment with a topical imidazole cream or topical terbinafine may be adequate but more extensive disease is best treated with oral griseofulvin (500mg daily for six weeks), oral fluconazole (50 to 100mg daily or 150mg once weekly for two to four weeks) or oral terbinafine (250mg daily for two weeks).
{kind=link}
Scabies is an important human skin infestation seen worldwide. Pruritic papules of the male genitalia are (almost) pathognomonic for scabies infestation (Figure 29). Pruritic papules on the penile shaft and scrotum due to scabies vary from few to many (Figure 30). Clinical diagnosis is not always easy. Drawing over a suspected scabetic burrow with a washable marker pen and wiping off the excess ink with an alcohol swab may help identify a scabetic burrow. A skin scraping from burrows between fingers or volar aspects of the wrists demonstrating the scabetic mite confirms the clinical diagnosis. A scabies mite in a cutaneous burrow may more easily be identified with dermoscopy. Topical treatment with 5% permethrin cream (or 25% benzyl benzoate lotion) is usually effective. The permethrin cream (or benzyl benzoate lotion) is applied to the whole body surface from the neck down and left on for at least eight hours (overnight). The permethrin cream (or benzyl benzoate lotion) are washed off in the morning. This procedure is repeated after seven days. All clothing and bedding need to be carefully washed and all possible contacts treated. Common scabies is usually spread from a family member or close contact. Scabies is more commonly transmitted from a person infected with crusted (Norwegian) scabies. A patient infected with crusted scabies needs more intensive topical treatment combined with systemic treatment with oral ivermectin (0.2mg/kg). Recommendations for treatment of crusted scabies with oral ivermectin are variable, with treatments repeated four to seven times over one to four weeks.
{kind=link}
{kind=link}
Sexually transmissible infections (STIs)
STIs remain a worldwide problem. Important STIs of genital skin include viral infections (warts, herpes simplex) and bacterial infections (syphilis). Sexually transmitted infestations with pubic lice (crab lice or pediculosis) are becoming less common with pubic depilation (e.g. Brazilian waxing). Opportunistic screening for STIs should be undertaken whenever appropriate. STIs commonly occur together, particularly chlamydia, gonorrhoea, hepatitis B, hepatitis C, syphilis or HIV infection, so if one is detected, others should be looked for. STIs often have atypical presentations in immunosuppressed patients.
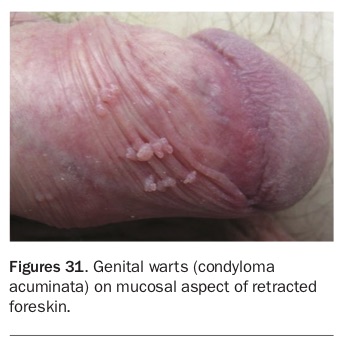
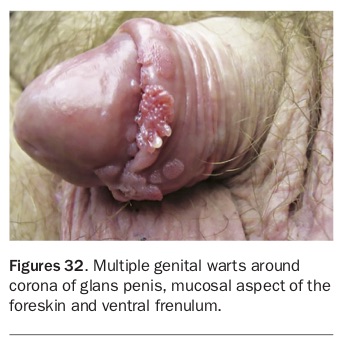
Anogenital warts (condyloma acuminata; Figure 31 and Figure 32) are caused by infection with certain strains of the human papillomavirus (HPV). Condyloma acuminata are a common STI worldwide but challenging to treat. Treatment of anogenital warts usually requires repeated doctor-administered cryotherapy (liquid nitrogen) combined with patient-applied topical preparations (e.g. imiquimod cream, podophyllotoxin lotion). Shave excision or curettage under local anaesthesia is often necessary for more resistant anogenital warts. Persistence and patience are necessary for successful treatment. Clinical anogenital warts and subclinical HPV infections are reduced by immunisation with the HPV vaccine prior to the onset of sexual exposure. Although the use of HPV vaccine has been shown to significantly reduce female genital tract cancers, the impact of HPV vaccination in preventing male genital cancers is as yet unclear. It is important to exclude anal carcinoma in any patient with perianal warts who is co-infected with HIV, particularly men who have sex with men (MSM).
{kind=link}
{kind=link}
Herpes simplex virus (HSV) is the most common cause of genital vesicles (Figure 33), erosions and ulceration. Recurrent outbreaks of genital herpes are common. The first clinical episode of genital herpes is usually a reactivation, rather than primary infection. Genital ulceration predisposes the patient to other STIs. The severity and duration of acute episodes of herpes genitalis is usually reduced with a five- to 10-day course of oral antiviral therapy (aciclovir, valaciclovir or famciclovir). More frequent relapses require long-term suppressive therapy with an antiviral medication.
{kind=link}
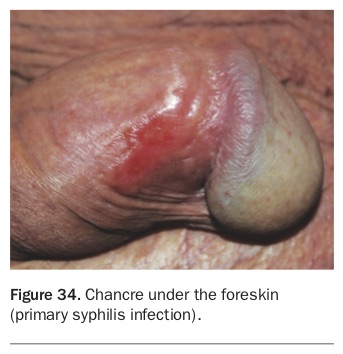
Syphilis is caused by the bacterium Treponema pallidum. Syphilis is increasing worldwide, particularly in MSM who are co-infected with HIV. Syphilis may be congenitally acquired but is mostly an acquired STI. Primary infection with T. pallidum is characterised by a painless eroded or ulcerated plaque known as a chancre (Figure 34). It is important to inspect under the foreskin, oral cavity and perianal region for occult chancres. Taking a skin swab, performing a genital skin biopsy and arranging syphilis serology are important investigations for any painless eroded or ulcerated genital plaque (suspected chancre). Syphilis is the great imitator. Secondary and tertiary syphilis are more difficult to diagnose. Secondary syphilis should be suspected in any patient with maculopapules on the palms (of the hands) or soles of the feet or any patient with a pityriasis rosea-like, scaly truncal eruption. In any patient co-infected with HIV, atypical presentations of syphilis may be more difficult to diagnose. Fortunately, T. pallidum has remained relatively penicillin sensitive. Long-acting penicillin still remains the treatment of choice for syphilis. Partner notification, partner treatment and long-term follow up are essential if syphilis is diagnosed.
{kind=link}
Conclusion
Appropriate management of male genital skin diseases is based on making a correct diagnosis. Differentiating common variants from true genital skin disease is essential. Common variants of male genitalia include differences in skin colour, pearly penile papules, ectopic sebaceous glands (Fordyce spots) and angiokeratoma of Fordyce. The presence of a foreskin (being uncircumcised) is associated with higher rates of genital skin disease. The important male genital inflammatory skin diseases include dermatitis, psoriasis, lichen sclerosus, lichen planus and plasma cell (Zoon’s) balanitis. Male genital skin infections may be either nonsexually or sexually acquired. Nonsexually acquired male genital skin diseases include candidiasis, molluscum contagiosum, pyogenic skin infections, erythrasma, tinea cruris and scabies. Important sexually acquired male genital skin diseases include herpes genitalis, anogenital warts and syphilis. Scabies can also be transmitted sexually. Syphilis infection is on the increase worldwide.
The second part of this article to be published in the May issue of Medicine Today will cover premalignant and malignant disease. MT