Osteoporosis in older people – managing the risks

Osteoporosis
Bone diseases
Osteoporosis increases with age and people aged over 70 years are at high risk of nonvertebral and hip fractures. Management should be multifactorial and needs to consider the triad of osteoporosis, falls risk and the impact of a fall in older people. Pharmacological treatment can aid with increasing bone density, but adherence is key.
- Older people are at highest risk of minimal trauma fracture, requiring a multifactorial and multidisciplinary approach to fracture reduction.
- Bone mineral density testing is essential to screen for osteoporosis in this population.
- It is essential to address the triad of osteoporosis, falls risk and the impact of falls in older people.
- Safe mobility and exercise with appropriate supervision should be encouraged, and nutrition, calcium intake and vitamin D levels optimised.
- Osteoporosis medications can be chosen based on patient preferences to optimise adherence.
- Use of hip protectors should be encouraged, as the risk of falls-associated hip fracture cannot be abolished in most older people.
The skeletal system is metabolically active. Over a person’s lifetime, the skeleton is continually being repaired and remodelled in response to multifaceted stresses. Osseous tissue is replaced annually at a rate of about 10 to 20%, varying by site and type. Bone remodelling is an active and highly regulated process that includes resorption (osteoclasts) and formation (osteoblasts).1
Osteoporosis occurs when bone resorption overwhelms the bone formation capacity of the skeleton. This imbalance in bone turnover results in reduced bone density and microarchitectural deterioration of bone tissue, which leads to increased fragility and greater risk of fracture.2,3 The incidence of osteoporotic fracture increases with age, and one in three women and one in five men over the age of 50 years are affected.
Epidemiology of postmenopausal and age-related osteoporosis
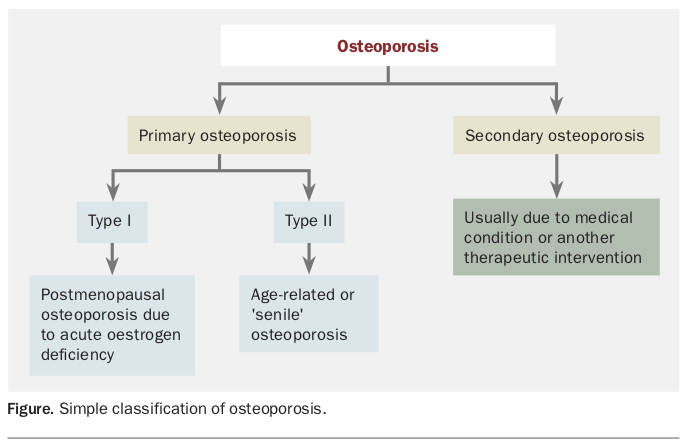
Osteoporosis is not a homogeneous disease (Figure). Postmenopausal (type I) osteoporosis tends to present differently from age-related or ‘senile’ (type II) osteoporosis.4 Postmenopausal osteoporosis is driven mainly by increased remodelling, with predominant bone resorption resulting in trabecular bone loss. In contrast, there is reduced remodelling in age-related osteoporosis, with bone formation disproportionately suppressed, resulting in predominantly cortical bone loss in both men and women.4 Based on this difference in pathogenesis, younger (50 to 75 years) postmenopausal women (with an increased rate of bone resorption) mainly experience vertebral fractures, whereas older patients (with a reduction in bone formation) have significantly higher rates of nonvertebral and hip fractures.5
{kind=link}
The prevalence of type II osteoporosis, which tends to occur in people aged over 75 years, is increasing because of longer life expectancy and an ageing population.6 In 2010, the number of people over 50 years of age who were considered to be at high risk of fragility fractures worldwide was 158 million, and this figure is set to double by 2040.7 Of the 75,000 fragility fractures that occur each year in Australia, about one-third are hip fractures. The annual incidence of fragility fractures increases with age.8 One-third of women and one- sixth of men will sustain a hip fracture by their ninth decade, and the rate of hip fracture doubles every five years after the age of 65 years.5,6,9,10 Osteoporosis is undertreated after all types of fragility fractures.
Risk factors for osteoporotic fracture
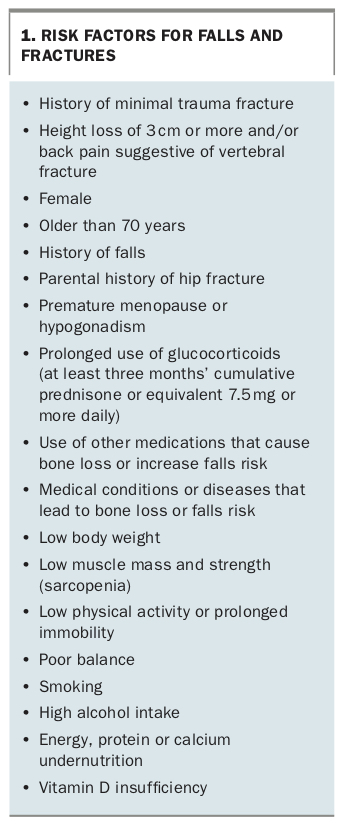
The main risk factors for fracture in older people are the triad of osteoporosis, falls risk and the impact from a fall. About 30% of older people living in the community and 50% of those in residential aged care fall each year, with an associated high risk of injury, including osteoporotic fracture.11,12 Hip fracture is the most common fracture in the very old. Residents of aged-care facilities and older hospitalised people are the frailest population and at highest risk of falls and fractures. They are also the most challenging to manage, as falls and fracture risks in this group are usually multifactorial, and the potential to reverse these risks is often limited. The risk factors for falls and fractures are summarised in Box 1.
{kind=link}
Diagnosis and assessment of fracture risk
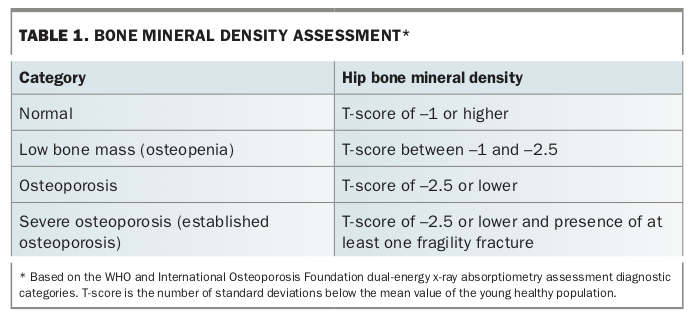
The gold standard for diagnosis of osteoporosis remains areal bone mineral density (BMD), measured by dual-energy x-ray absorptiometry (DXA).13 The WHO international reference standard for osteoporosis diagnosis is a T-score of –2.5 or lower at the femoral neck (Table 1). However, more than half of all minimal trauma fractures or subsequent fractures occur in people with a BMD T-score in the normal to osteopenic range. Hence, in the absence of a BMD measurement, the diagnosis of osteoporosis can be made on the basis of a fragility fracture. As most vertebral fractures are asymptomatic and diagnosed incidentally on spinal x-rays, a spinal x-ray may be a useful additional tool to identify fragility fractures.3
{kind=link}
For patients with ready access to bone densitometry, a DXA BMD measurement is recommended before starting therapy to enable monitoring of treatment, adherence and efficacy, even in cases of typical minimal trauma fracture (Flowchart). For patients in whom DXA BMD measurement is unreliable because of osteoarthritis, quantitative CT BMD measurement could provide more reliable information on the presence of hip or spine osteoporosis.
Absolute fracture risk is the most important determinant of an individual’s risk of fracture and is based on multiple factors.3 If there is uncertainty about patients with a prior fracture or osteopenia on BMD measurement, absolute fracture risk assessment may be useful for risk stratification and treatment decisions. The two calculators often used in Australia are the Garvan Fracture Risk Calculator (www.garvan.org.au/bone-fracture-risk) and the Fracture Risk Assessment Tool (FRAX; www.shef.ac.uk/FRAX).13-17 The Garvan calculator has an advantage over the FRAX in older populations as it includes people aged up to 96 years and stratifies risk based on the number of fractures and the number of falls. According to the US National Osteoporosis Foundation guidelines, an absolute risk of hip fracture greater than 3% and of any major fracture greater than 20% over 10 years is the threshold for intervention.3,18
Increased biochemical markers of bone turnover in the blood or urine have been shown in trials to be an independent risk factor for fractures in women and men. Although their use is controversial, bone turnover markers may have a role in assessing adherence and response to treatment and in helping guide choice of treatment.3,19
Nonpharmacological management of osteoporosis
Falls risk assessment and management
Community-dwelling older people
For community-dwelling older people, it is not sufficient to initiate pharmacological treatment of osteoporosis. Falls assessment and prevention are integral parts of the management of osteoporosis in older patients.20 There is evidence that group and home-based exercise programs and home safety interventions reduce both the rate of falls and the risk of falling in this group.11 Multifactorial assessment and intervention programs appear to be effective in reducing the rate of falls, but not the risk of falling. Tai chi reduces the risk of falling. Overall, vitamin D supplementation does not appear to reduce falls in older people living in the community, but it may reduce them in those who have low vitamin D levels before treatment is initiated.11 A recent Cochrane review concluded that exercise programs primarily involving balance and functional exercises, or multiple exercise programs including these two categories, reduce the rate of falls in older people living in the community (high-certainty evidence).21
Older people in aged care or hospital
A Cochrane review of studies of older people in aged-care facilities or hospitals found that vitamin D supplementation is probably effective in reducing the rate of falls.12 Evidence for multifactorial interventions in aged-care facilities suggests possible benefits but is inconclusive.
Exercise
The types of exercise that are best for bone strength are:
- weight-bearing exercise (e.g. brisk walking, jogging, skipping, basketball/netball, tennis, dancing, impact aerobics or stairs walking)
- progressive resistance training (e.g. lifting weights, ankle weights or gym equipment).22
Regular (two to three days per week) resistance training and balance training exercises that are moderate to vigorous, progressive (incremental over time) and varied have been shown to improve BMD and reduce falls and fracture risk. The strongest evidence for benefit is for people with mild to moderately impaired mobility. The frailest populations (e.g. highly dependent people in care institutions) have limited potential for benefit and may be at higher risk of falls and fractures from exercise programs if left unsupervised. This increase in risk may be caused by an overestimation of their ability after exercise or a lag in improvement in balance despite an improvement in strength.23,24
Hip protectors
Hip protectors, which protect against hip fractures by directing the force from a fall away from the hip, have been proven to be of benefit in a select group of older people in nursing or residential aged care but not in those living in the community.25-27 They are only effective with good adherence, which is difficult to achieve, but their use should nevertheless be encouraged if appropriate.
Pharmacological management of osteoporosis
Calcium and vitamin D supplementation
Lifestyle factors and frailty mean older people are at higher risk of calcium and vitamin D deficiency, in addition to being at higher risk of osteoporosis and fracture. There is a high prevalence of vitamin D insufficiency and deficiency in institutionalised and housebound older people, and vitamin D supplementation is considered standard care in these groups.28 Calcium levels are often suboptimal because of limitations in dietary intake, along with low vitamin D levels from limited sunlight exposure resulting in reduced calcium absorption.
It is especially important to resolve calcium and vitamin D deficiencies in patients with chronic kidney disease and those receiving antiresorptive therapy (ART), as they are at higher risk of hypocalcaemia and secondary hyperparathyroidism. Dietary calcium intake and serum 25-hydroxyvitamin D level should be checked before initiating osteoporosis therapy, with appropriate supplementation to be recommended if either is inadequate (Flowchart).29 However, caution is warranted when considering supplementation and dosage because of the reported increased risk of complications, including gastrointestinal and cardiovascular events, renal (stones) and falls.30-35
Bone-specific treatments
In Australia, a range of medicines to treat osteoporosis are subsidised by the government on the PBS.6,20,36-38 It is important that these medications are taken as directed to ensure the greatest benefit.6,39,40 Osteoporosis medicines can increase bone density and, although the increase may appear small, it can have a positive effect on reducing fracture rate. Medication can increase bone density in the hip by about 1 to 3% and in the spine by 4 to 8% over the first three to four years, but reduce spinal fractures by 50 to 70% and hip fractures by 30 to 50% (a positive effect can be seen as early as six to 12 months after starting treatment).40
Osteoporosis medicines are grouped into different classes depending on their active ingredient. The ARTs – bisphosphonates, monoclonal antibodies such as denosumab, selective oestrogen receptor modulators and oestrogens – reduce bone breakdown (loss).
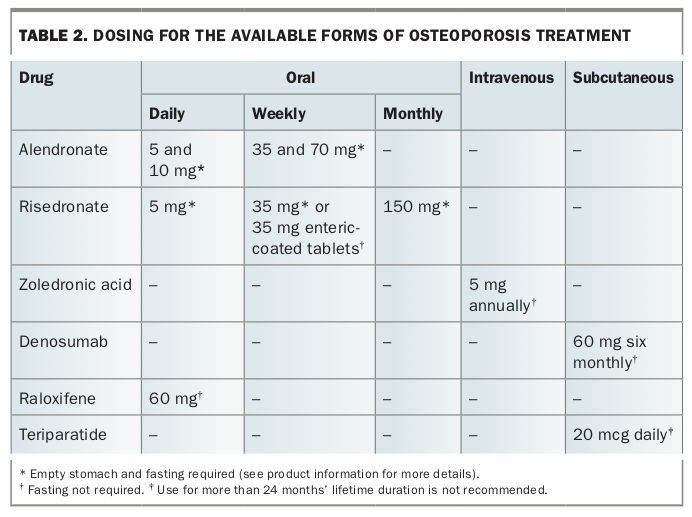
Bisphosphonates (alendronate, risedronate and zoledronic acid) are administered orally on a daily, weekly or monthly basis or as an annual infusion (Table 2). Adherence to fasting or other requirements of some of these oral agents is essential to maximise benefit, as they are otherwise poorly absorbed. Enteric-coated risedronate tablets (oral weekly) and intravenous zoledronic acid do not require fasting.
{kind=link}
Denosumab (six-monthly subcutaneous injection; Table 2) works differently from bisphosphonates but has the same effect of slowing the rate at which bone is broken down, with similar reductions in the risk of fractures.6,36-38,41 Adherence to timing and frequency of denosumab is essential. It is risky to miss doses or stop treatment abruptly as the benefit is quickly lost and may increase the risk of spinal fracture in some patients.
Raloxifene, a selective oestrogen receptor modulator, is only available on the PBS for postmenopausal women with a minimal trauma fracture. It acts on bone in a similar way to that of the hormone oestrogen, slowing bone loss and reducing the risk of spinal fractures in women who have been through menopause. It has been shown to be effective in reducing vertebral fractures but not nonvertebral fractures in osteoporotic postmenopausal women.42
Menopausal hormone therapy (MHT) helps to slow bone loss and reduce the risk of osteoporosis and fractures in women who have gone through menopause. The active ingredient is oestrogen. For women with an intact uterus, combinations also contain progesterone (combined MHT). MHT is safe and effective for most women under the age of 60 years who have osteoporosis and also need relief of menopause symptoms. It is not usually recommended to commence MHT in older women (those older than 60 years or more than 10 years after menopause), in whom caution is needed regarding the risk of heart disease, stroke and breast cancer and for whom other treatments may be considered.
Teriparatide is a self-administered daily injection for up to 24 months. In contrast to the ARTs, it is the only medicine available in Australia that stimulates bone formation, resulting in improved bone strength and structure. It is only available for people with severe osteoporosis (recurrent minimal trauma fracture despite at least 12 months of ART, and a BMD T-score of –3.0 or lower) when other osteoporosis medicines have not worked and the risk of further fractures is still very high. It can be taken for a maximum of 24 months in Australia but is only subsidised for 18 months on the PBS. Once the treatment is completed, another osteoporosis medication must be started to ensure that the new bone gained is maintained and improved. Otherwise, the benefit is lost within 12 to 24 months.
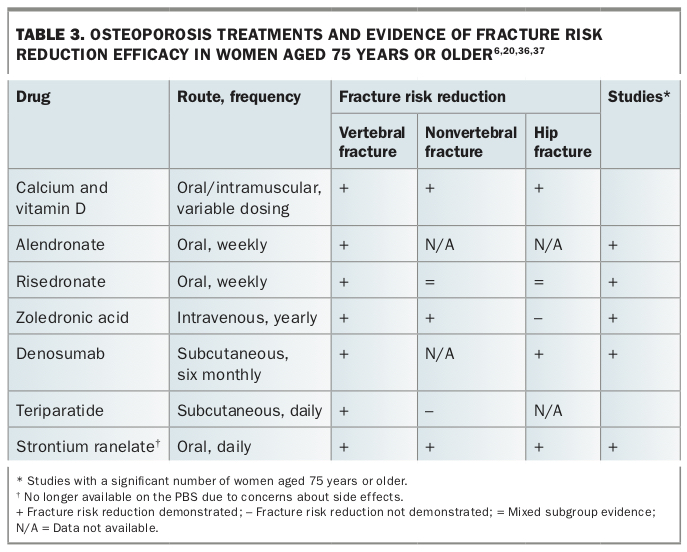
Despite the high absolute fracture risk in older adults, there is a paucity of evidence-based literature, randomised controlled trials and head-to-head studies of osteoporosis treatments that examine fractures in older patients as an outcome. Few studies include patients aged over 70 years; in those that do, the numbers are often small and infrequently analysed as a subgroup. Most of the evidence is based on pooled analyses. However, a review of the published literature on the clinical efficacy and safety of specific osteoporosis treatments in reducing fracture risk in women aged 75 years or older confirms the benefit of treatment (Table 3).6,20,36,37
{kind=link}
Denosumab and strontium ranelate (which is no longer available on the PBS due to concerns about side effects) are the only agents for which randomised controlled trials have been specifically designed and powered to show a reduction in the risk of hip fracture in people aged over 75 years. Risedronate has been shown in a post hoc analysis to be beneficial in a mixed cohort of patients aged between 70 and 100 years (mean age, 77 ± 5 years) with severe osteoporosis, compared with those aged over 80 years with risk factors only.43
For nonvertebral fracture, there is evidence of fracture risk reduction in people aged 75 years or older with the use of strontium ranelate and zoledronic acid, and in patients aged 70 to 79 years for risedronate.6,20,36,44-48 There are inadequate conclusive data for most agents in terms of nonvertebral fracture risk reduction, but all available agents are effective for reducing vertebral fracture risk.
Notwithstanding the limitations of these data, all agents have shown benefit in unselected populations and (other than strontium ranelate) are approved on the PBS for use in older patients. The choice of treatment is based on patient factors, including preference and adherence. Furthermore, as noted above, patients with severe osteoporosis and recurrent fracture despite ART can access anabolic treatment with teriparatide on the PBS.
Monitoring and long-term therapy
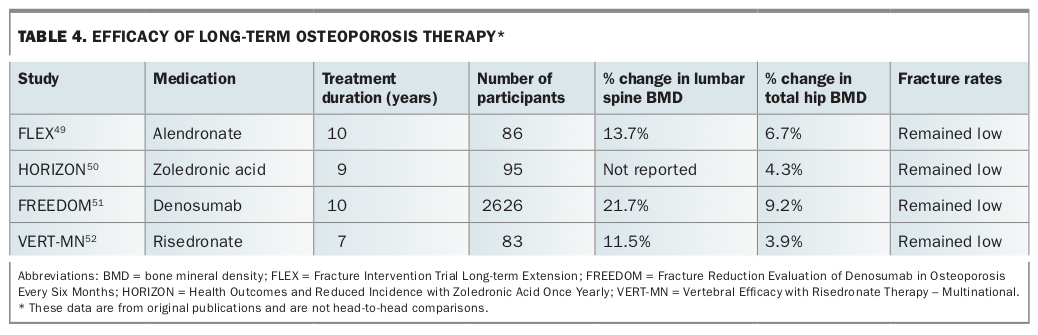
There is relatively little evidence on monitoring and long-term therapy, and decisions may need to be based on clinical judgement and expert advice. Similar to diabetes and hypertension, osteoporosis is a chronic condition without an imminent cure and requires long-term therapy. The RACGP and Osteoporosis Australia guidelines provide useful advice in this regard.3 As a general rule, patients should continue treatment for as long as they remain at risk or cessation would result in a loss of benefit. There is evidence of benefit up to 10 years, with the rate and severity of treatment side effects remaining low, and there is no suggestion of significant adverse effects (Table 4).49-52 Direct treatment comparisons are not possible, as studies have used different patient selection criteria and different study designs and there are no head-to-head comparison studies.
{kind=link}
Bisphosphonate treatment is generally reviewed after three to five years, and the decision to interrupt or continue treatment is based on risk. It is recommended that BMD measurement is repeated after three to five years, to monitor treatment, response and need. Treatment is reviewed if fracture risk reduces to low-risk thresholds (e.g. total hip BMD T-score of –2.5 or higher). In this situation, bisphosphonates may be interrupted, with close monitoring and review every 12 to 24 months (time for the effect of treatment to wear off), and treatment should be reinitiated if required.
With reversible agents, especially denosumab, cessation results in a rapid reduction in BMD and an increase in risk to pretreatment levels. Hence, greater caution is recommended, and treatment should be either continued (if safe to do so) or transitioned to a less readily reversible agent (e.g. bisphosphonates for a period before cessation to blunt the rapid loss of bone).
Long-term and serious complications of treatment
The main concern with potent ART is the risk of hypocalcaemia. This risk can be minimised by optimising calcium and vitamin D status. Extra caution is required in those with renal impairment (estimated glomerular filtration rate less than 30 mL/min), and treatment with ART should be used with caution or avoided in these people, depending on the severity of renal impairment (specialist advice is recommended).
Potential serious long-term complications of bisphosphonate and denosumab treatment are atypical femoral fracture (AFF) and osteonecrosis of the jaw (ONJ).37 Both are extremely uncommon in people receiving osteoporosis treatment, and the benefit of treatment in terms of fracture morbidity and mortality outweighs the risk. However, the risk increases with duration of ART, and patients should be monitored and managed on an individual risk-benefit basis. To put this risk into perspective, the rate of major osteoporotic fracture in women at high risk is 3100 per 100,000 person-years, and bisphosphonates reduce fractures by 20 to 70%.37 The rate of AFF attributed to long-term bisphosphonate therapy at eight years is 78 per 100,000 person-years. Many more osteoporotic fractures would be prevented for each AFF caused by ART.37
The overall risk of ONJ in patients receiving bisphosphonates remains low (between one in 10,000 and less than one in 100,000 patient treatment-years).53 The incidence is higher in patients with cancer, who are often treated with high-dose bisphosphonates.53 Although there have been reports of an increase in incidence of oesophageal cancer in patients taking bisphosphonates, further studies are required.54 However, it is recommended that clinicians should avoid prescribing oral bisphosphonates to people with existing oesophageal disease (e.g. achalasia, Barrett’s oesophagus).54
The American Dental Association recommends that a patient with active dental or periodontal disease should be treated despite the risk of ART-induced ONJ, because the risks and consequences of no treatment likely outweigh the risk of developing ONJ.55 It is important to inform patients taking ART that there is a risk (albeit low, at less than 0.1%) of ONJ before they undergo dental care. Risk can be minimised with good hygiene practices and regular dental care. Discontinuing therapy may not eliminate ONJ risk but may increase fracture risk.
Long-term (more than five years) bisphosphonate use may be associated with higher risk of AFF (100 per 100,000 person-years), but there are few data in this area. Although the relative risk of AFF with bisphosphonate therapy appears, on this evidence, to be high, the absolute risk remains very low, ranging from 3.2 to 50 cases per 100,000 person-years.56 The risk of AFF has been shown to significantly decrease after cessation of bisphosphonates, irrespective of the duration of treatment.57 It is not known if the same is true of ONJ. The European Menopause and Andropause Society suggests that all bisphosphonates should be discontinued after five years. If there is no evidence of high risk (BMD T-score less than –2.5 or fragility fracture on treatment), a drug holiday is recommended for one to two years.58 Fracture risk increases after two years off therapy, so patients should be closely monitored during this time. If fractures occur or BMD decreases (T-score of –2.5 or less), ART should be recommenced.
Case reports and an observational trial have suggested that BMD declines rapidly and vertebral fracture risk increases after discontinuation of long-term denosumab.59-61 Oral alendronate for 12 months after denosumab prevents bone loss in the majority of patients.62 However, the protective effect of prolonged exposure to bisphosphonates before denosumab initiation against vertebral fractures after denosumab discontinuation has not been confirmed. Data from small studies have suggested this, but further studies are required.63
Conclusion
Osteoporosis is undertreated after all fragility fractures, including hip fracture. Hip fractures are a common osteoporotic fracture in older people; they usually require surgical intervention and can have serious consequences. Osteoporosis is a chronic condition that requires timely and ongoing treatment. ART is the current mainstay, and choice of medication depends on patient factors and adherence. Adherence to oral bisphosphonates is often poor because of specific oral dosing requirements, and enteric-coated risedronate, which does not have these requirements, may be the preferred option if oral therapy is chosen. Parenteral treatment can reduce adherence concerns, as long as patients are followed up regularly for dosing, and it can also reduce polypharmacy. Anabolic therapies, such as teriparatide, add value to treatment but must be followed by ART to consolidate and maintain their benefit. Adherence is important to maintain benefit, and cessation or interruption of therapy eventually results in loss of benefit and increased fracture risk. Long-term therapy appears to be safe, with a very low risk of serious adverse effects. Useful resources for GPs and patients are listed in Box 2. MT
{kind=link}