Osteoporosis: a practical update on its management

Osteoporosis is a common chronic musculoskeletal condition affecting many Australians and is associated with significant morbidity and premature mortality. Once patients are recommended for treatment to reduce fracture risk, long-term management and monitoring is recommended. Clinicians can be guided in their management decisions by an understanding of the assessment of bone mineral density scan results, fracture risk estimation and the range of effective available pharmacotherapies and strategies to mitigate potential adverse effects.
- Osteoporosis and fragility fractures are a growing health burden in our ageing population but remain underdiagnosed and undertreated in both men and women.
- Despite advancements in diagnosis and treatment of osteoporosis, there are several barriers to optimising osteoporosis treatment.
- Serial dual-energy x-ray absorptiometry (DXA) bone mineral density (BMD) scans should ideally be performed at the same facility for more accurate comparison.
- Clinicians should be aware of the pitfalls of DXA BMD measurement, including causes for artefactual elevations in BMD.
- Bisphosphonate ‘treatment breaks’ are not recommended for all patients; rather they should be used on a case-by-case basis, depending on ongoing fracture risk.
- Denosumab has a favourable long-term risk-benefit profile; however, cessation results in a ‘rebound phenomenon’ and thus patients should be transitioned to a bisphosphonate.
- Patients commencing on denosumab should be carefully chosen and counselled regarding risks of post-cessation rebound bone loss and fracture risk.
- Long-term safety data on antiresorptive use is overall reassuring for the risk of atypical femoral fracture and osteonecrosis of the jaw, although particular care should be taken with its use in specific populations.
- Osteoanabolic agents (teriparatide, romosozumab) are PBS-reimbursed for patients with severe osteoporosis at very high fracture risk, and short treatment courses should be followed by antiresorptives to consolidate gains in BMD and fracture risk reduction.
Osteoporosis, or osteopenia, is a chronic musculoskeletal disorder characterised by low bone mineral density (BMD) and microarchitectural deterioration, resulting in skeletal fragility and increased risk of fragility/minimal trauma fractures (spontaneous fractures or those resulting from impact equal to or less than a fall from standing height). Osteoporosis is common, affecting up to 6.2 million Australians over the age of 50 years.1 One in three women and one in five men in Australia will experience an osteoporotic fracture. In 2015 and 2016, more than 50,000 people were hospitalised for hip fractures, of which 90% occurred in adults older than 65 years.
Osteoporotic fractures are associated with functional decline, impaired quality of life, institutionalisation and premature mortality.1 Hip fractures are the most devastating consequence of osteoporosis, whereas vertebral fractures are the most common fracture and can either be asymptomatic (detected radiographically) or associated with kyphosis, loss of height, impaired self-esteem and severe pain. Distal radius fractures can also be the first warning sign of osteoporosis. As Australia’s population continues to age, over 180,000 osteoporotic fractures are projected to occur in 2022, costing an estimated $3.84 billion to the healthcare system and society as a whole.1
Once treatment is recommended to reduce a patient’s fracture risk, their condition is ideally managed with a long-term treatment and monitoring plan. This plan should incorporate a nuanced balance between minimising lifetime fracture risk whilst also considering individual drug efficacy and risk-benefit profile, and minimising risk of rare skeletal adverse events, such as atypical femoral fracture (AFF) and osteonecrosis of the jaw (ONJ).
This article aims to provide a practical overview of the diagnosis, assessment, management and monitoring of osteoporosis. Key areas of interest include the use of dual energy x-ray absorptiometry (DXA) bone mineral density (BMD) scans, bisphosphonate ‘treatment breaks’, safety issues surrounding the risks of AFF and ONJ, post-denosumab cessation ‘rebound phenomenon’, and the role of the newer osteoanabolic agent romosozumab in osteoporosis treatment.
Current barriers to effective osteoporosis management
Recent advances in our understanding of bone remodelling have enhanced the therapeutic options available for treating osteoporosis and preventing fractures. These include demonstration of the long-term efficacy and safety of well-established antiresorptive therapies and the recent emergence of the osteoanabolic agent romosozumab. Unfortunately, osteoporosis remains underdiagnosed and undertreated. Many individuals who sustain low impact fragility fractures or incidental vertebral fractures are not investigated further.
Ongoing barriers to adequate population-based treatment of osteoporosis and prevention of fragility fractures contribute to suboptimal treatment initiation and adherence, and include a lack of understanding of osteoporosis and its consequences, excessive patient and clinician fear of rare skeletal adverse events, concerns regarding post-denosumab discontinuation rebound, poor co-ordination between health teams for patients sustaining an initial fracture and issues related to cost and treatment subsidisation. Osteoporosis is a silent disorder until fractures occur. Clinicians and patients are unaware of fractures prevented with treatment at an individual level, which makes it difficult to counsel patients on the benefit of initiating or continuing osteoporosis pharmacotherapy.2 One cost-effective system increasingly used to address the ‘osteoporosis treatment gap’ are fracture liaison services, which identify patients with a recent fragility fracture and deliver a multidisciplinary intervention aimed at optimising education, lifestyle management, assessing fracture risk and considering pharmacotherapy to reduce fracture risk.2,3
Bone biology - a brief overview
Bone is a dynamic organ undergoing continuous remodelling and repair to replace old bone with new bone. After osteoclasts resorb bone, new bone is subsequently laid down by osteoblasts at resorption surfaces. Bone formation occurs in a two-step process: deposition of predominantly collagen-containing osteoid (bone matrix), followed by mineralisation of osteoid with calcium and phosphate. Osteocytes have a key role in bone physiology, facilitating skeletal responses to loading or exercise by acting as ‘mechanosensors’ and regulating the release of molecules such as sclerostin, an inhibitor of bone formation.
Diagnosis and monitoring of osteoporosis using DXA
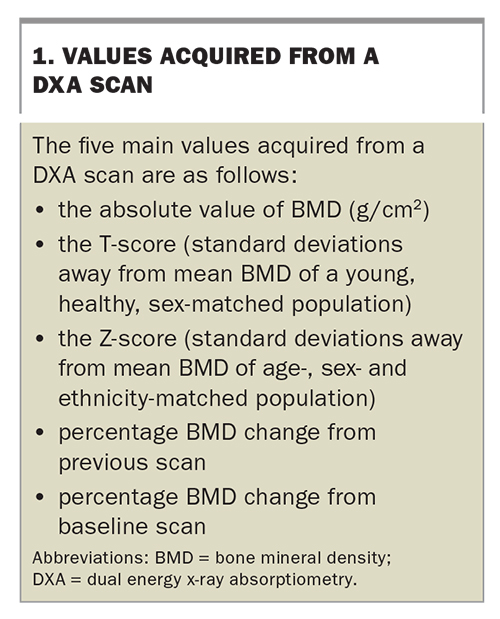
DXA BMD scans are valuable tools in diagnosing osteoporosis, refining assessment of fracture risk, monitoring therapeutic effect and informing treatment decisions.4 Advantages of DXA include low radiation, wide availability and extensive data supporting BMD as a surrogate marker for fracture risk.5 The main disadvantage of DXA is that BMD is only one of several important risk factors for fragility fracture, reflected by the low sensitivity for detecting patients who will experience a fracture when using a T-score cut-off of less than or equal to –2.5 to recommend treatment. Although lower T-scores are associated with higher risk of fracture, most fractures at a population level occur in people with BMD T-scores above –2.5 (the ‘osteoporosis prevention paradox’).2 The five main values acquired from a DXA scan at any skeletal site are listed in Box 1.
{kind=link}
Patients commencing osteoporosis pharmacotherapy may have a progress DXA scan at 12 to 24 months to assess initial response to treatment, and then serial DXA scans at two- to three-yearly intervals, unless an earlier scan is clinically indicated, such as if the patient experiences a fracture on treatment (as the BMD result may qualify patients for governmentfunded osteoanabolic therapy). Serial DXA BMD scans should preferably be performed on the same densitometry system (e.g. GE Lunar, Hologic, etc.) at the same facility to allow more accurate comparison with previous scans. Differences in BMD between DXA machine manufacturers is clinically important and cannot be directly compared. Although a calculator is available to allow conversion between BMD results using different scanners (https://courses.washington.edu/bonephys/opBMDs.html), the average error is about 3.5% and thus, ideally, all serial BMD scans should be performed on the same machine for each patient.
When monitoring treatment effect, only changes greater than the ‘least significant change’ may be considered clinically significant. The least significant change, included in the DXA BMD report, is the minimum change to be 95% confident that the measured change is real and not due to error. Longitudinal comparisons of BMD (percentage change) should be made between absolute BMD values (g/cm2) rather than changes in T-scores or Z-scores.
In the event of an unexpected change in BMD, it is useful to review the DXA images for consistent positioning of the patient compared with previous scans. If in doubt, contact the service provider before making treatment decisions based on the BMD result. Lumbar spine BMD can be artefactually elevated in the setting of degenerative changes of osteoarthritis (such as osteophytic changes) or vertebral fracture. Some centres may include lumbar spine trabecular bone score, which provides information about trabecular microarchitecture, is not affected by degenerative changes and can be incorporated into the University of Sheffield Fracture Risk Assessment Tool (FRAX) to refine fracture risk estimates.4 Femoral neck and total hip BMD are rarely affected by degenerative changes of osteoarthritis; however, surgical hip fixation or hip replacement would render the hip DXA impractical for monitoring.
During follow up of patients with osteoporosis or high fracture risk, frequency and risk factors for falls should be evaluated, given that more than 90% of fragility fractures occur secondary to falls.1 Patients should be routinely assessed for features suggestive of a new vertebral fracture, such as mid-lower midline back pain, midline spinal tenderness, worsening thoracic kyphosis or interval height loss of 2 cm or more. If there are any concerns regarding new vertebral fracture, a thoracolumbar spine x-ray (anteroposterior and lateral views) should be obtained. If the x-ray does not suggest a fracture and clinical suspicion remains high, the patient may be suitable for further imaging, such as CT (detects past fractures), MRI or a technetium whole-body bone scan (detects recent fractures).
Patients with osteoporosis or high fracture risk should have their electrolytes (including corrected calcium), renal function and vitamin D levels monitored annually, and more frequently if any hypocalcaemia or vitamin D deficiency is identified. Vitamin D levels should be maintained at above 50 nmol/L during treatment to reduce the risk of hypocalcaemia from antiresorptive therapies.
When deciding which patients to start on antiresorptive therapy, it is important to note that PBS subsidisation criteria based on DXA BMD T-scores should not be considered as a threshold to recommend treatment as this runs the risk of withholding treatment from patients who may benefit from but don’t quite meet criteria for government-subsidised treatment (Table 1). For example, a 65-year-old postmenopausal woman with lumbar spine BMD T-score –4.0 and femoral neck T-score –3.0 with no history of fragility fracture would not qualify for PBS-funded antiresorptives because her age is less than 70 years; however, she likely has a considerably high fracture risk warranting treatment for fracture risk reduction. In such cases, the option of self-funding treatment may be discussed with the patient.
{kind=link}
Osteoporosis risk factors and secondary screen
The most common risk factor for osteoporosis is menopause, given that oestrogen withdrawal is associated with increased bone turnover and progressive BMD loss by 1 to 4% per year. Androgen deficiency in men can lead to a similar degree of bone loss. When diagnosing and managing patients with osteoporosis, lifestyle risk factors should be optimised, including cigarette smoking, excess alcohol consumption, low physical activity levels, low body weight, anorexia and vitamin D deficiency. The role of exercise as a therapeutic option in osteoporosis management and evidence for antifracture efficacy is not well-established. High-intensity, resistance and weight-bearing or impact exercises have the most robust evidence basis for improving BMD, particularly at the lumbar spine, and may provide other meaningful benefits including improvements in markers of overall physical function and balance.6,7
Exposure to certain medications can also contribute to fracture risk, including chronic glucocorticoid use, antiepileptics, androgen deprivation therapy for prostate cancer and antioestrogen therapy (aromatase inhibitors) for breast cancer. It is reasonable to screen all patients diagnosed with osteoporosis for more common secondary causes, including medication history, vitamin D deficiency, renal impairment, primary hyperparathyroidism (calcium, magnesium, phosphate and intact parathyroid hormone levels) and thyrotoxicosis (thyroid stimulating hormone and free T4 levels). Other investigations may be warranted in certain cases, such as for coeliac disease (total IgA, anti-tissue transglutaminase IgA and antideamidated gliadin peptide IgG levels) and myeloma (serum free light chain, serum electrophoresis and immunofixation). Treating the secondary cause may have a positive effect on BMD and antiosteoporotic treatments alone may not be as effective unless the secondary cause is appropriately treated. Some patients warrant a more extensive secondary screen, including premenopausal women, men aged less than 50 years and patients with a prevalent fracture history. Falls risk reduction strategies may also be useful.1,8
Fracture risk calculators
The FRAX tool provides an estimated 10-year risk of major osteoporotic (spine, hip, forearm, shoulder) and hip fracture (www.sheffield.ac.uk/FRAX/tool.aspx). When using FRAX, ensure the correct country is selected under the drop-down menu ‘calculation tool’ and that the correct BMD machine is used (e.g. Hologic or GE Lunar, etc). FRAX incorporates various clinical risk factors for fracture, listed in Box 2.
Limitations of the FRAX calculator include lack of inclusion of falls history and underestimation for various reasons, including disproportionately low spinal BMD compared with femoral neck BMD and a history of multiple and recent fractures.
The Garvan fracture risk calculator includes number of falls (in the past 12 months) and number of fragility fractures since the age of 50 years and provides an estimated five- and 10-year risk for hip fracture and any osteoporotic/fragility fracture. The Garvan calculator has been validated for use in Australian men and women (www.garvan.org.au/promotions/bone-fracture-risk/calculator/).
Pharmacotherapeutic options for managing osteoporosis
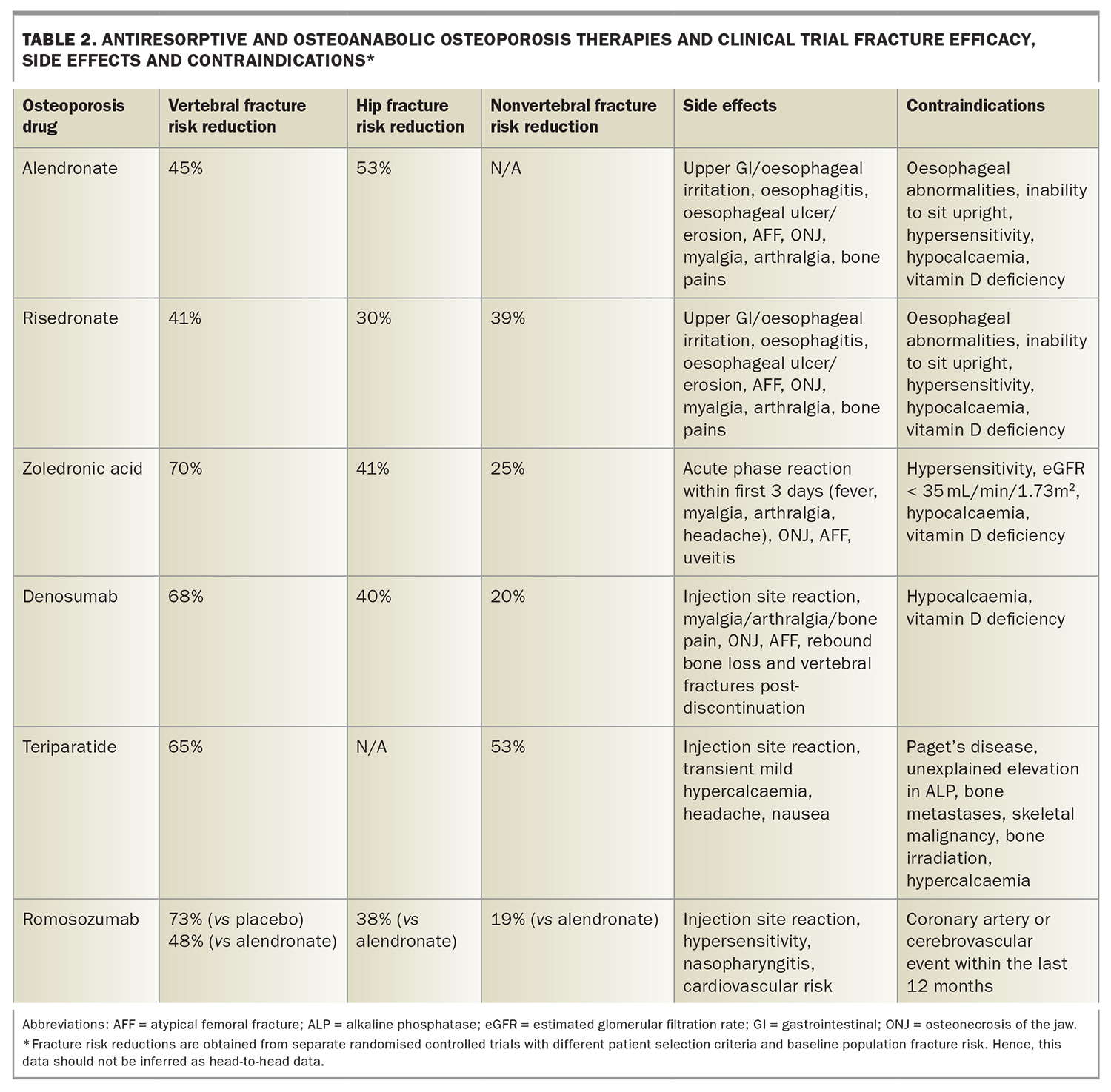
Pharmacotherapy for osteoporosis can be divided into two categories: antiresorptive and osteoanabolic therapy. Antiresorptive therapies (bisphosphonates and subcutaneous denosumab) act to reduce bone resorption, allowing rebalancing of bone remodelling to improve BMD and reduce fracture risk. Bisphosphonates (oral, e.g. alendronate and risedronate, and intravenous zoledronic acid) and denosumab have proven antifracture efficacy for vertebral, nonvertebral and hip fractures in large placebo-controlled randomised controlled trials (RCTs) in postmenopausal women with osteoporosis, and have demonstrated overwhelmingly favourable risk-benefit profiles for risk of osteoporotic fractures compared with skeletal adverse events (Table 2). However, bisphosphonates and denosumab have different mechanisms of action and pharmacokinetic properties and therefore have different recommended prescribing practices and counselling for patients commencing these treatments.9
{kind=link}
Bisphosphonates
Bisphosphonates are preferentially taken up by skeletal sites of increased remodelling, slowly eliminated from bone and suppress bone resorption by inhibiting post-translational modification of proteins essential for osteoclast function and survival.9 The major placebo-controlled trial for alendronate in women with osteoporosis found a 45% reduction in vertebral fractures, 53% reduction in hip fractures and 30% reduction in all clinical fractures.10 Placebo-controlled RCTs for risedronate in postmenopausal osteoporosis showed a reduction in vertebral fractures by 41%, hip fractures by 30% and nonvertebral fractures by 39% over three years.11,12 Annual treatment with zoledronic acid over three years has been associated with a 70% reduction in vertebral fractures, 41% reduction in hip fractures, 25% reduction in nonvertebral fractures and 33% reduction in clinical fractures compared with placebo (Table 2).13
Bisphosphonate treatment breaks
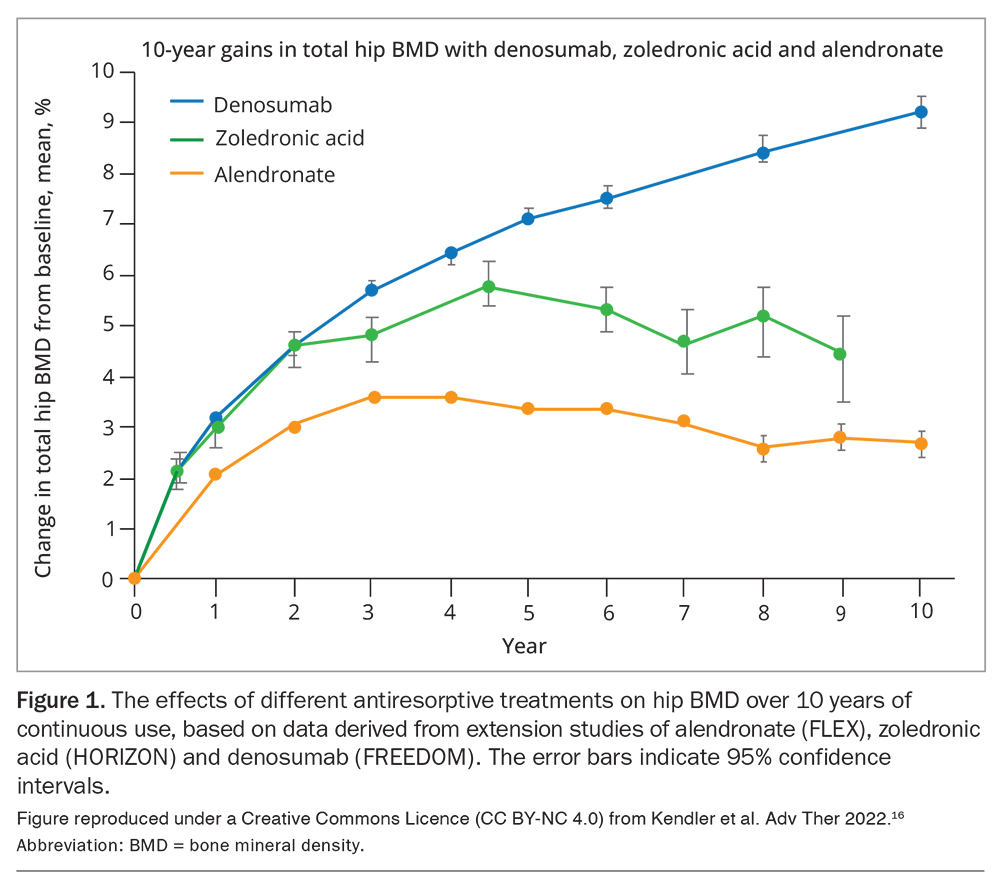
Bisphosphonate ‘treatment breaks’ are used to optimise the risk-benefit profile of medium- to long-term management. Bisphosphonate use is associated with a plateau in BMD gains and antifracture efficacy, and has slow offset of effect, particularly with zoledronic acid (Figure 1). The risk of AFF is associated with increased duration of therapy, particularly beyond eight years of continuous use, and dramatically declines after stopping bisphosphonates.8,14,15
{kind=link}
However, a treatment break should not necessarily be given to all patients taking bisphosphonates. Patients should have their fracture risk reassessed at three to five years for an individualised shared decision to be made about whether to continue treatment, based on BMD T-scores achieved at lumbar spine and hip, history of fracture since starting treatment, recent hip or clinical/multiple vertebral fractures and patient preference. For example, a treatment break may be appropriate for a patient with a lowest T-score of –2.0 after three to five years of taking bisphosphonates without any new fractures, whereas it may not be appropriate for a patient with a lowest T-score of –3.0 after treatment and a recent symptomatic vertebral fracture. Based on a recent placebo-controlled RCT, 18-monthly zoledronic acid infusions over a six-year period were shown to reduce fragility fractures by 37% in postmenopausal, predominantly osteopenic women. Therefore, patients on zoledronic acid who still require ongoing treatment after three to five years may be suitable for continuation of therapy with reduced frequency of infusions to 18-monthly. However, whether this approach reduces the risk of AFFs is unclear.16
Denosumab
Denosumab is a fully human monoclonal antibody against receptor activator of nuclear factor-kappaB ligand (RANKL), inhibiting osteoclast differentiation, function and survival.9 Based on recent data from the extension of the FREEDOM placebo-controlled study, denosumab has shown favourable efficacy and safety for up to 10 years continuous treatment, with continued increases in BMD and persistently low rates of osteoporotic fracture, AFF and ONJ. Denosumab use was associated with sustained increase in BMD of 21.7% at lumbar spine and 9% at femoral neck (Figure 1). Two cases of AFF occurred (at three and seven years of exposure), with an incidence of 0.8 per 10,000 patient years, and 13 cases of ONJ occurred, of which 11 were mild to moderate, with incidence of 5.2 per 10,000 patient years. The skeletal risk-benefit profile with 10 years of denosumab therapy was positive, with 281 and 40 clinical fractures prevented for each case of AFF and ONJ, respectively.17,18 In contrast to denosumab use, the effect of bisphosphonates on BMD plateaus at three to five years (Figure 1).18
Denosumab post-discontinuation rebound phenomenon
Unlike bisphosphonates, treatment breaks are not recommended for patients receiving denosumab for osteoporosis. Reasons for this include the continuous BMD gains and persistent fracture risk reduction with long-term therapy and, most importantly, the rapid offset and reversal of BMD gains after stopping denosumab after at least two doses.18
This ‘rebound phenomenon’ is characterised by rapidly rising bone resorption marker levels peaking at twelve months after the last injection, with profound loss of BMD gains within 12 to 24 months after the last dose, and, in some cases, multiple vertebral fractures.15
The pathophysiology of post-denosumab rebound is not yet fully elucidated. Risk factors for vertebral fractures after stopping denosumab include previous history of multiple vertebral fractures, longer duration off treatment, greater hip BMD gain during treatment and greater loss of hip BMD after discontinuation. The duration of denosumab treatment may influence the rate and amount of BMD loss; however, the association with vertebral fracture risk is conflicting.19,20
Denosumab discontinuation and counselling before initiation
Denosumab discontinuation may be performed in certain settings, such as when a patient prefers to stop antiresorptive therapy, in patients who are intolerant to denosumab, or if the patient has low fracture risk and does not require long-term antiresorptives. Transitioning to a bisphosphonate for one to two years is recommended when stopping denosumab (unless denosumab is stopped because of a skeletal adverse event, e.g. AFF) to try to reduce the risk of rapid loss of BMD gains and multiple vertebral fractures.18 The choice, dose and timing of bisphosphonates to mitigate denosumab rebound is largely unknown; however, based on most recent evidence and a position statement by the European Calcified Tissue Society, it is prudent to start an oral or intravenous bisphosphonate six months after the last injection (i.e. when the next denosumab dose is due). Intravenous zoledronic acid is preferred for more high-risk patients, such as those with longer duration of denosumab treatment (more than 2.5 years) or greater BMD gain on denosumab. For patients requiring elective dental procedures, denosumab should ideally be continued, although it may be prudent to perform the procedure at four to five months after the last denosumab dose.
Careful consideration should be taken in choosing appropriate patients for denosumab initiation, based on age, fracture risk and likelihood of needing long-term antiresorptives. All patients commencing denosumab should be counselled about the risk of post-cessation rebound, which does not appear to be completely attenuated by transitioning to bisphosphonates, and that commencement of denosumab is generally with a view towards long-term antiresorptive treatment. For example, denosumab may not be suitable for a 60-year-old woman without any fractures and a lowest T-score of –3.0; whereas, it may be very suitable for an 80-year-old woman with a vertebral or hip fracture and a lowest T-score of –4.0.
Hormone-based therapies
Menopausal hormone therapy (MHT)
MHT (oestrogen alone or combined oestrogen and progesterone if uterus intact) is indicated for postmenopausal symptoms (e.g. hot flushes) and is a reasonable treatment option for osteoporosis in women who have undergone menopause in the past 10 years with a low baseline risk of venous thromboembolism (VTE), coronary artery disease, stroke and breast cancer. In the Women's Health Initiative (WHI) placebo-controlled trials, MHT significantly reduced the risk of any clinical fracture by 28%, major osteoporotic fracture by 40% and hip fracture by 34%, over a mean 4.3 years. Systematic review evidence suggests a modestly increased risk of coronary artery events, stroke, VTE and breast cancer with combined MHT; however, oestrogen-only MHT is associated with a modestly increased risk of VTE and a reduced risk of breast cancer, with no impact on risk of coronary artery events. Based on subgroup analyses of WHI data, a more favourable risk-benefit profile was found for women aged 50 to 59 years.8,21,22 Transitioning to alternative osteoporosis therapy may be advised after MHT given that the positive gains in BMD seen with MHT are lost within 12 to 24 months after stopping therapy.
Raloxifene
Raloxifene is a selective estrogen receptor modulator (SERM), which mimics oestrogen action in bone and has antioestrogenic actions in breast tissue, with no effect of endometrial stimulation.23 Raloxifene is TGA-indicated as a treatment option for postmenopausal osteoporosis and has been shown to reduce vertebral fracture risk by 30% over three years compared with placebo, with no significant reduction in nonvertebral fracture risk.23 There is a 70% lower incidence of breast cancer and a 3.1-fold higher risk of VTE (comparable to increased VTE risk with MHT), although with low incidence rates (1% vs 0.3%).24Adverse events included hot flushes (9.7% vs 6.4% with placebo), which were mostly mild to moderate and occurred in the first six months of use, and leg cramps (6.9% vs 3.7% with placebo). A one-year extension study indicated persisting vertebral fracture risk reduction and no new safety concerns.25 Raloxifene use may therefore be appealing to postmenopausal women with osteoporosis without vasomotor menopausal symptoms who are particularly at risk of vertebral fracture and have low VTE risk.
Tibolone
The metabolites of tibolone have variable oestrogenic effects on various tissues. Tibolone is TGA-indicated for use to minimise vasomotor menopausal symptoms and as a second-line treatment for postmenopausal osteoporosis. Tibolone has proven antifracture efficacy, based on results from a placebo-controlled study that showed a 45% reduction in vertebral fractures, 26% reduction in nonvertebral fractures and 46% reduction in wrist fractures.26 There was a 68% reduced risk of invasive breast cancer with no safety signals for coronary artery disease or VTE with tibolone treatment. However, an increased risk of stroke (RR 2.19, 1.1% vs 0.5%) resulted in premature termination of the study.27 Therefore, tibolone may be used as a second-line treatment for postmenopausal osteoporosis, and should be avoided in patients who are at high risk of stroke or have a previous history of stroke.
Safety of antiresorptive therapy
Transient hypocalcaemia can occur uncommonly in patients receiving denosumab and bisphosphonates; risk factors include pre-existing hypocalcaemia, vitamin D deficiency and renal impairment (estimated glomerular filtration rate less than 30 mL/min/1.73 m2). Clinicians should ensure patients are vitamin D replete (with levels greater than 50 nmol/L) when therapy is started, with reassessment of vitamin D levels based on clinical judgement.
Patients taking oral bisphosphonates (alendronate, risedronate) may experience reflux or upper gastrointestinal discomfort and should be advised to avoid eating or lying flat for at least 30 minutes after administration (avoiding food before administration also improves absorption). Patients should not be started on alendronate or risedronate if they are unable to sit upright or if they have existing oesophageal disorders (e.g. achalasia, stricture). An enteric coated formulation of risedronate is now available to minimise gastrointestinal irritation and may be taken with a light breakfast. Myalgias, arthralgias and bone pain can also occur uncommonly in those taking oral bisphosphonates and denosumab.
Patients started on intravenous zoledronic acid must be counselled about the potential risk of an ‘acute phase reaction’, usually characterised by one to two days of myalgia, arthralgia and lethargy with or without fever, with symptom onset the day after the infusion. This reaction is rarely severe; however, it can be alarming for patients who are not appropriately counselled, particularly given the COVID-19 pandemic. Patients should be advised to keep well hydrated and, if no contraindications, paracetamol (1000 mg up to four times per day as required) can be recommended to alleviate pain and fever and has been shown to reduce the risk of an acute phase reaction by 50%. Patients who are particularly concerned or with a history of a severe acute phase reaction may be offered a two-to-three-day course of oral prednisolone on a case-by-case basis.
Uveitis is a very rare side effect associated with intravenous zoledronic acid use and patients should be advised to see an ophthalmologist urgently if they develop redness in the eye, particularly if any associated concerns of blurred vision or eye pain.
Atypical femoral fractures
In 2005, the first cases of atypical femoral diaphyseal/shaft fractures (AFFs) were reported in patients with osteoporosis taking bisphosphonates. Longitudinal studies have since shown overwhelming favourable risk-benefit profiles on the risks of osteoporotic fractures compared with skeletal adverse events. For every case of AFF associated with three years of bisphosphonate treatment, an estimated 1,200 fractures, including 130 hip fractures, are prevented. Despite this, substantial concerns among patients and clinicians persist regarding long-term skeletal safety of antiresorptive treatments.8,28
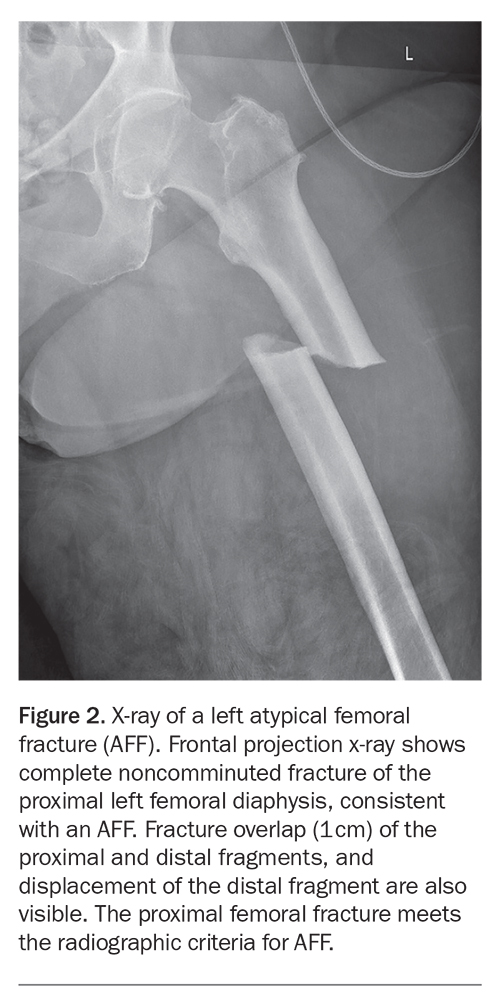
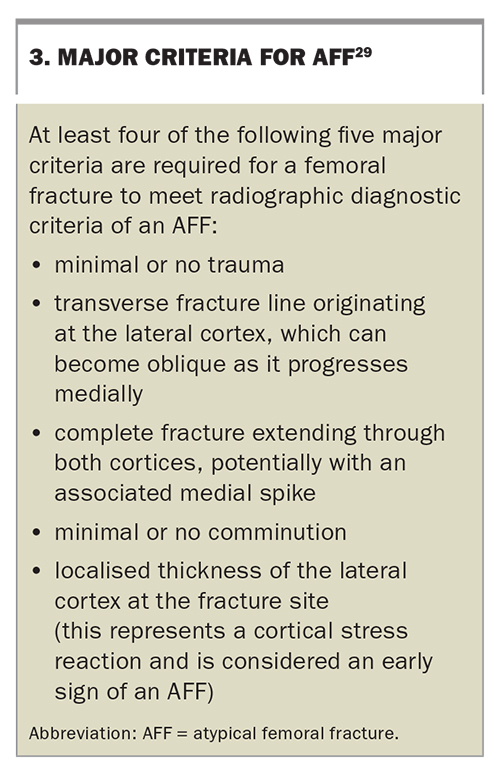
According to the revised definition by the American Society for Bone and Mineral Research Task Force in 2014, AFFs must be located along the femoral shaft (Figure 2). The five major criteria for AFF, of which four are required, are shown in Box 3.
{kind=link}
{kind=link}
Risk factors for AFF include bisphosphonate or denosumab use and longer duration of exposure, Asian ethnicity and concurrent glucocorticoid exposure. The age-adjusted incidence rate for AFF with bisphosphonate use is 1.8 per 100,000 person-years with less than two years of exposure, compared with 113 per 100,000 person-years with eight to 10 years of exposure. The underlying pathogenesis is unclear; however, the current consensus is that bisphosphonates suppress targeted osteoclastic bone resorption, resulting in a culmination of unrepaired micro-cracks into stress-like fractures.28,30
An important 10-year study of 196,129 women receiving bisphosphonates (98% oral) found 277 episodes of AFF. The study confirmed that a longer duration of bisphosphonate exposure increases the risk of AFF, particularly continuous exposure of more than eight years, and found a four- to fivefold higher risk in Asian participants compared with Caucasians. There were two major reassuring findings from this study: the absolute risk of AFF was very low and a far greater number of fragility fractures were prevented for every case of AFF (at five-years of bisphosphonate exposure, 286 hip and 859 clinical fractures were prevented for every eight AFFs); and AFF risk rapidly declined early after bisphosphonate discontinuation and continued to fall over time (4.5 per 10,000 person years among current users, compared with 0.5 per 10,000 person years at more than 15 months since discontinuation).31
All patients starting antiresorptives for osteoporosis should be counselled, and largely reassured, about the risk of AFF. Patients should be educated on the potential symptoms of AFF, including persistent anterior thigh or groin pain, and be advised to seek medical consultation if these symptoms persist. Patients with suspected AFF should undergo a bilateral femoral x-ray as it is not uncommon for patients with AFF to have signs of an early stress fracture on the contralateral femur, even if asymptomatic on that side. Patients with an AFF and asymptomatic patients with early signs of an AFF (e.g. cortical beaking with or without lucency) should be considered for prophylactic surgical fixation. If symptoms are persisting and there is no evidence of AFF on an x-ray, further imaging may be warranted, such as CT, MRI or bone scan.
Decisions about ongoing management of osteoporosis after an AFF are complex and require assessment of the risk of a contralateral AFF with continued treatment compared with the risk of a fragility fracture if treatment is stopped. Such patients should be referred to a clinician specialising in the management of osteoporosis.
Osteonecrosis of the jaw
ONJ is a clinical diagnosis defined as exposed bone in the maxillofacial region for more than eight weeks, in absence of local radiotherapy. Radiographic and histopathological findings are supportive but not required for diagnosis.17,32-35 ONJ is an uncommon skeletal complication of long-term bisphosphonate and denosumab use in osteoporosis and is more commonly seen in patients taking much higher doses for skeletal metastases. ONJ incidence is less than 1 in 10,000 person-years in patients using bisphosphonates for osteoporosis.8 The underlying pathogenesis is not well defined; however, ONJ has been associated with periodontal surgery or infection and poor dental hygiene in individuals with antiresorptive-induced suppression of bone resorption and angiogenesis (and thus impaired remodelling and wound healing).4,5 Risk factors for ONJ include malignancy, intravenous bisphosphonate use, longer duration of antiresorptive exposure, recent invasive dental procedure (e.g. extraction or implantation, not root canals or routine cleaning), tobacco use, excessive alcohol consumption and glucocorticoid use.
Patients should be counselled to maintain good oral hygiene and have regular annual dental reviews while taking antiresorptives. If a patient has not had a dental review for two or more years at the time of starting antiresorptive therapy, and if there are concerns regarding dental hygiene, this may be recommended first to ensure any required dental surgeries can be undertaken promptly before starting antiresorptive therapy. Meticulous detail to dental surgery, antiseptic mouth rinses and antibiotics may reduce the risk of ONJ associated with dental procedures.
Osteoanabolic agents
The two available osteoanabolic agents for osteoporosis treatment in Australia include romosozumab and teriparatide. Patients being managed with short courses of osteoanabolic therapy (up to 12 months for romosozumab and up to 24 months for teriparatide) need to be managed by an osteoporosis specialist and, hence, the GP’s role in this setting is knowing who to refer for potential commencement of osteoanabolic therapy and to be aware of safety concerns patients may have.
Teriparatide
Teriparatide is administered as a subcutaneous 20 mcg daily injection. Teriparatide is a recombinant form of the first 34 amino acids of parathyroid hormone (PTH 1-34), which harbours most of PTH’s biological activity. Teriparatide demonstrates potent anabolic effects, inducing increased remodelling rates with a net increase in bone formation.36 It has been shown to reduce vertebral fractures by 65% and nonvertebral fractures by 53% over a 21-month period based on placebo-controlled trial data (Table 2).37 Teriparatide was well tolerated; mild hypercalcaemia occurred more frequently with teriparatide in the first four to six hours after the dose (11% vs 2%) and headache and nausea occurred in 8% of participants but at similar rates to placebo. Concerns regarding osteosarcoma were raised based on carcinogenicity studies in rats; however, this was at higher relative doses and administration across their entire lifespan.36 Based on a 15-year postmarketing surveillance study conducted in the US, there is no apparent increased risk of osteosarcoma associated with teriparatide use in humans.38
Teriparatide is PBS-reimbursed for patients with severe osteoporosis (T-score less than or equal to –3.0) who have at least two osteoporotic fractures, including at least one occurring despite 12 months of continuous antiresorptive therapy (Table 1). Although PBS reimbursement only covers 18 months of treatment, teriparatide is TGA-approved for a total of 24 months (i.e. if a further six months is sought, this would not be PBS-reimbursed). Given the theoretical risk of osteosarcoma, teriparatide is contraindicated in patients with an unexplained elevation of alkaline phosphatase, Paget’s disease, or prior bone irradiation because these are risk factors for osteosarcoma in the general population.
Romosozumab
Romosozumab is a monoclonal antibody against sclerostin, and acts to increase bone formation and reduce bone resorption.40 Romosozumab is well-tolerated and has been shown to increase lumbar spine and hip BMD at greater magnitudes than other available treatments (11% and 4% at 12 months, respectively) and has substantial antifracture efficacy.39,40 In the FRAME placebo-controlled trial, 12-months of romosozumab reduced the risk of vertebral fractures by 73% and clinical fractures by 36%.40 The ARCH trial comparing romosozumab with alendronate showed a 48% reduction in vertebral fractures, 38% reduction in hip fractures and 19% reduction in nonvertebral fractures with romosozumab (Table 2).41
Romosozumab is currently PBS-reimbursed in Australia for patients considered to be at very high fracture risk (i.e. patients with BMD T-scores less than or equal to –3.0 who have fractured despite continuous antiresorptive use). The recommended dose is 210 mg monthly subcutaneous injection (two doses of 105 mg) for 12 months.
The main side effects of romosozumab include nasopharyngitis (12%), arthralgia (12%) and injection site reactions (3%); however, hypocalcaemia, AFF and ONJ are exceedingly rare. There was an increased signal for serious cardiovascular events, including coronary artery disease and cerebrovascular disease from the ARCH trial comparing romosozumab (2.5%) with alendronate (1.9%); whereas, no increased risk was found in the FRAME trial comparing romosozumab with placebo.41 The clinical significance of this result is currently unclear. However, it is recommended to avoid romosozumab in patients with a history of a coronary artery or cerebrovascular event within the last 12 months. It may also be suitable to screen for and modify reversible risk factors for cardiovascular disease, including smoking, hypertension and hypercholesterolaemia, when starting a patient on romosozumab.
Osteoanabolic therapy should be followed by antiresorptive therapy to consolidate BMD gains and preserve fracture risk reduction, based on results of treatment sequence trials in which teriparatide and romosozumab were followed by placebo or antiresorptives.42,43
Conclusion
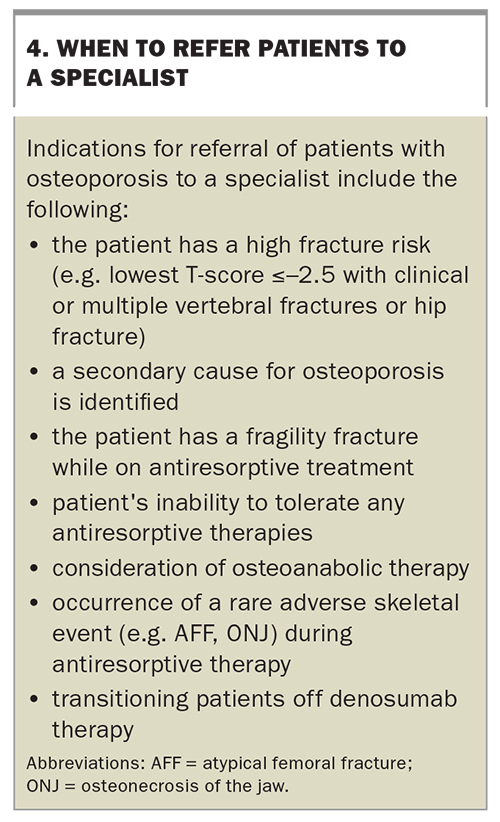
Osteoporosis is a chronic musculoskeletal condition and, once patients are recommended for pharmacotherapy to reduce fracture risk, management and monitoring across the remaining lifespan should be considered. GPs play an important role in the diagnosis and management of osteoporosis in the community, and in encouraging long-term patient adherence with therapies. To improve diagnosis and management of people with osteoporosis and elevated fracture risk in primary care, a greater understanding of the consequences of undertreating osteoporosis and fragility fracture risk, appropriate interpretation of DXA BMD scan results and methods for fracture risk assessment are needed. Additionally, clinicians should be aware of the wide array of pharmacotherapeutic options available for fracture risk reduction, including nuances in treatment efficacy and risks, particularly surrounding bisphosphonate ‘treatment breaks’, post-denosumab ‘rebound phenomenon’ and AFF and ONJ, which are associated with antiresorptive use. Osteoanabolic agents, such as romosozumab and teriparatide, are initiated by specialists experienced with management of osteoporosis; primary care physicians should have a good understanding of which patients may be suitable for referral for consideration of osteoanabolic therapy, as well as other reasons to refer patients in the community for specialist review. Practice points on when to refer patients to a specialist are summarised in Box 4. MT
{kind=link}
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.