Cochlear implants – the best option for severe hearing loss in adults

Ear disorders
Hearing disorders and deafness

Severe hearing loss can have a major impact on a person's employment and quality of life. The surgical implantation of an electronic prosthesis into the inner ear, commonly known as cochlear implantation, is now the intervention of choice for adults with severe-to-profound levels of hearing loss. GPs play an important role in identifying potential candidates for cochlear implantation and encouraging them to seek specialist advice.
- Severe hearing loss can affect quality of life and growing evidence suggests that it is also associated with cognitive decline in older adults.
- Cochlear implantation is the intervention of choice for older adult patients with severe-to-profound hearing loss, with a significant increase in the number of patients aged over 70 years receiving the implant.
- The fundamental indication for cochlear implantation is bilateral severe-to-profound hearing loss for which well-adjusted hearing aids have given little or no benefit.
- Well-selected candidates with reasonable expectations can achieve highly satisfying outcomes from cochlear implantation, including benefits to auditory communication within their work and social environments.
- GPs have an important role in recognising potential candidates for cochlear implantation and facilitating their preliminary investigations.
Hearing loss is common in the community.1 When mild, it responds well to a hearing aid and the disability associated with it can be minimised. However, disability increases with the extent of the hearing loss and when the loss is severe, it can have a major impact on a person's employment and quality of life. Safety in dangerous environments also becomes a significant issue.
The surgical implantation of an electronic prosthesis into the inner ear, commonly known as cochlear implantation, is now the intervention of choice for patients with severe-to-profound levels of hearing loss. For the severely deafened patient for whom the most powerful hearing aids have failed, the outcomes of implantation are often dramatic with beneficial improvement in hearing and communication ability. These benefits are shared with the recipient’s family, social associates and work colleagues.
When first developed, the focus of cochlear implantation was on paediatric age groups. However, the past 20 years has seen an increasing number of adult candidates identified and successfully implanted, with the largest number being aged 60 years or older (Figure 1). With an ageing population in Australia, this trend is likely to continue (Figure 1 and Figure 2).
{kind=link}
{kind=link}
How do we hear?
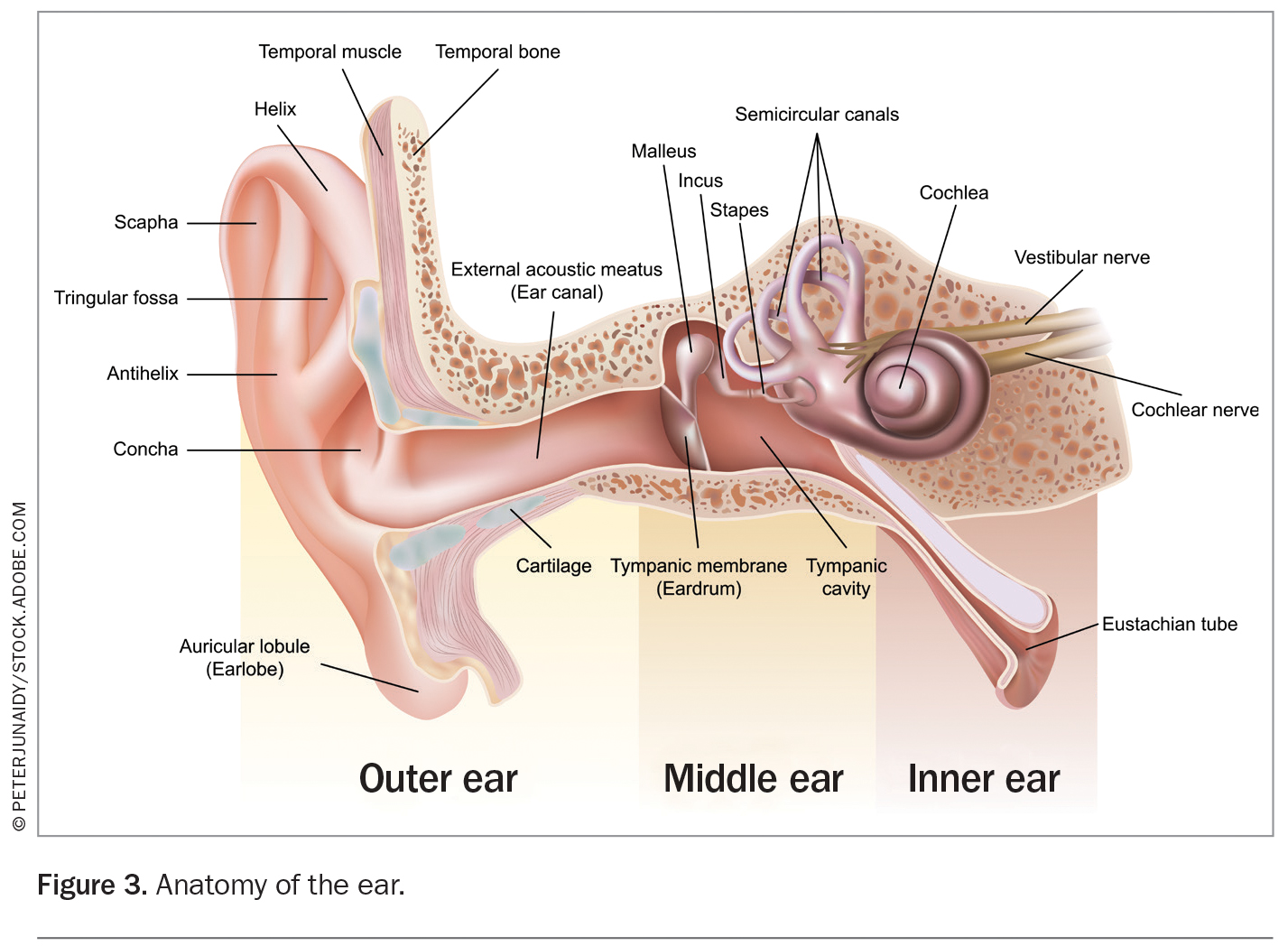
Hearing requires sound to be transmitted mechanically through the external and middle ear components (the conductive components) to the inner ear (Figure 3). Within the inner ear, the mechanical sound energy is converted to electrical signals by the hair cells (the sensory components) in the organ of Corti (the end organ of hearing within the cochlea), which in turn leads to stimulation of the auditory nerve and higher neural pathways, ultimately reaching the auditory cortex in the temporal lobe.2
{kind=link}
Disruption to the conductive hearing mechanisms (e.g. caused by otitis media, perforations or otosclerosis) produces hearing loss that is mild-to-moderate in degree and responds well to treatment with surgery or hearing aids. In contrast, problems affecting the sensory mechanisms in the inner ear (e.g. caused by ageing, genetics, noise exposure, Ménière’s disease, trauma, meningitis or ototoxicity) may produce severe-to-profound hearing loss, which responds poorly to hearing aids and is associated with a significant reduction in quality of life. It is for patients with this latter type of hearing loss that the cochlear implant has been designed and developed.
How do we go deaf?
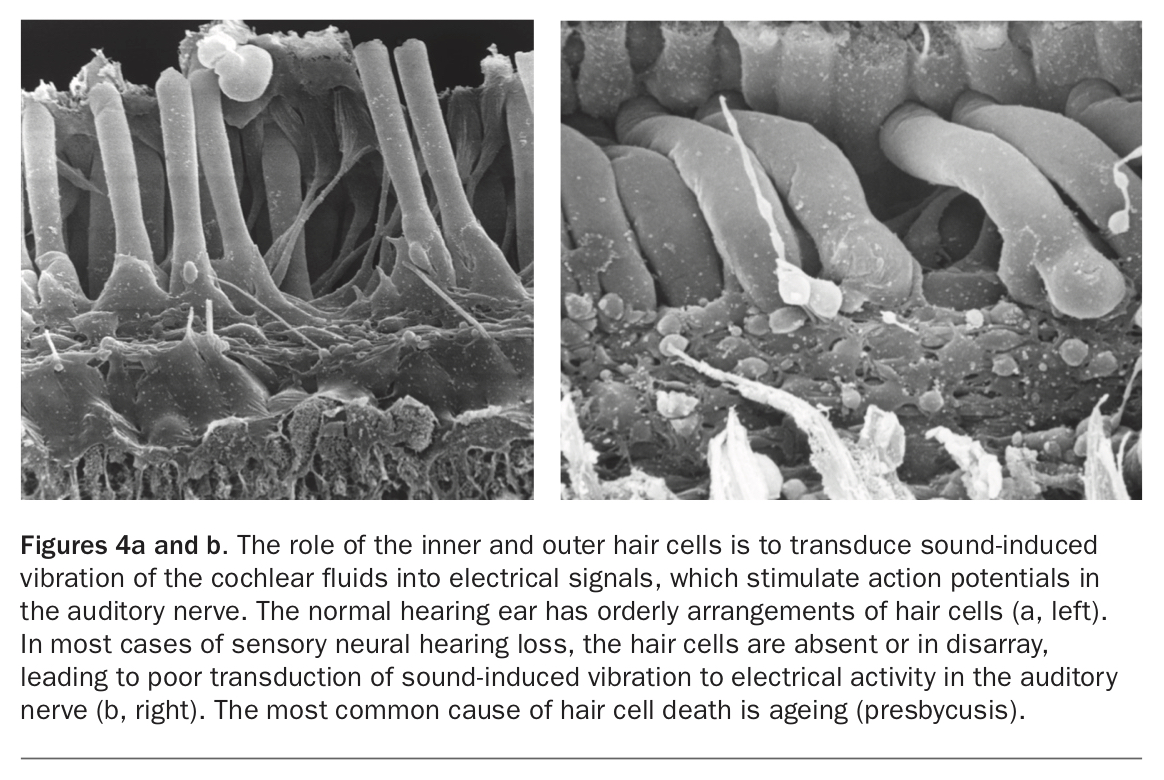
Most causes of acquired hearing loss involving the sensorineural parts of the hearing pathway are due to hair cell lesions of the inner ear (Figure 4a and b). The hair cells within the organ of Corti are vulnerable to a variety of toxicities. In some cases of profound hearing loss there may be a single identifiable causative agent that leads to hair cell loss and subsequent deafness, such as exposure to ototoxic agents (e.g. gentamicin, cisplatin) or following inflammation caused by meningitis. More often there are a variety of factors that together produce hair cell loss and profound hearing loss or, alternatively, the deafening aetiology is unknown. One common pattern of hearing loss is the effect of ageing (presbycusis) added to a pre-existing, nonaging factor for hearing loss, such as noise exposure with a background genetic susceptibility leading to early hair cell dysfunction.
{kind=link}
Sustained stimulation of the higher neural pathways linking the inner ear and the auditory cortex is necessary for development of normal sound and speech perception. Most causes of deafness involve the hair cells within the cochlea, with the higher pathways remaining intact. However, hearing losses that occur very early in life are associated with poor maturation of these pathways, particularly at a cortical level. Hearing loss acquired before the acquisition of cortical speech perception (prelingual) is usually associated with disordered higher pathways and characterised by abnormal speech quality, which in extreme cases can be completely unintelligible. Hearing loss acquired later in life, after the acquisition of speech (postlingual), is usually associated with well-formed higher pathways and characterised clinically by normal speech quality.
The separation of these two broad categories of hearing loss (prelingual versus postlingual) is an important factor in the selection and counselling of prospective cochlear implantation candidates. In general, candidates with postlingual deafness have predictable and satisfactory outcomes. With prelingual hearing losses, outcomes are more difficult to predict and can vary since they are dependent on many factors, including the age of the patient at implantation. Although the outcomes with regard to speech perception may be limited because cortical perception of speech sounds is poorly developed, the individual’s appreciation of environmental sounds allows many adults with prelingual deafness to derive considerable auditory benefit from cochlear implantation. However, the prospective candidate should receive careful counselling to ensure their expectations are realistic.
How common is hearing loss?
Hearing disorders are common in Australia, with over 3 million people (14%) reporting at least one long-term hearing disorder.3 The proportion of people with long-term hearing disorders increases with age from 3% of children aged up to 14 years to 49% of adults aged 75 and over, and is higher in men (18%) than women (11%).3 The prevalence of hearing loss in the adult community increases from 17% in 50-year-olds to 48% in 60-year-olds and 64% in 70-year-olds.4 The most common hearing disorder is complete or partial deafness, which affects one in 10 people in Australia.3
Most of the affected population has a mild to moderate degree of hearing loss that is highly suitable for assistance with a hearing aid. Severe hearing losses (greater than 70 dB) affect a smaller proportion of the community but carry a greater disability burden. In the elderly, hearing loss is often combined with visual failure and cognitive decline. The impact of this combination of sensory losses on quality of life and independent living can be profound.
In adults of employable age, the impact of hearing loss on potential employment, quality of life and general function is much higher than has been commonly realised, and is equivalent to the disability burden of many health conditions recognised as national health priorities.5 For example, in terms of disability burden, mild hearing loss is comparable with mild asthma; moderate hearing loss is comparable with severe pain related to degenerative spinal disease (such as a slipped disc); and severe hearing loss is comparable with pneumonia or severe diabetes associated with visual failure.
Hearing loss and cognitive decline
Recognition of the association between hearing loss and cognitive decline is increasing. A longitudinal study of hearing changes and cognition over decades in the same population indicates a very strong correlation and a possible causative association.6,7 Hearing loss may place an additional load on the mental resources of a vulnerable brain such that the person with hearing loss has to work harder to decode and process sounds. This additional load may mean that there are reduced resources for memory and other cognitive functions, leading to brain changes presenting as dementia. Up to 9% of the global burden of dementia is linked to hearing changes of varying degree (https://www.thelancet.com/infographics/dementia2017).6 Whether the treatment of hearing loss will halt the progression of, or perhaps reverse, dementia is still being investigated.
How a cochlear implant works
A cochlear implant is an electronic prosthesis that works by bypassing the residual damaged hearing elements within the organ of Corti and directly stimulating the intact nerve endings in the auditory nerve. The device has two components:
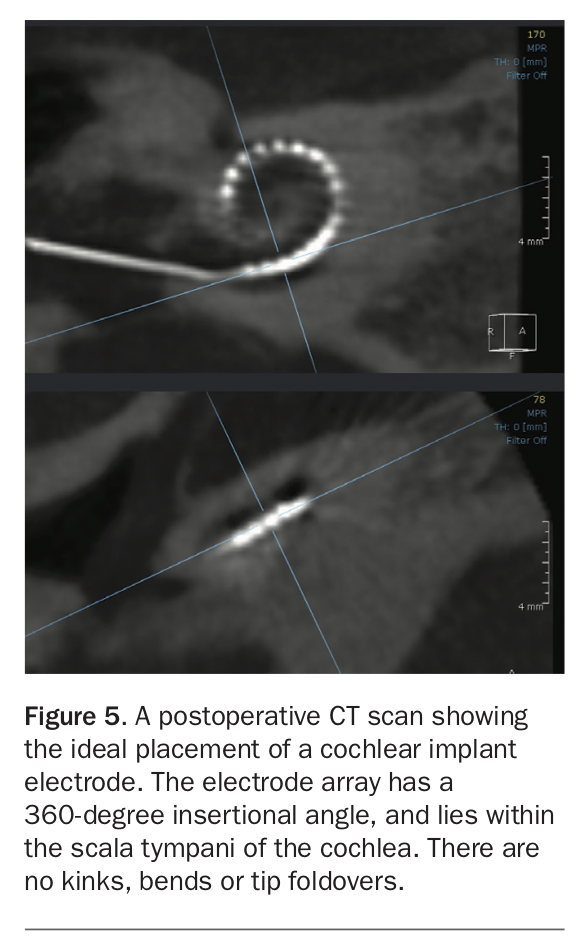
- a fully implanted intracochlear electrode attached to a receiver stimulator package, which is inserted during cochlear implant surgery (Figure 5)
- an external speech processor unit that sits behind the ear and looks like a sophisticated hearing aid (Figure 6).
{kind=link}
{kind=link}
Both components are required for the cochlear implant system to function properly. The microphone within the speech processor unit captures speech and environmental sounds (Figure 6). The sounds are then processed within the electronic package to a series of electrical pulses and transmitted wirelessly to the internal receiver–stimulator unit. The internal unit then further processes the signals and sends them down the multiple channels of the intra-cochlear electrode array (Figure 5), which in turn stimulates the intact auditory nerve endings. These intact auditory nerves carry electrical signals through the higher pathways and eventually the auditory cortex where they are perceived as speech and sound sensations.
The patient journey and when to consider a cochlear implant
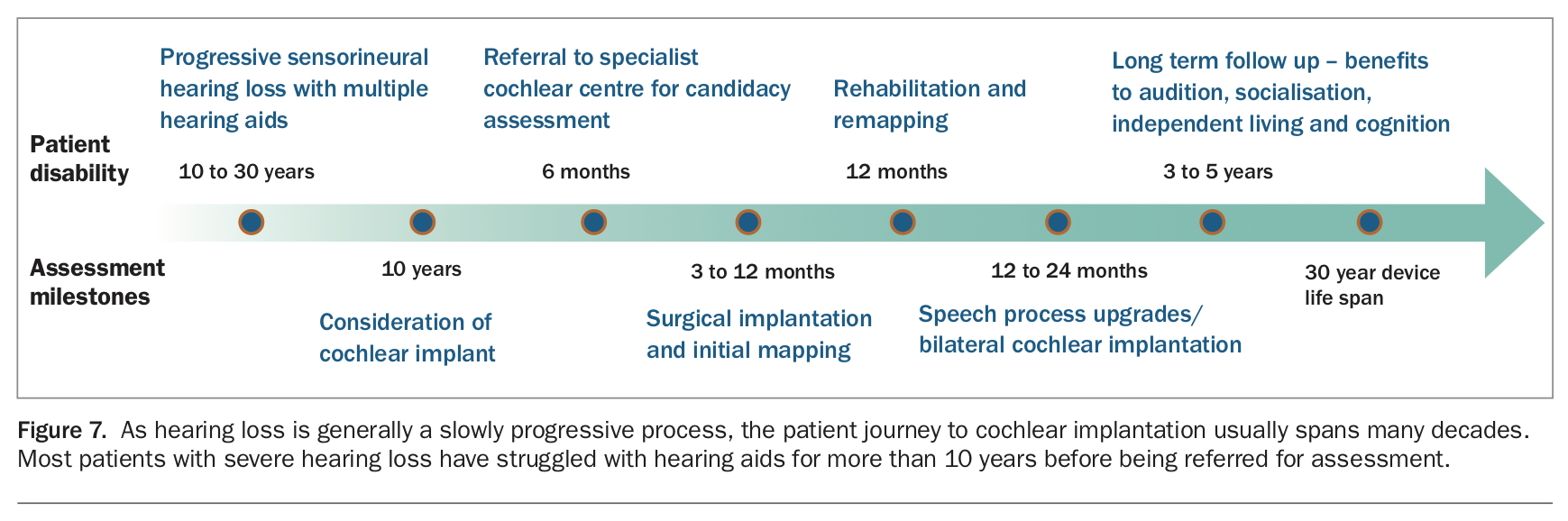
As hearing decline is usually a slow process, the patient journey to cochlear implanting spans several decades (Figure 7). Initially, modifying listening environments or simply increasing the volume of phones, TV and other assistive listening device may compensate for mild hearing loss. Further progression of hearing loss impacts on the patient's family and work associates, prompting testing and the use of hearing aids. This might be all that is needed if the hearing loss stabilises; however, further decline in hearing will render the hearing aids ineffective, particularly when there is background noise or with higher frequency sounds such as children’s voices. Difficulty with phone usage follows.
{kind=link}
When a patient's hearing loss is severe-to-profound, the efficacy of hearing aids fails, phone usage is severely limited and, unless lip-reading skills are developed and maintained, general day-to-day aural communication becomes difficult. A cochlear implant should be considered at this point.
Many adult patients have had severe hearing loss for at least 10 years before receiving a cochlear implant. The opportunity cost of hearing disability, effect on cognition and impact on socialising is measurable. It is also notable that only one in 10 adult patients with hearing loss severe enough to qualify for a cochlear implant presents for assessment. The barriers to assessment are multiple, and measures to address these are being developed. The GP has an important role in recognising suitable candidates and prompting a referral to an ENT surgeon with an interest in cochlear implantation.
Indications for cochlear implantation
The fundamental indication for cochlear implantation is bilateral severe-to-profound hearing loss for which well-adjusted hearing aids have given little or no benefit. Establishing these criteria requires a detailed and rigorous assessment of aidable residual hearing. Specially designed tests of speech perception presented to each aided ear in isolation and both ears together, under a variety of controlled quiet and noisy conditions, provide quantification of residual hearing capacity. This preimplantation data can help predict the hearing outcomes after implantation.
All patients are carefully evaluated with CT and MRI to demonstrate normal cochlear anatomy and identify any factors that may preclude accurate placement of the stimulation electrodes before undergoing cochlear implantation. Potential sources of infection should also be evaluated. Any health factors that might interfere with the anaesthesia or surgery should be identified and managed beforehand. Prospective candidates for cochlear implantation should be well motivated and supported. They need to understand the commitment required for rehabilitation and auditory training once the implant is placed. Advanced age is rarely a limiting factor for cochlear implantation.
Use of a hearing aid in the contralateral ear or bilateral cochlear implants are highly successful interventions. Indications are also being expanded to include patients with single-sided deafness (with normal hearing on the contralateral side), moderate hearing loss and tinnitus occurring in association with severe hearing loss.
Devices that incorporate a fusion of a cochlear implant with a hearing aid assist patients with residual aidable hearing. As most of these patients have residual hearing in the lower frequencies with severe high-tone hearing losses, the aim is for the cochlear implant to rehabilitate the higher (speech) frequencies while preserving the lower tones. When successful, this combination of ‘electroacoustic’ hearing can produce a hearing result with near normal listening experience; however, the risks of losing functional residual hearing during surgery to place the implant should be accepted.
Recognising potential candidates
Adult patients with severe hearing loss should be considered for a cochlear implant when their hearing aids are optimally adjusted but still give poor hearing experiences in quiet listening environments. In common terms, this level of hearing impairment is reached when the patient is having difficulty understanding phone conversations with familiar voices and subjects. If readjustment of the hearing aids by the hearing aid provider fails to improve the situation then referral of the patient to an ENT surgeon with an interest in cochlear implantation should be considered. A recent audiogram as well as the results of previous hearing tests will be useful in determining the rate of progression of the hearing loss.
Cochlear implant surgery
Surgery to place a cochlear implant has evolved considerably since the first operations were designed 40 years ago. The procedure takes about two hours and recovery usually requires an overnight stay in hospital. It can take four to five days before most patients can return to their usual routine and social activities, including driving and work.
Surgery involves performing a limited mastoidectomy to access the middle ear cleft and cochlear structures. A small opening measuring about 1 mm in diameter (cochleostomy) is then drilled into the cochlea to allow placement of the intracochlear electrode close to the auditory nerve endings (Figure 5). The implant is tested to confirm its function and correct placement within the cochlea. Patients are typically given a general anaesthetic; however, more recently, surgery has been performed under local anaesthetic with the patient fully awake. This obviates the need for general anaesthesia and its potential to cause postoperative confusion or further cognitive decline in the very elderly patient. The surgery is well tolerated.
When the incisions from the procedure are fully healed, usually within two to three weeks, the implant device can be switched on and programmed (a process called mapping) to optimise the patient’s hearing outcome. Although useful sound and speech perception often occurs at the time of switching on the device, it usually takes many months to reach the best possible hearing outcomes. Persistence with the rehabilitation program is required.
Hearing outcomes
Many factors determine the hearing outcomes of cochlear implantation. These include the following:
- the nature of the hearing loss – including age of onset (pre- or postlingual), duration of deafness and degree of residual hearing
- patient factors – including age, level of cognition and auditory stimulation and persistence with the rehabilitation program
- the experience of the cochlear implantation team – including completeness of electrode insertion, type of implant and persistence with the rehabilitation program.
Well-selected candidates with reasonable expectations of what is involved in the cochlear implantation process can achieve highly satisfying outcomes, including benefits to auditory communication within their work and social environments. Previously employed and socially active adults often return to their usual work and social roles. Elderly patients and their families report a reduced sense of social isolation and the ability to continue living independently and safely as a result of the cochlear implant. Many patients can return to fluent listening over the phone and some to music appreciation. Quality of life, mood and sense of vitality and energy can also be enhanced following cochlear implantation. In general terms, people with well-performing cochlear implants can hear in quiet environments as effectively as matched patients with aided moderate hearing losses.3
Limitations
Limitations to cochlear implantation are important for patients to understand and accept before embarking on surgery. Although outcomes are clustered at the higher range of the hearing spectrum, some patients derive only modest benefit with perception of environmental sounds and very limited speech understanding. Occasionally, such patients become nonusers of their implant.
Several of the limiting factors will be known before implantation. Longstanding deafness (of several decades) and prelingual hearing loss, in which the patient’s speech quality is unintelligible, are two conditions in which the hearing outcomes are variable. Preimplant counselling is important in these patient groups, with the aims of implantation being awareness of environmental sounds and an aid to lip reading, rather than speech perception. The option of cochlear implant surgery under local anaesthesia is appealing to patients concerned about the potential effects of general anaesthetic agents.
Patient support associations such as Cicada (www.cicada.org.au) play an important role informing patients and families of the range of possible outcomes after cochlear implantation. Information about the assessment process, surgery to place the devices and the rehabilitation process following the switching on of the cochlear implant is conveyed by means of a series of informal social events and information sessions. Future candidates have the opportunity to meet previous cochlear implantation recipients and view their outcomes and experiences from both the patient and the family perspective.
The role of the GP
The GP has an important role in recognising potential candidates for cochlear implantation and facilitating their preliminary investigations – particularly basic audiometry and temporal bone imaging. For instance, difficulty hearing phone conversations with well-adjusted hearing aids is a reasonable trigger for a patient to be assessed for a cochlear implant. Two case studies illustrating the journey to cochlear implantation of adult patients with different causes of hearing loss are presented in Box 1 and Box 2.
{kind=link}
{kind=link}
The availability of funding streams for adults requiring cochlear implants has improved considerably. Higher levels of private health insurance cover most costs and public funding is available for uninsured patients, although waiting lists in some areas can be lengthy.
Conclusion
Although originally designed for paediatric cohorts, cochlear devices are being increasingly implanted with great success in adult patients who have severe hearing loss. This trend is likely to continue as the longevity in the ageing population increases, funding streams become available and the association between hearing and cognition strengthens. GPs have an important role in identifying patients who are suitable for cochlear implantation and facilitating referral to an appropriate ENT specialist. MT
COMPETING INTERESTS: None.
References
(Figure%203.15 (accessed August 2021).