Ménière’s disease. A guide to management

Meniere's disease
Hearing disorders and deafness
Ménière’s disease is an uncommon cause of recurrent vertigo that should be distinguished from other common causes of balance disturbance, such as vestibular migraine and positional vertigo. Stepwise introduction of dietary restriction of sodium, lifestyle changes and medication can reduce the frequency and severity of attacks in most patients. Hearing loss can be treated initially with hearing aids and, in the later stages, a cochlear implant.
- Ménière’s disease is characterised by recurrent attacks of vertigo, fluctuating hearing loss, tinnitus and a sensation of aural fullness.
- Attacks are sudden in onset, typically accompanied by an intense sensation of movement, nausea, vomiting, diarrhoea and sweating, and can last hours.
- Treatment options for acute attacks include ondansetron, prochlorperazine and diazepam.
- In most patients, attack frequency and severity can be reduced by a stepwise approach of dietary restriction of sodium, lifestyle changes and medication; surgical treatment is rarely required.
- Referral to a specialist is best for initial diagnosis and evaluation.
- GPs have an important role in ongoing management of patients with Ménière’s disease.
Ménière’s disease is characterised by recurrent attacks of vertigo accompanied by fluctuating sensorineural hearing loss, tinnitus and a sense of aural fullness. Prosper Ménière in 1861 correctly attributed the attacks to a disorder of the inner ear, suggesting that the mechanism of causation could be similar to migraine or inner ear vasospasm, a differential diagnosis which is still relevant for the disease today.1
Meniere's disease today
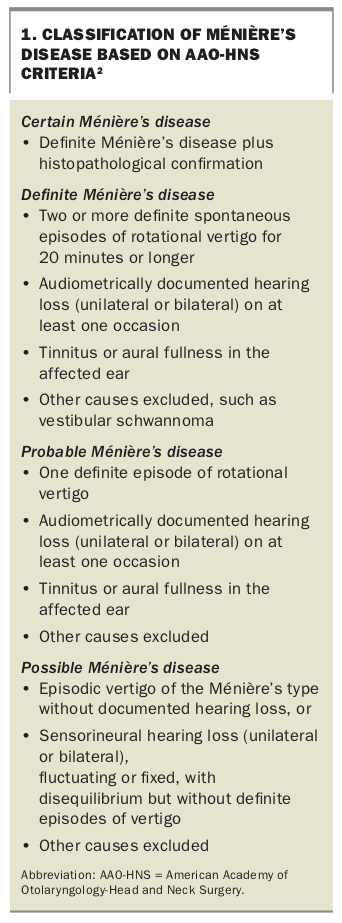
The differential diagnosis of vertigo is broad, often leading to all cases of vertigo being labelled as Ménière’s disease. To clarify the diagnosis, treatment and prognostication of patients with Ménière’s disease, the American Academy of Otolaryngology – Head and Neck Surgery (AAO-HNS) published guidelines for the classification of Ménière’s disease (Box 1).2 Although the category of ‘certain Ménière’s disease’ is used only as a research definition, as it requires postmortem histological examination of the temporal bone, the other categories are clinically useful.
{kind=link}
Clinical features and natural history
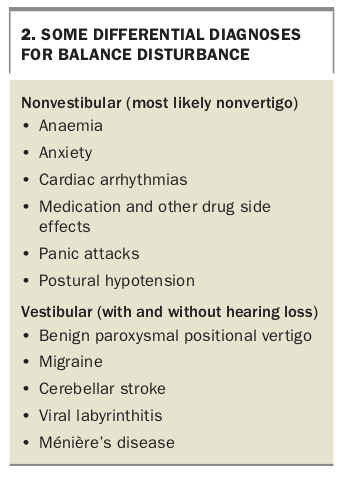
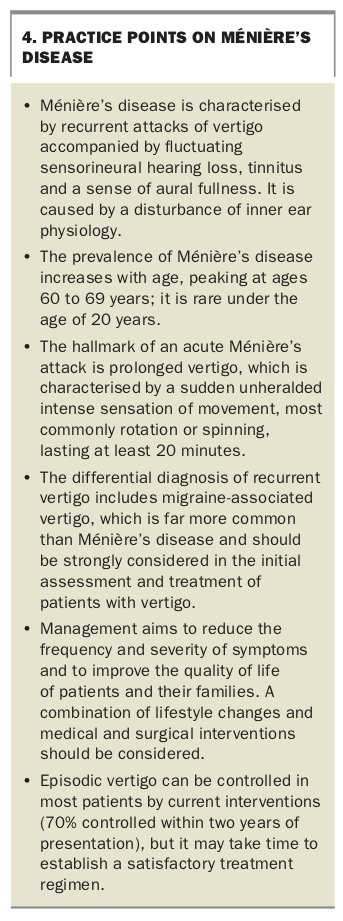
The hallmark of an acute Ménière’s attack is prolonged vertigo. The vertigo is characterised by a sudden unheralded intense sensation of movement, most commonly rotation or spinning, lasting at least 20 minutes and accompanied by nausea, vomiting, diarrhoea and sweating. The duration and character of the vertigo is important in the diagnosis of Ménière’s disease because episodes lasting a few seconds or minutes are more likely to be due to benign paroxysmal positional vertigo (BPPV) or, if longer than eight to 12 hours, to vestibular neuritis or cerebellar stroke. Feelings of light-headedness, pressure or vague disturbances of balance are more likely to be due to nonotological causes, such as postural hypotension, hyperglycaemia, hyperventilation, panic attacks or anxiety.
In the early stages of Ménière’s disease, patients may report only the vertigo symptoms, as the fluctuations in hearing thresholds are minor and may go unnoticed. However, as the disease progresses the fluctuating hearing loss (generally affecting low tones) becomes more marked, and a permanent hearing loss may persist between attacks (middle stages of the disease). Later in the disease course, the hearing loss becomes permanent and nonfluctuating. At this stage, the attacks of vertigo usually lessen, and hearing loss becomes the dominant symptom (‘burnt out’ Ménière’s disease). The sensation of tinnitus similarly may be less noticed in the early stages, only to become more prominent in the later course of the disease.
Late in the disease, patients may experience drop attacks (caused by dysfunction of the vestibulospinal reflex), where a sudden loss of balance control causes them to drop to the ground without losing consciousness.
The natural history of Ménière’s disease is highly variable. Attacks of vertigo can occur daily in clusters over periods of several weeks or as isolated episodes interspersed with variable periods of remission, sometimes lasting many months or several years. In the later stages of the disease, the episodes of vertigo tend to ‘burn out’, and severe hearing loss dominates the clinical picture. In long-term follow-up studies of patients with Ménière’s disease, 30% to 45% developed the disease in the contralateral ear within a period of 30 years.
There are many variants of classical Ménière’s disease, in which vertigo precedes the fluctuations in hearing loss. The reverse occurs in Lermoyez syndrome: hearing loss precedes vertigo and improves following vertigo attacks. Some patients experience a fluctuation in their hearing thresholds (usually low tone) accompanied by tinnitus and fullness but no vertigo. This has been labelled ‘cochlear hydrops’.
Epidemiology
Several epidemiological studies of Ménière’s disease have been performed over the past few decades with widely contrasting results. Estimated prevalence rates range from as low as 3.5 per 100,000 population to as high as 513 per 100,000 population. The wide range is likely to result from methodological differences, changes over time in criteria for the diagnosis of Ménière’s disease, difficulty in distinguishing Ménière’s disease from related conditions such as migraine-associated vertigo, and differences in the populations surveyed. However, it is clear that Ménière’s disease is more common in women, and the prevalence increases dramatically with age, peaking in the 60 to 69 years age group.3,4 It is very rare in people younger than 20 years.
Pathophysiology
History
Before Ménière’s description of the disease in 1861 correctly attributed it to a disorder of the inner ear, vertigo attacks were thought to be due to a form of epilepsy.1 Ménière suggested the mechanism could be similar to migraine or vasospasm within the inner ear. Early treatments, including cervical sympathectomy and vasodilators such as nicotinic acid, were based on this understanding.
In 1938, the first reports of temporal bone histology in patients with Ménière’s disease were published, showing an increased fluid volume in the endolymph compartment of the cochlea, termed endolymphatic hydrops. It was assumed that increased endolymphatic volume led to the attacks of Ménière’s disease. However, further histological analysis of human temporal bones showed many examples of endolymphatic hydrops in patients with no clinical symptoms of Ménière’s disease.
In 1964, further histological studies showed evidence of ruptures of Reissner’s membrane, one of the membranous divisions between the potassium-rich endolymph and the perilymph of the cochlea. The ensuing ‘rupture theory’ proposed that the acute mixing of potassium-rich endolymph with perilymph leads to transient hair cell dysfunction within the cochlear and vestibular end organs, resulting in the attacks seen in Ménière’s disease. On the basis of this theory, many different forms of surgery to alter the function of the endolymphatic system were designed, with the aim of preventing pressure build up within the inner ear and minimising the membrane ruptures implicated in attacks of Ménière’s disease.
Current theories
As the understanding of the complex physiology of the inner ear evolved and the outcomes of various surgical and medical treatments for Ménière’s disease were reviewed, it seemed less likely that the rupture theory could explain the attacks of vertigo and fluctuating hearing loss. Contemporary understanding of the radial and longitudinal endolymph flow patterns in the healthy and diseased cochlea led to a theory in 1991 that Ménière’s disease is caused by episodic disturbances of endolymph formation and resorption.5 The theory encompasses current anatomical, physiological and pathophysiological knowledge about the functions of the cochlear and balance system. It also explains the stages of Ménière’s disease, including the occurrence of drop attacks late in the disease, and the responses to various treatments, particularly surgery to the endolymphatic system.
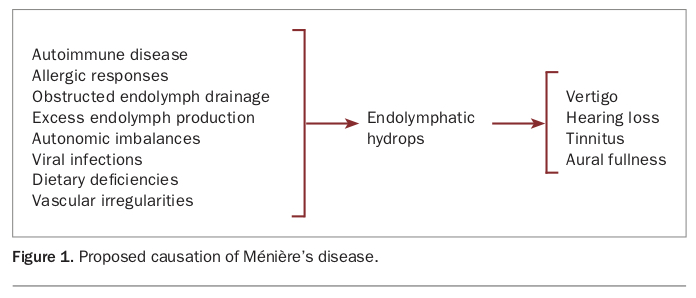
Although no single theory of Ménière’s causation is accepted by all workers in this field, a more contemporary concept of the disease is that it represents a failure of the complex inner ear homeostasis caused by any of a range of pathologies. The symptoms during an attack can be more usefully viewed as a syndrome than as a single disease entity. The inner ear changes leading to symptoms may be caused by a range of abnormalities (Figure 1). They include autoimmune diseases (Cogan’s syndrome and systemic lupus erythematosus), congenital rubella and other viral infections (possibly herpes simplex) of the inner ear (viral labyrinthitis), syphilis, chronic ear disease, acoustic neuroma, trauma, allergy and hormonal changes with the menstrual cycle. In most patients the cause is unknown.
{kind=link}
Diagnosis
In the vast majority of cases, Ménière’s disease can be diagnosed on the basis of an accurate history that looks for the AAO diagnostic criteria, and a few relevant tests to exclude differential causes of recurrent vertigo.2 Clinical examination of patients with Ménière’s disease often finds no abnormalities or at most shows evidence of a unilateral sensorineural hearing loss (or bilateral asymmetrical hearing loss in the case of bilateral disease). Clinical tests of balance such as Romberg’s test (standing feet together with eyes closed) and Unterberger’s stepping test (walking on the spot with eyes closed) may show only a mild disturbance of balance. This is because most patients are examined only between attacks, long after their symptoms have resolved. If there are associated persisting neurological signs (cranial nerve palsies or nystagmus) then other intracranial pathologies need to be considered.
In the few cases where patients have been observed during an acute attack, clinical examination has varying results. In general, patients appear quite unwell because of the unpleasant sensation of vertigo. They may be sweaty and pale, unable to stand up safely, nauseated and violently vomiting. There may be horizontal nystagmus that changes direction as the attack progresses. Following an attack, patients are left with a sense of ‘hangover’ for a day or two before recovering to normal function.
Investigations
Pure tone audiogram
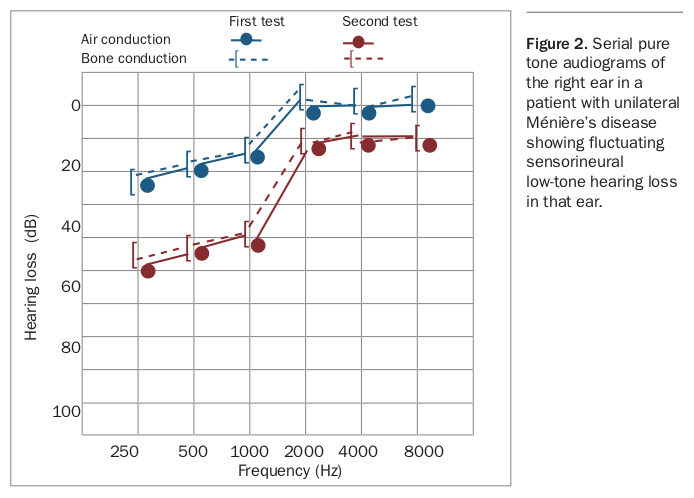
The most useful investigation for diagnosing Ménière’s disease is a standard pure tone audiogram. In classical Ménière’s disease, this may show varying degrees of sensorineural hearing loss. Most commonly the hearing loss affects low tones, although other patterns are also seen (Figure 2).
{kind=link}
Serial audiograms recorded at intervals during the progression of Ménière’s disease may show fluctuations in the degree of hearing loss. In the earliest stages of Ménière’s disease, an audiogram (typically recorded after the attack has abated) usually appears normal. As the disease progresses, the hearing loss becomes more marked with some degree of hearing loss persisting between attacks (middle stages of the disease). Later in the disease course, the hearing loss becomes permanent and nonfluctuating.
Vestibular function tests and electrocochleography
Vestibular function tests are highly specialised tests of the balance system and are particularly useful in evaluating patients whose cases are unusual, for example with an atypical clinical history or bilateral disease.6 Vestibular testing is mandatory before considering interventions that involve permanent ablation of vestibular function (e.g. surgery, labyrinthectomy or vestibular nerve division). Vestibular function tests are best ordered and interpreted by a specialist (a neurologist or ear nose and throat surgeon) with experience in managing otological conditions.
An electrocochleogram, which records the hair cell responses to sound, may also be useful in confirming the diagnosis of Ménière’s disease in atypical cases.6
Imaging studies
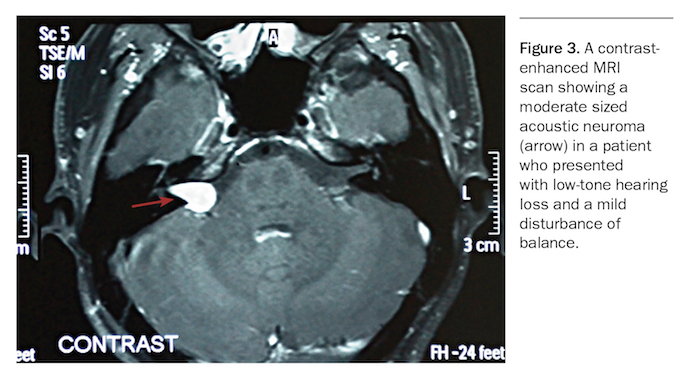
Imaging studies such as MRI and CT scans are useful in excluding acoustic neuromas (Figure 3) and other intracranial pathologies that disturb balance and hearing (e.g. acoustic tumours, hydrocephalus and multiple sclerosis). At current diagnostic resolutions, MRI imaging has no specific findings to indicate the presence of endolymphatic hydrops. However, there have been recent advances in MRI imaging using intratympanic injections of gadolinium contrast material, which have demonstrated dilation of the endolymph compartments in some patients with advanced Ménière’s disease (Figure 4).7 Further refinements of these imaging techniques may allow a more definite diagnosis in patients with Ménière-type symptoms, and strengthen the evidence base for the many treatments available for patients with Ménière’s disease.
{kind=link}
{kind=link}
Other tests
General haematological and biochemistry tests show no specific abnormalities in Ménière’s disease but are useful in evaluating patients for other causes of imbalance. A full blood count may show anaemia. Renal function tests are important for patients who may require treatment with diuretics as part of their overall management.
Differential diagnosis
Patients with disturbances of balance are extremely common in general practice, with many of the underlying causes being nonvestibular (Box 2). The key to evaluating the differential diagnosis of disturbed balance lies in obtaining an accurate history of the balance problem and associated symptoms (e.g. hearing loss, tinnitus and a feeling of aural fullness). Descriptions such as light-headedness, disorientation and floating are likely to have nonvestibular causes, whereas a history of vertigo (a true sense of movement, spinning, rocking or tilting) is highly likely to be due to a disturbance of the vestibular system, including Ménière’s disease.
{kind=link}
Further clues in the history, such as the duration of the vertigo, its frequency (rate of recurrence), positional elements, and the association of hearing loss, tinnitus and aural fullness, allow Ménière’s disease to be distinguished from other vestibular causes of vertigo such as BPPV, vestibular neuritis and cerebellar haemorrhage.6 Vestibular migraine can mimic early Ménière’s disease but can usually be distinguished by its response to antimigraine medication (see below).
Simultaneous loss of vestibular and cochlear function is most commonly due to Ménière’s disease but occasionally can have other causes. Herpes zoster causes pain, vertigo and hearing loss, with vesicles in the ear canal (and if accompanied by facial palsy is termed Ramsay Hunt syndrome). Meningitis due to bacteria or fungi, carcinoma, lymphoma or sarcoid can cause vestibular and cochlear dysfunction associated with other cranial nerve lesions. Vasculitides, including some ear- and eye-specific syndromes such as Cogan’s syndrome and Susac’s syndrome (retinocochleocerebral vasculopathy), and syphilis can mimic Ménière’s disease. Brainstem lesions involving the vestibular nerve root or nucleus, such as multiple sclerosis, rarely cause a similar syndrome.
Migraine and Meniere's disease
Over the past 25 years, awareness has increased that migraine can be associated with disturbances of balance, including dizziness, imbalance and vertigo, with or without headache, mimicking early Ménière’s disease. The overall prevalence of migraine in the general population is 13%, and a quarter of migraine patients experience dizziness or vertigo along with other more typical migraine symptoms. Because the prevalence of migraine in the general population is far greater than that of Ménière’s disease, a patient presenting with recurrent vertigo is much more likely to have migraine-associated vertigo than Ménière’s disease.
The distinction between vestibular migraine and Ménière’s disease may not be considered important in the early stages of Ménière’s disease as initial management strategies for the two disorders overlap (diet and lifestyle modification), and prescribed medications generally have few side effects. However, in the later stages of Ménière’s disease, when more invasive and irreversible treatments are being considered (e.g. gentamicin or surgical labyrinthectomy or endolymphatic sac surgery), it is crucial that the two be distinguished. If doubt exists, a trial of antimigraine management should be undertaken before considering irreversible interventions for Ménière’s disease. Vestibular migraine was discussed in detail in a previous issue of Medicine Today.8
Management
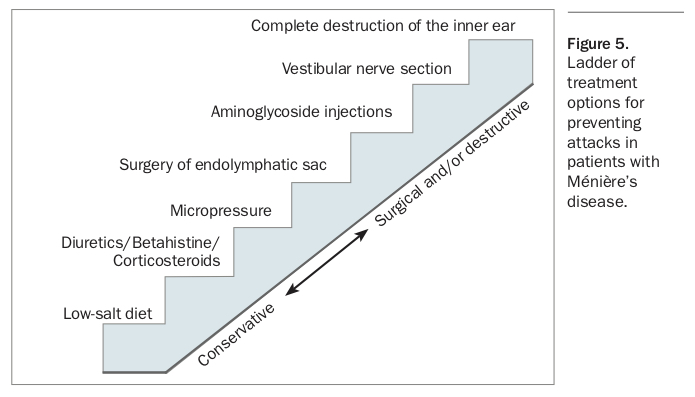
Modern management of patients with Ménière’s disease aims to reduce the frequency and severity of symptoms and to improve the quality of life of patients and their families. A flexible management strategy needs to be formulated for each patient and for different stages of the disease. Treatments are best considered from a symptom control viewpoint, leading to a stepwise introduction of available therapies depending on their toxicities and ease of administration (Figure 5).
{kind=link}
In general, episodic vertigo can be controlled in most patients by current interventions (70% controlled within two years of presentation), but it may take time to establish a satisfactory treatment regimen. In the advanced stages of Ménière’s disease, especially when it is bilateral, hearing loss has greater impact, often requiring powerful hearing aids or at times a cochlear implant. Tinnitus and the sensation of aural fullness are more difficult to manage. Patients often habituate to these symptoms, but they can persist and remain troublesome.
Treatment of acute vertiginous attacks
The dominant symptom during acute attacks is vertigo. This is usually associated with intense nausea, vomiting, sweating and sometimes diarrhoea. As the attacks are usually unheralded, it is wise to advise patients of strategies:
- to ensure their safety (especially while driving or working in situations of danger)
- to allow the attack to pass (which may take several hours) and recovery to ensue (often after a period of a day or two of feeling ‘washed out’).
Once an attack is established, little can be done to alter its natural course. Vestibular suppressants with antinausea effects (ondansetron [off-label use], prochlorperazine) are useful. My preferred strategy is to use sublingual ondansetron wafers (4 to 8 mg three times daily), as these can be taken despite intense nausea and have a rapid onset of action. Diazepam 2 mg orally twice daily for 24 hours is a reasonable alternative (off-label use). Rarely, hospital admission for a severe or prolonged attack is necessary for intravenous rehydration, especially for elderly patients or during hot weather.
Preventive strategies
Education, lifestyle changes and support societies
Patient education is an important part of the management of Ménière’s disease. Knowledge about the disease, likely natural history and treatment options and dispelling of myths surrounding treatment are important to improve the quality of life of patients and their families. Accurate information can help alleviate the feelings of frustration and helplessness experienced by many patients at first diagnosis.
Simple interventions such as regularity with diet, sleep and exercise go a long way to improving patients’ coping mechanisms. Stress, both physiological and emotional, plays a role in triggering attacks. Formal stress management programs delivered by a psychologist and tailored to patients’ individual requirements can be helpful. A regular and vigorous exercise program is also useful in helping patients regain confidence in their sense of balance. A regular brisk walk of 30 minutes, three to five days each week, is achievable by most patients. Formal vestibular exercises, conducted by a physiotherapist, may be useful for those who need help designing a specific and sustainable training program.
Support societies such as Meniere’s Australia (www.menieres.org.au) provide useful and accurate information for patients about vertigo, hearing loss, tinnitus and management of Ménière’s disease. They can also provide reassurance for patients and their families (Box 3).
{kind=link}
Low-salt diet
A simplistic understanding of diet and Ménière’s disease suggests that dietary salt intake is related to the degree of endolymphatic hydrops and influences the frequency and severity of vertiginous episodes. Although there is little formal evidence to support this view, there is anecdotal evidence from clinical practice, with some patients reporting acute attacks of Ménière’s disease following a salt binge.
Sensible recommendations for dietary sodium restriction suggest a salt intake ranging from 1 to 2 g/day. In practice, this involves following a ‘no added salt’ (NAS) diet, avoiding obviously salty foods, taking note of food labelling and avoiding processed and fast foods. Although food may initially taste bland and unappetising, most patients who persist habituate to the new dietary conditions after a few weeks. Input from a dietitian or an NAS recipe book can be useful. Reducing caffeine, caffeinated soft drinks, chocolate and alcohol intake seems to make a difference in some patients.
Diuretics
Diuretics have been a mainstay for treatment of Ménière’s disease since the early 1900s. Theoretically, the sodium loss produced by diuresis reduces the extracellular fluid in the body and in turn the amount of endolymphatic hydrops. Hydrochlorothiazide is the most widely used diuretic, but furosemide (frusemide), spironolactone and combination diuretics such as hydrochlorothiazide plus triamterene are also used (all off-label use). Careful monitoring of serum electrolyte levels is required. Despite the widespread use of diuretics, a recent Cochrane review found that there is no good evidence to support or reject their use in patients with Ménière’s disease.9
Betahistine
Vascular insufficiency to the inner ear has long been proposed as a mechanism for Ménière’s disease. Betahistine (a histamine analogue) has been used in this context for decades with the aim of improving inner ear perfusion. Testing in animals suggests that this improves blood flow in the stria vascularis of the cochlear duct. A recent clinical trial in humans showed betahistine to be useful in reducing the frequency and severity of vertiginous episodes and to some degree in helping tinnitus. There was no effect on hearing loss or aural fullness.
Betahistine has minimal side effects (gastric irritation), and the dose is easily varied, allowing it to be titrated against the frequency and severity of vertiginous attacks. It is available as 8 mg, 16 mg and 24 mg preparations. An initial regimen of 16 mg twice daily is a useful starting point, with the dose reduced by half each month. Higher doses may be useful for patients with more resistant disease. Betahistine has very little interaction with other medications, making it safe for use in older patients with Ménière’s disease.
Corticosteroids
Corticosteroid treatments for Ménière’s disease are a more recent intervention, based on the possible autoimmune basis of the disease and recent experience with use of intratympanic corticosteroids to treat sudden sensorineural hearing loss. In addition to their possible immune-modulating effects, corticosteroids are likely to influence the sodium and fluid dynamics of the inner ear through their mineralocorticoid properties, making them a theoretically attractive treatment. However, few clinical trials have investigated the use of corticosteroids for vertigo control to date. It may be reasonable to administer a short course of oral corticosteroids (prednisone 1mg/kg/ day for 10 days) or to consider intratympanic injection (dexamethasone 4 mg, single dose) for patients with Ménière’s disease who experience a sudden drop in hearing thresholds.
Hearing aids and tinnitus management
Later in the course of Ménière’s disease, hearing loss starts to become intrusive. Unilateral hearing loss has limited impact in quiet listening environments but becomes significant with background noise. Directional hearing and music appreciation are also impaired. Bilateral hearing loss in bilateral Ménière’s disease is more intrusive. Hearing aids can be useful in this situation, but a particular challenge is the fluctuating hearing loss seen in Ménière’s disease. This has been partially addressed with self-programming and adjustable hearing aids, which allow patients to adjust the power and processing setting of the hearing aid to suit their current hearing thresholds. If hearing loss is severe then cochlear implants are highly effective in restoring hearing.10
Tinnitus can be a particularly distressing symptom. Management strategies include education, sound therapy, short-term drug therapy with benzodiazepines or sedating antidepressants, tinnitus retraining therapy and cognitive behavioural therapy.11
Semi-invasive and surgical treatments
Grommets
Several nonevidence-based surgical operations and ‘sham’ procedures have been used in the past with some benefit, most likely because of a strong placebo effect. Most have now become historical, but insertion of grommets (tympanostomy tubes) is still used and may have a benefit on vertigo control and aural fullness. As it is a simple procedure able to be performed under local anaesthesia, is temporary and has a low risk of complications (persistent perforation, otorrhoea) grommet insertion is worth considering.
Micropressure therapy
Micropressure therapy is a minimally invasive therapy for Ménière’s disease that uses a soft probe inserted into the external ear canal. This delivers pressure pulses to the inner ear from a portable pressure generator. Its use is based on the observation that pressure changes applied to the inner ear result in improved vertigo control in patients with Ménière’s disease. A standard ventilation tube (or pre-existing perforation of the ear drum) is required for a micropressure device to be used. A treatment cycle takes a few minutes and is repeated three times a day. Several studies have suggested beneficial vertigo control with minimal risk of complications.
Aminoglycoside treatment
For patients in whom disabling vertigo continues to be the dominant symptom despite reasonable trials of medical management, chemical labyrinthectomy should be considered. Gentamicin is the most commonly used ototoxic agent. The aim of treatment is to gradually reduce hair cell function in the vestibular system of the affected ear. Gentamicin is relatively vestibulotoxic but leaves the cochlear hair cells intact, making it suitable for treatment of intractable vertigo in ears with functional hearing. Gentamicin can be administered under local anaesthesia by a transtympanic injection or via a grommet to the affected ear, thereby sparing toxicity to the unaffected ear in unilateral disease or the inactive ear in bilateral disease.
A commonly used fixed-dose transtympanic protocol involves a single injection of gentamicin (40 mg in a 2 mL solution, off-label use) to the middle ear, with a second injection four weeks later if the vertiginous episodes continue. Most outcome studies of gentamicin report greatly improved vertigo control. The effect on the vestibular hair cells is permanent and irreversible, with a small risk of associated hearing loss.
Endolymphatic sac surgery, labyrinthectomy and vestibular nerve section
Surgery on the endolymphatic sac has been a major treatment for intractable vertigo. However, more recent analysis of the outcomes of sac surgery have shown it to be no better than placebo treatments (simple mastoidectomy), leading to a decline in its popularity as a treatment of Ménière’s disease.
Complete unilateral surgical deafferentation of the vestibular system in the affected ears via labyrinthectomy or vestibular nerve section have also lost popularity. Although highly effective in controlling vertigo, these procedures carry the risk of total hearing loss, facial nerve palsy and neurosurgical complications related to entering the posterior fossa. Surgical treatment of Ménière’s disease has been largely replaced by transtympanic application of gentamicin, because of the latter’s ease of administration and relative safety.
Experimental treatments
Management of active Ménière’s disease focuses on reducing the frequency and severity of vertiginous attacks. This can be satisfactorily achieved in most patients with a combination of the interventions described above. However, in some patients with severe disease and particularly those with bilateral Ménière’s disease, disabling disequilibrium (poor balance) persists between each cluster of vertiginous attacks. This is usually because of insufficient residual vestibular function in longstanding end-stage disease.
A current experimental intervention is the vestibular electronic implant. This comprises an implanted device with three electrodes, one placed in each of the end organs of the affected semicircular canals, attached to a microprocessor (analogous to a cochlear implant), which can sense changes in head posture and position. The aim of the device is to simulate vestibular function during head movement with the hope of improving balance control and quality of life in patients with end-stage vestibular disease.
Role of the GP
GPs have an important role in the management of patients with Ménière’s disease. It is important to recognise the chronic nature of Ménière’s disease and to differentiate it from more common causes of transient vertigo, such as BPPV, vestibular neuritis and vestibular migraine. Providing education about the natural history of Ménière’s disease, ways of implementing and sustaining dietary (low sodium) and lifestyle (regular sleep and exercise) changes can go a long way to improving patients’ quality of life.
Referral to a specialist is preferable to establish the correct diagnosis and to formulate a treatment plan. Some practice points about Ménière’s disease are summarised in Box 4.
{kind=link}
Conclusion
An attack of Ménière’s disease can be a frightening experience for patients and their families. It occurs suddenly and without warning. Later in the disease, hearing loss and tinnitus can become intrusive, particularly in bilateral cases. In patients with classical Ménière’s disease, a careful history and a simple audiogram are usually sufficient to make the diagnosis. A carefully designed, stepwise treatment plan involving dietary and lifestyle changes and medication can stabilise the symptoms and greatly improve patients’ quality of life. MT