Testicular cancer. Key issues in diagnosis, treatment and follow up

Testicular cancer is the most commonly diagnosed malignancy in men aged under 40 years. Eliciting red flags for metastatic disease and discussing fertility are key issues in the early diagnostic process. Monitoring for long-term sequelae of treatment and potential relapse is important in the management of survivors of testicular cancer.
- Testicular cancer is the most commonly diagnosed malignancy in men aged under 40 years.
- Men presenting with a testicular lump and a solid intratesticular lesion on ultrasound need an urgent urology referral as most types of testicular cancer are rapidly progressing.
- Surveillance of lower stage disease is the recommended strategy to minimise morbidity of adjuvant chemotherapy, radiotherapy or surgery but requires clinicians to be vigilant for relapse.
- Chemotherapy, radiotherapy and surgery with retroperitoneal lymph node dissection are treatment options after orchidectomy for higher stage testicular cancer or lower-stage cancers with possible occult metastasis.
- It can take on average two years for fertility to recover after adjuvant treatment. Therefore, a family planning discussion about semen cryobanking before treatment is paramount.
- Testicular cancer survivors should be monitored for relapse, cardiovascular disease, secondary malignancy and hypogonadism.
Over 900 men are diagnosed with testicular cancer in Australia each year.1 Patients typically present with a painless firm lump, but other nonspecific symptoms may indicate the presence of metastatic disease. Although in many circumstances radical orchidectomy alone is curative, a multidisciplinary team of urological surgeons and medical and radiation oncologists is required for the management of advanced testicular cancer. Implications of treatment on fertility requires careful consideration and planning pre-treatment. High survivorship rates necessitate monitoring for long-term risks associated with adjuvant treatment. This article summarises the presentation, initial investigations, treatment options and long-term implications of treatment for testicular cancer, with a focus on germ cell tumours.
Pathology
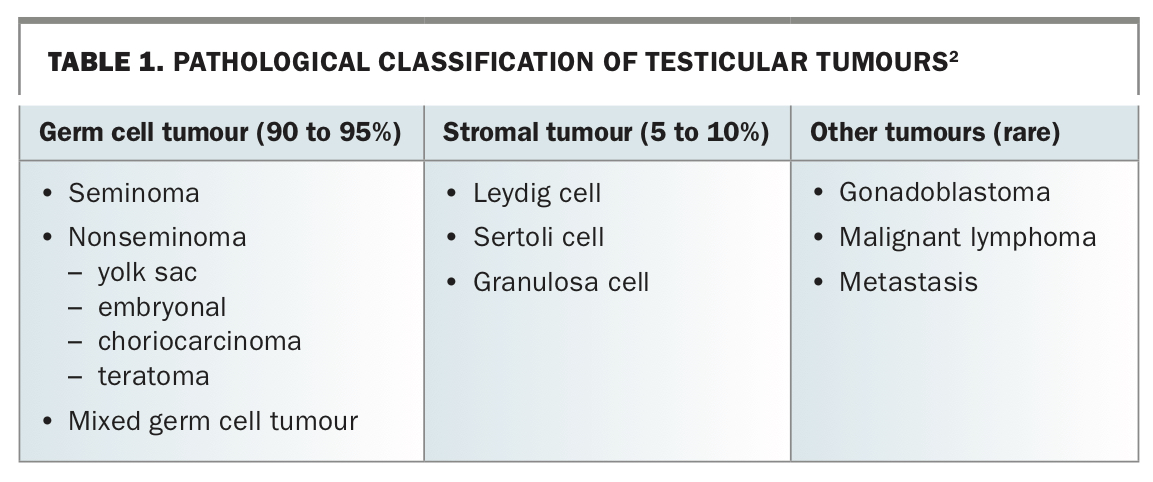
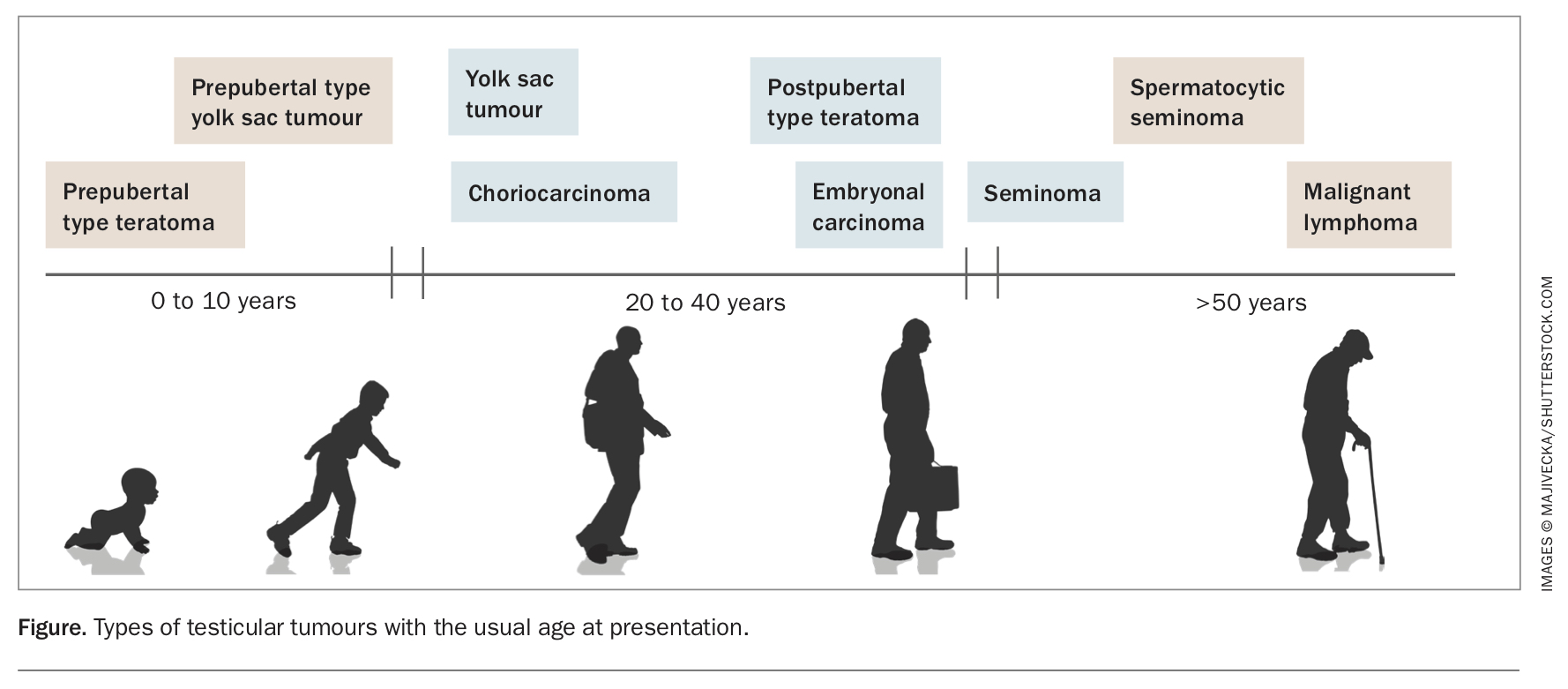
Primary testicular cancer can be divided into germ cell tumours (90 to 95%) and stromal tumours (5 to 10%) (Table 1).2 Testicular cancer can present in three distinct age groups: prepubertal boys up to 10 years of age, men aged between 20 and 40 years, and men older than 50 years; the age of presentation will relate to the pathology of the testicular cancer (Figure). In the prepubertal age group, teratomas are the most common tumour, and almost always behave in a benign fashion, followed by pure yolk sac tumours, which are malignant. In men aged over 50 years, malignant lymphoma is the most common testis tumour. In addition, spermatocytic seminomas are indolent tumours that predominantly affect this age group.
{kind=link}
{kind=link}
In men aged between 20 and 40 years, tumours commonly arise from a precursor lesion, termed germ cell neoplasia in situ (GCNIS), and are histologically divided into seminomas and nonseminomas. Seminomas account for around 65% of germ cell tumours and commonly present in men aged between 30 and 40 years.
Nonseminomas comprise a broad group of tumours including choriocarcinoma, embryonal carcinoma, yolk sac tumours and teratoma. Most nonseminomas have a mix of these pathologies. Unlike in children, teratoma in adults has malignant potential, and can dedifferentiate into somatic malignancy and grow to invade and encase adjacent structures, particularly in the retroperitoneum or mediastinum.
Gonadal stromal tumours, such as Leydig cell and Sertoli tumours account for less than 10% of primary testicular tumours. They can secrete androgens and/or oestrogens, leading to virilisation and gynaecomastia. Around 10% are malignant.
Diagnosis
Presentation
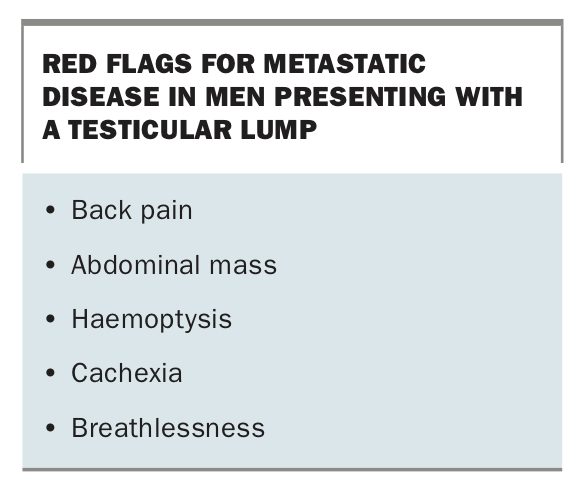
Most men present with a painless, palpable testicular lump. Only one in 10 men will present with testes pain, likely caused by intra-tumour haemorrhage. Most men present with clinically localised disease; however, the red flags of back pain, abdominal mass, haemoptysis, cachexia and breathlessness should raise the alarm for metastatic disease (Box). Retroperitoneal lymph nodes are the most common site of metastatic spread, followed by distant metastasis to lung, liver and brain. An overview on the management of a patient with testicular cancer, from diagnosis through to monitoring after treatment, is presented in the Flowchart.
{kind=link}
Key risk factors should be elicited. Cryptorchidism as a child, particularly if not corrected before the age of 12 years, HIV infection, infertility, family history and Klinefelter’s syndrome all increase the risk of testicular cancer.3,4 A history of testicular trauma or atrophy does not increase risk of testicular cancer.
On examination, a nontender lump arising from the testis is typically found. Testicular cancer, most commonly malignant lymphoma, can present as bilateral disease and thus examination of the contralateral side is paramount. Occasionally, a concurrent hydrocele may obscure the tumour clinically; in such cases, further evaluation with a scrotal ultrasound is recommended. Patients should also be examined for signs of metastatic disease such as an abdominal mass, inguinal lymphadenopathy (particularly in the setting of previous scrotal or inguinal surgery) and abnormal chest auscultation. Gynaecomastia is occasionally seen in men with germ cell tumours but is a common sign in Leydig and Sertoli cell tumours.
Initial investigations
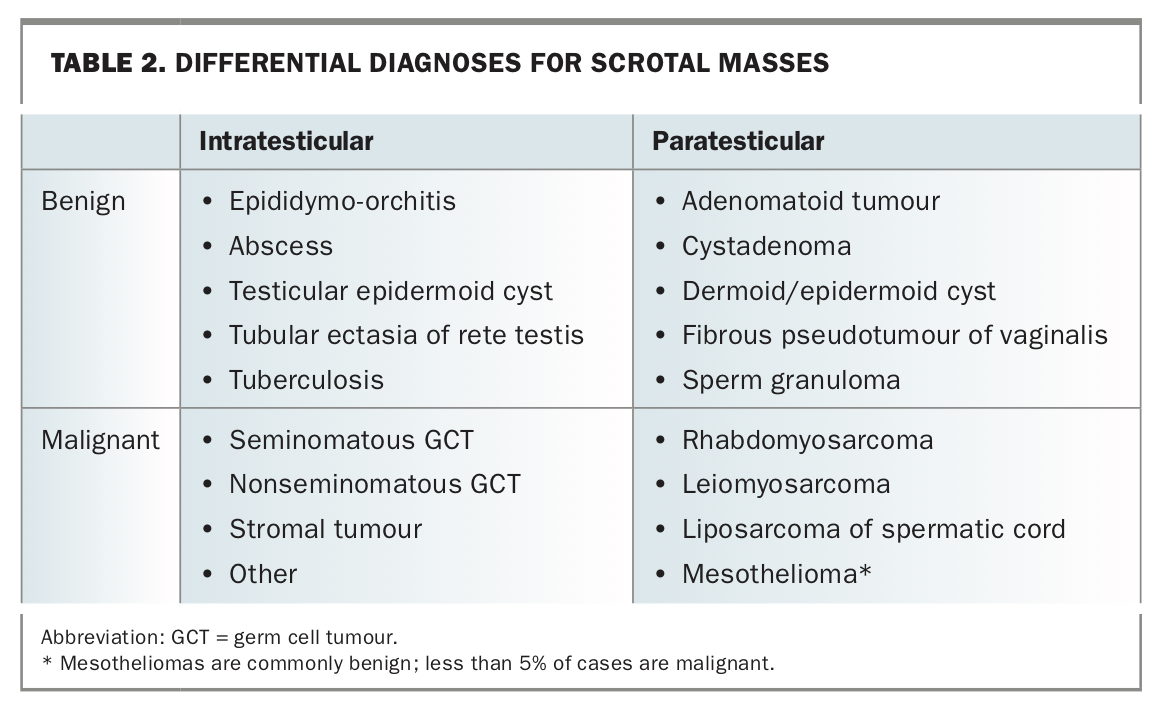
The key diagnostic imaging test is trans-scrotal ultrasonography. Most testicular tumours appear as hypoechoic and heterogeneous solid masses within the testes and are vascular on Doppler images. Any intratesticular lesion with solid elements should be regarded as malignant until proven otherwise. Paratesticular lesions are uncommon and typically benign; however, rare paratesticular malignancies such as rhabdomyosarcoma can be discovered (Table 2). Testicular microlithiases are often found on ultrasound, typically associated with a solid testicular mass. An isolated finding of testicular microlithiasis was thought to be a risk factor for testicular cancer; however, the most recent guidelines do not recommend further evaluation for an incidental finding of testicular microlithiasis in the absence of a solid mass or risk factors for testis cancer.5
{kind=link}
Levels of serum tumours markers, namely alpha-fetoprotein (AFP), beta-human chorionic gonadotrophin (beta-HCG) and lactate dehydrogenase (LDH) are assessed as part of the diagnosis. AFP and beta-HCG levels help to differentiate between different types of testicular cancer, whereas LDH level correlates with the volume of cancer present. Baseline blood tests, including a full blood count, urea, electrolyte and creatinine levels and liver function tests, should also be obtained to exclude hepatic causes of elevated AFP.
Urology consultation
At this stage in the diagnostic pathway, urgent referral to a urologist is mandatory for excision of the testicular mass. This serves both a diagnostic and therapeutic purpose, as treatment of testicular cancer is primarily based on the staging and pathology of the tumour. Some aggressive nonseminomatous tumours (choriocarcinoma) can metastasise very quickly, therefore, urgent referral is necessary after ultrasound scan confirming a testicular lesion. Management of testicular cancer is complex, and patients should be referred to high-volume cancer centres for the best outcomes.6
In healthy men with a normal contralateral testis, radical inguinal orchidectomy is the preferred approach, whereby the testis and its covering tunica vaginalis are excised with the spermatic cord. This is commonly performed as a day surgery through a small inguinal incision, as trans-scrotal orchidectomy can disrupt the spread of testicular cancer, risking spread to other groups of lymph nodes (termed scrotal violation). Testicular prosthesis can be offered to patients at the time of radical orchidectomy or can be deferred. In patients with high volume metastasis or metastatic to viscera, orchidectomy is often deferred until after chemotherapy.
Special situations in which a testis-sparing approach, excising only the cancer from the normal testicular tissue, can be considered when the tumour is in a solitary testis, synchronous bilateral testes tumours are present or contralateral testes are poorly functioning. Tumours that are likely benign, indicated when serum tumour markers are normal and maximum diameter of the mass is smaller than 2 cm, may also be considered for a testis-sparing approach.5 If preservation or fertility is not desired or hypogonadism is present, a testis-sparing approach is irrelevant and radical orchidectomy is performed.
Staging
Computed tomography of the abdomen and pelvis is obtained to stage the retroperitoneal nodes that serve as the main lymphatic drainage pathway of the testes. Chest imaging with either a radiography or CT scan is also needed.
Staging of testicular cancer is based on the American Joint Committee on Cancer (AJCC) TNM Staging System that describes the amount and spread of cancer, where T is the size of the primary tumour, N is the number of cancerous lymph nodes and M refers to whether the cancer has metastasised.7 Interestingly, testicular cancer is the only malignancy to have an S stage for its TNM criteria – this is the nadir value of the post-orchidectomy serum tumour markers and differentiates lower-stage from more advanced malignancy. Patients are also classified according to prognostic risk categories (good, intermediate and poor) based on their cancer type, stage and tumour marker levels, which will help with their management and surveillance protocols.
Treatment
Treatment of testicular cancer is based on the staging and pathology of the tumour. Differentiating between seminoma and nonseminoma is required for treatment decisions. When tumours demonstrate mixed seminomatous and nonseminomatous elements, the treatment protocol for nonseminomas is used. In general, stage I disease is confined to the testis, stage II is spread to the lymph nodes and stage III involves distant metastases. Patients’ staging should be discussed at a multidisciplinary uro-oncology meeting to tailor the many available treatment options to the individual patient.
Surveillance
Historically, patients with testicular cancer have undergone adjuvant therapy to reduce the risk of recurrence. However, as understanding of the risk factors for recurrence has improved, surveillance for low-risk patients is recommended in place of adjuvant therapy to reduce the morbidity from systemic therapies. Generally, patients with either seminoma stage I or nonseminoma stage I testicular cancer should be considered for surveillance. The relapse rate is between 15 and 20%, with most relapses occurring within two years of orchidectomy and only very rarely occurring after five years. Surveillance requires a high degree of patient adherence, with follow-up appointments and scans initially every four to six months. In patients likely to be nonadherent, adjuvant therapy is more likely to be considered.
Chemotherapy
With the exception of teratomas, germ cell tumours are chemosensitive. Platinum-based therapies (e.g. cisplatin) are the most effective agents against germ cell tumours; however, multidrug regimens are more effective than platinumbased therapies alone. The most commonly used regimen for primary treatment consists of bleomycin (an antitumour antibiotic that binds to and breaks DNA), etoposide (DNA alkylating agent) and cisplatin (DNA cross-linking agent). Number of cycles used varies depending on stage and tumour marker response. Acute toxicities are common and include fatigue, diarrhoea, electrolyte imbalances, neutropenia and thrombocytopenia, peripheral neuropathy, ototoxicity and nephrotoxicity. Rarely, bleomycin-induced lung injury is seen, where a fibrotic response manifests as restrictive lung disease. Salvage chemotherapy is used for men who progress during primary therapy, or relapse afterwards, and can consist of high-dose chemotherapy requiring autologous bone marrow transplant in some instances.
External beam radiotherapy
Once a commonly prescribed treatment for seminomas, the use of external beam radiotherapy as adjuvant treatment for seminomas has declined rapidly in Australia in the past three decades.8 As trials have shown surveillance to be an efficacious strategy for stage I disease, patients can now avoid the unnecessary acute toxicities (gastrointestinal, fatigue, bone marrow suppression), late toxicities (peptic ulceration, gastritis), and long-term risks of cardiovascular morbidities and secondary malignancies. In addition, single-dose carboplatin has emerged as the better alternative to radiotherapy for patients electing adjuvant treatment, with better toxicity profile, shorter treatment course and equivalent oncologic outcomes.9 Similarly, in stage IIA/IIB seminoma, chemotherapy is the preferred treatment due to fewer long-term side effects and lower incidence of secondary malignancy.10 Nonseminomatous germ cell tumours are resistant to radiotherapy and it is not used for this pathology.
Primary retroperitoneal lymph node dissection
Retroperitoneal lymph node dissection (RPLND) surgically removes all the lymph nodes that drain the affected testes. It provides the most accurate pathologic staging, has a low risk of short- and long-term complications in experienced hands and minimises the risk of relapse from chemoresistant germ cell tumours and teratomas. With recent advancements in minimally invasive surgery, robotic- RPLND has emerged as an alternative option to traditional open surgery, with reduction in surgical morbidities, pain and recovery time, while maintaining oncologic proficiency.11 RPLND surgery (both open or robotic) is a very complex operation that should only be performed at high-volume centres with experienced surgeons.
Residual lesions
Residual lesions that remain after chemotherapy or radiotherapy are common, but may not necessarily contain tumour. Seminomas are very chemosensitive; around 95% of residual seminomatous masses are inflammatory or necrotic, and generally do not require surgical resection. For nonseminomatous tumours, post-chemotherapy residual tumours can contain either viable germ cell tumour (around 10%), teratoma (around 40%) or fibrosis/necrosis (around 50%). Teratoma is especially important to surgically remove, as it:
- is unresponsive to chemotherapy and radiation
- can grow rapidly to encase or invade adjacent structures
- can undergo malignant transformation into a somatic malignancy
- can lead to a late recurrence of germ cell tumour.12
Patients with large residual lesions who have normal serum tumour markers require surgical resection. Resection of post-chemotherapy residual tumours can be a technically challenging procedure, owing to the post-chemotherapy effects of inflammation and fibrosis and close proximity to vascular structures.11 Tumour resection should be performed by surgeons who are experienced in RPLND. Residual masses with elevated tumour markers indicate persisting viable tumour, and salvage chemotherapy is the preferred treatment.
Fertility
Testicular cancer is associated with subfertility. At the time of diagnosis for testicular cancer, up to half of patients have abnormal semen parameters, and 10 to 35% are infertile. Hypothesised mechanisms include:
- disruption of spermatogenesis by tumour-secreted hormones, which are thought to raise intratesticular oestrogen levels
- tumour-induced damage of the testis-blood barrier causing anti-sperm antibodies to infiltrate the seminiferous tubules
- disruption of the hypothalamic–pituitary–gonadal axis by over- and undersecretion of hormones from the testis.13
Discussing fertility and family planning with patients before starting treatment is imperative. Most patients who require only radical orchidectomy for treatment can achieve conception at a similar rate to the general population.14
However, several adjuvant therapies in the treatment of testicular cancer have adverse effects on fertility; these are usually temporary but can be permanent. The germinal epithelium is extremely sensitive to chemotherapy, and most patients will be rendered temporarily azoospermic immediately after cisplatin treatment, but 50% of men recover spermatogenesis after two years and 80% after five years.15 The testes are also exquisitely radiosensitive, and radiotherapy targeted to the retroperitoneal nodes may still impact spermatogenesis through internal scatter radiation.16 Historically, RPLND risked damage to the lumbar plexus, which could cause retrograde or anejaculation. Newer nerve-sparing techniques are now widely used, with ejaculatory function preservation rates approaching 95%.17
Most patients with treatment-induced infertility recover two years after treatment, but paternity can be delayed during a couple’s peak reproductive years. Contraception is recommended during this period, because of the lingering effects of chemo- or radiotherapy on sperm DNA quality.18 Semen cryopreservation (sperm banking) remains the method of choice for fertility preservation, but it is widely underused – only about one-third of patients with testicular cancer bank sperm.19 GPs can encourage patients at the outset of their testicular cancer diagnosis to consider sperm banking, and screen for oligo- or azoospermia with a semen analysis, hypogonadism with a sex hormone panel (follicle stimulating hormone, leutinising hormone and testosterone levels) and hepatitis B, D and HIV in anticipation of semen cryopreservation.
Follow up and long-term problems
Patients with testicular cancer have a high overall survival rate for low stage cancers. For both seminomas and nonseminomas, five-year overall survival rates of 98% and above and 95% and above are observed for stage I and IIA/IIB cancers, respectively. Even for advanced testicular cancers with good- or intermediate-risk (stage IIC and III), five-year survival is greater than 65%.
For testicular cancer survivors, follow up usually consists of regular physical examination, including abdominal and chest examination, imaging and screening for serum tumour markers. Examination of the remaining testicle is imperative as the cumulative risk of malignancy in that testis is around 2% by 15 years after orchidectomy.20 For this reason, survivors should be encouraged to regularly perform a testicular self-examination, as should first-degree relatives who are at higher risk of testicular cancer.
Patients with stage I tumours who are on active surveillance have less than 1% risk of recurrence after five years and may therefore be discharged from specialist care, with imaging and screening for serum tumour markers performed only when clinically indicated. Patients who received cisplatin-based chemotherapy or radiotherapy as part of their treatment are 1.5 to 2.0 times more likely to develop cardiovascular disease compared with those that did not, and are at increased risk of developing secondary malignancies, such as prostate, colorectal, melanoma, kidney and lymphoma.8,21 Identification and treatment of modifiable cardiovascular risk factors and vigilance for the red flag symptoms of other cancers (such as weight loss, cachexia, fatigue) are important roles for the GP in managing survivors of testicular cancer.
Quality of life studies of survivors of testicular cancer indicate that, for the average patient, quality of life deteriorates during diagnosis and treatment, but returns to normal after treatment.22 However, chronic or late side effects, particularly from chemotherapy, compromise survivors’ quality of life. Hearing loss or damage, neuropathy, cardiovascular disease, diabetes, thyroid disease and depression and anxiety are potential domains of significant morbidity after standard cisplatin-based chemotherapy to treat testicular cancer.23 Compared with the general population, higher rates of chronic fatigue and anxiety disorders are observed in survivors of testicular cancer. Hypogonadism is a common problem, seen in 10% of patients managed with orchidectomy alone, and up to 33% of chemotherapy-treated patients.24 Potential manifestations, including depression, sexual problems and diminished physical wellbeing, should be monitored for. Patients should be tested for hypogonadism with morning serum testosterone and leutinising hormone measurement and, if appropriate, treated with supplemental testosterone.
Conclusion
Although testicular cancer predominantly affects young men, survivorship is high even with advanced disease. GPs play a key role in the detection of disease and in monitoring and treatment of long-term issues affecting testicular cancer survivors. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.