Schizophrenia: the GP’s crucial management role

Schizophrenia
Psychotic disorders
Schizophrenia and related psychoses are conservatively estimated to affect more than 100,000 Australians, as well as their families, friends and colleagues. People with schizophrenia are more likely to experience health morbidity and to die prematurely, by up to 25 years, from suicide or physical illness. GPs are in an ideal position to detect and treat schizophrenia and related psychoses and to monitor and manage the physical health of patients with psychotic illnesses.
- Early recognition and referral are key in managing schizophrenia and related psychoses.
- Management should occur within a framework of autonomy and self-determination and, where possible, with family or carer inclusion.
- Pharmacological and psychosocial treatments improve outcomes, including quality of life, for people affected by schizophrenia.
- Antipsychotic, mood stabiliser and antidepressant medications may all be indicated in treating psychoses.
- Several new atypical and depot antipsychotic medications (oral brexpiprazole and depot aripiprazole and paliperidone) are available on the PBS.
- When risk is high or escalating, safety is paramount and urgent referral should be considered.
- Monitoring and managing the long-term physical health of people with schizophrenia is crucial to reducing morbidity and mortality.
- GPs have a key role in recognising substance misuse and supporting behavioural change.
Schizophrenia is a chronic mental health disorder that is conservatively estimated to affect more than 100,000 Australians, or 0.5% of the Australian population, in their lifetime and is often managed in general practice.1 It is characterised by the persistent or intermittent presence of a pattern of psychotic experiences, such as delusional ideas, perceptual abnormalities and thought disorder, as well as dysregulation of mood and cognition.2 Schizophrenia is thought to be a heterogeneous group of disorders with complex and incompletely elucidated underlying mechanisms.3 It is therefore best considered in association with its related spectrum of illnesses, including schizoaffective disorder and other affective psychoses.4 For practical purposes, this article encompasses schizophrenia, schizoaffective disorder and related psychoses and refers to schizophrenia and psychoses interchangeably.
The prognosis of schizophrenia is variable but is usually established during the first five years of illness. Although antipsychotic medication has improved outcomes considerably, 50 to 60% of patients continue to experience relapsing and chronic psychotic symptoms, whereas about 30% have persistent social and occupational functional deficits, particularly because onset often occurs during the formative adolescent and early adult years.5 Complications are common in those with psychotic disorders, with lifetime prevalences of 35% for suicide attempts, 74% for substance misuse, 5% for homelessness and 49 to 68% for commission of violent acts.4
Physical health disorders are often comorbid, and the life expectancy of people with schizophrenia is as much as 25 years lower than that of the general population.6 About 80% of this excess mortality is attributable to physical illness.7
GPs are often the first point of contact for people with psychoses, as well as providing care for their physical health (Box 1 and Table 1 and Table 2). Where people are not able or willing to access specialist psychiatric services, many GPs provide specialist-level care. This is particularly true in rural and remote areas, as well as for people with poor insight into their illness and a reluctance to receive treatment. The episodic care practised by stretched mental health services may also increasingly see patients discharged to GP care; hopefully, but not always, when a stable phase of illness has been reached. In Australia, the role of the GP in relation to early detection, engagement in treatment, physical health monitoring and long-term follow up remains crucial for people with schizophrenia. GPs may also play a primary role in the care of itinerant or elderly people with psychosis in hostels or aged care facilities.
{kind=link}
{kind=link}
{kind=link}
Recognition of psychoses
The onset of schizophrenia may be preceded by a protracted prodrome. The prodrome is characterised by months to years of apathy, social withdrawal and deterioration of function, which may be difficult to recognise.
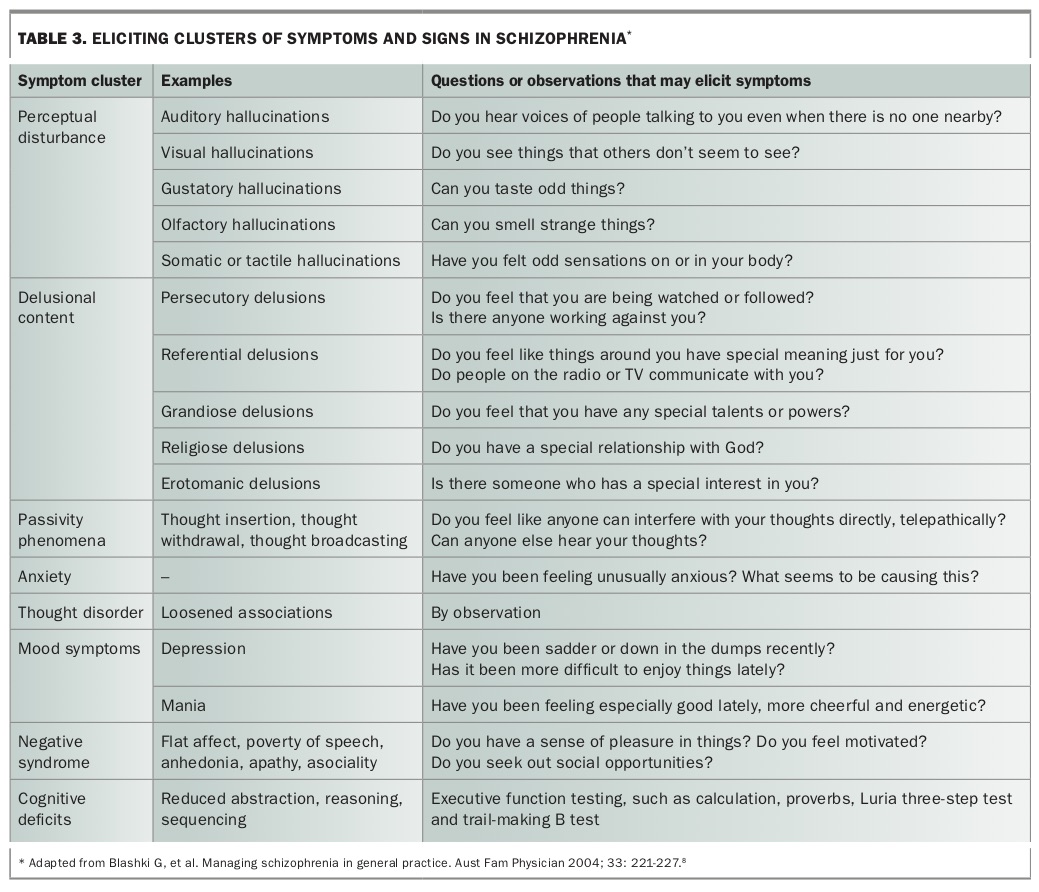
In contrast, acute psychosis (whether the first episode or a psychotic relapse) is often more recognisably manifest by auditory hallucinations, persecutory ideation, referential delusions and passivity phenomena, as well as anxiety and major mood abnormalities. Other abnormalities of perception, possession and thought can occur. Thought disorder and abnormalities of affect modulation are also frequent and may range in severity. In some patients, acute psychosis may be associated with negative syndrome manifestations and cognitive deficits, which tend to be chronic and persistent. Questions to ask the patient to assist with diagnosis are listed in Table 3.8
{kind=link}
Concerned family members may be the first to detect mental state disturbances and report these to the GP. The patient’s family is also a rich source of collateral history. Neither the family nor the patient may recognise the problem as psychosis, especially if more well-known symptoms, such as hallucinatory voices, are not present. Although health literacy regarding mental health disorders is increasing, recognition and understanding of appropriate treatment of psychosis remain poor in the community, highlighting the need for detection and psychoeducation in healthcare settings.9,10
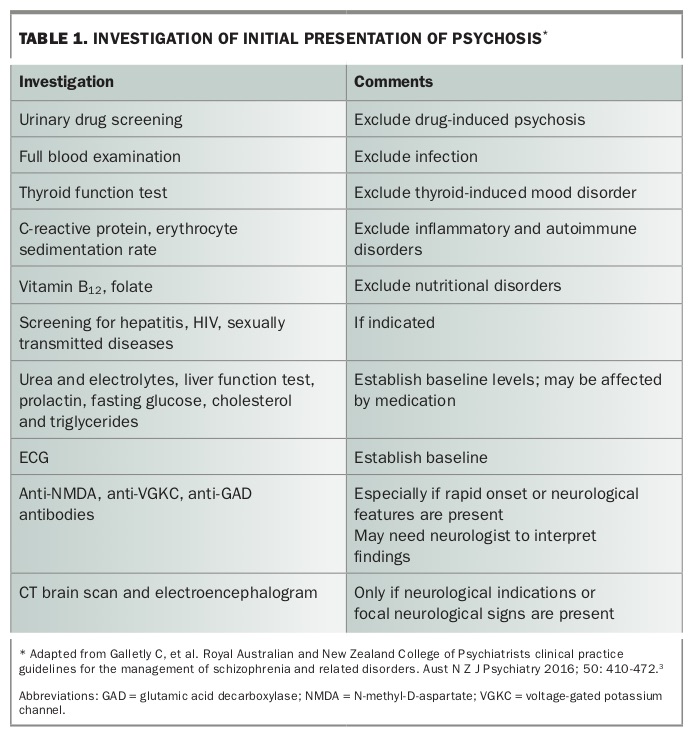
Once psychosis is detected, drug-induced psychosis or the presence of a physical illness (e.g. neurological, endocrine, infective) as the cause must be excluded. Physical causes may emerge through direct or collateral history, but more often investigations are needed (Table 1). A physical examination should be performed if possible.
Treatment
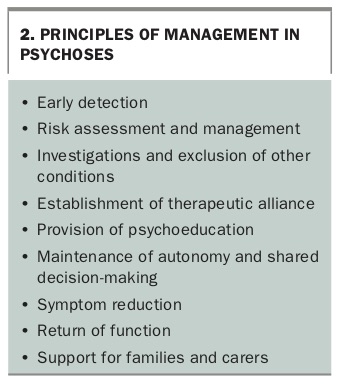
The overarching principles of treatment are outlined in Box 2. Treatment is aimed at ensuring safety, symptom reduction and return of function and quality of life. This should occur within a framework of shared decision-making and respect for autonomy, unless risk escalates unacceptably.
{kind=link}
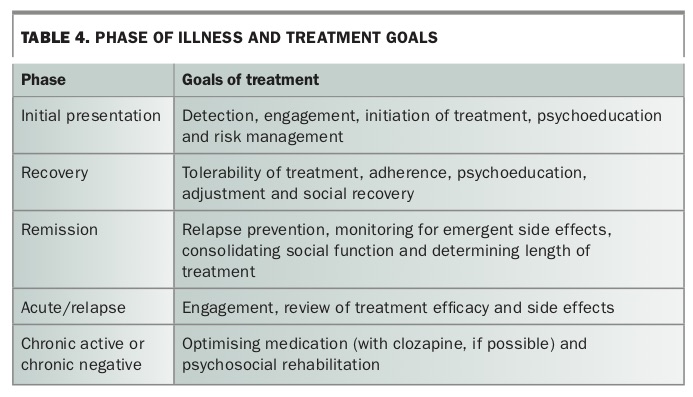
When psychosis is detected, the next step is to identify the patient’s illness phase: initial presentation, acute, recovering, remitted, relapsed, chronically active or chronically negative. This will determine the treatment plan needed by the patient (Table 4).
{kind=link}
In the patient’s initial presentation of psychosis, there is an emphasis on detection, engagement, initiation of treatment and psychoeducation. Initial presentations of psychosis often involve acute symptoms that have a less predictable risk profile and may require inpatient treatment for risk containment. This is followed by a recovery phase, in which the patient may still be experiencing attenuated symptoms, as well as adjusting to medication side effects and the social impact of the illness. For patients who experience complete remission, the emphasis is on maintaining remission, reducing side effects, returning to social function and determining length of treatment. Some patients will develop a chronically psychotic state; for these patients, the emphasis is on providing optimised pharmacological treatment (with clozapine, if possible) and psychosocial rehabilitation.
The types of management options in schizophrenia are also dependent on the symptoms and subsyndromes present, such as prominent anxiety, mood symptoms or negative syndromes. Such syndromes may affect the choice of antipsychotic medication, other medications such as antidepressants, or psychological interventions such as supportive or cognitive behavioural therapy.3
Medication prescribing
All antipsychotic medications block dopamine D2 receptors in the mesolimbic tract of the brain, and dysregulation of brain dopamine mechanisms is probably the common pathological factor in schizophrenia and related psychoses.4 Conventional, or typical, antipsychotic medications cause extrapyramidal side effects when given at doses that are effective for treatment of psychosis through nonselective dopamine blockade.
Second-generation, or atypical, antipsychotic drugs are associated with a substantially lower risk of extrapyramidal side effects (including tardive dyskinesia) when given at clinically effective doses. Most atypical antipsychotics also block serotonin receptors, and the combination of serotonin and dopamine antagonism may be responsible for the lower frequency of movement disorders with these drugs. More recently, partial dopamine agonists, such as aripiprazole and brexpiprazole, have been introduced.11
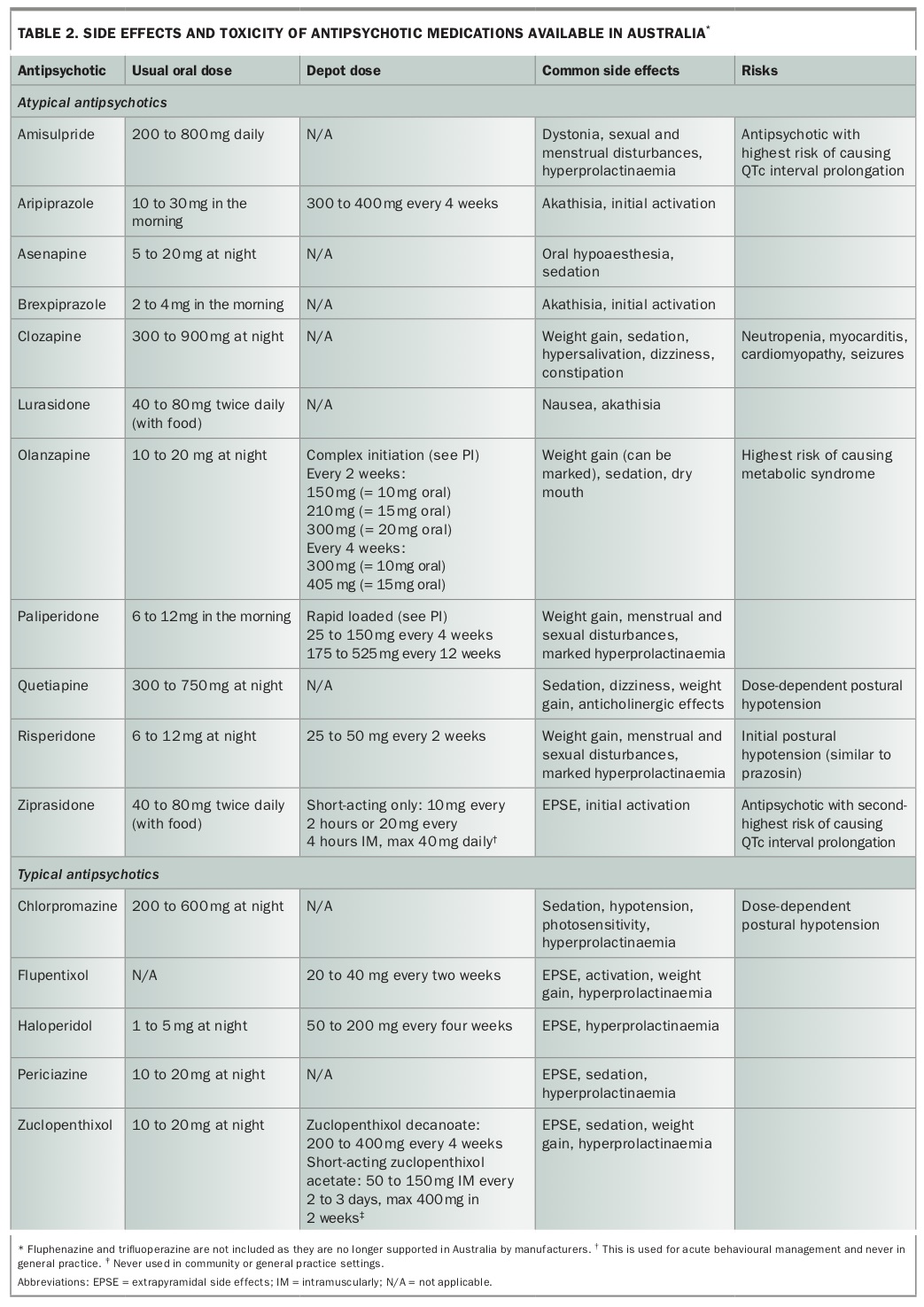
Antipsychotics and their common side effects and risks are listed in Table 2. All antipsychotic medications can cause neuroleptic malignant syndrome, lowering of seizure threshold and cardiac arrhythmias.
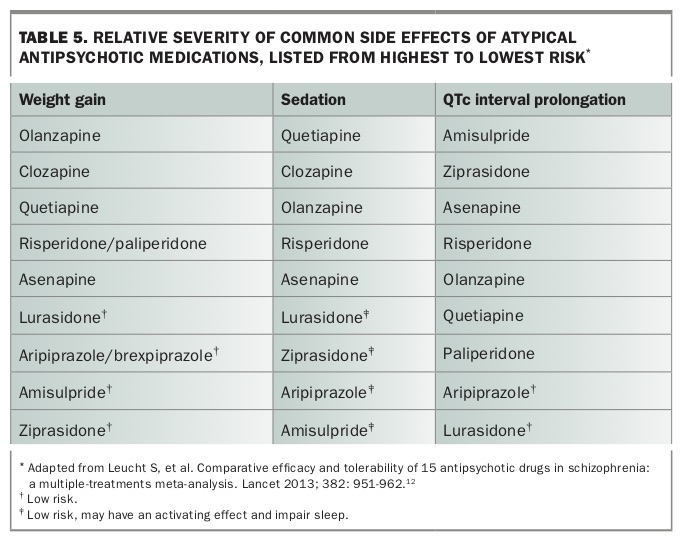
Medication choices are best based on side-effect profile, acceptability of side effects to the patient and likelihood of efficacy. Patient education regarding the comparative severity of side effects is important in making informed choices about medication. The comparative severity of several common side effects (weight gain, sedation and QTc interval prolongation) of the atypical antipsychotic medications is shown in Table 5.12
{kind=link}
Although there are risks associated with antipsychotic medications, epidemiological studies uniformly show that absence of antipsychotic treatment is associated with the highest mortality, and mortality is reduced with the use of effective antipsychotic medication.6 All causes of premature death, including suicide and cardiac disease, are reduced by treatment with antipsychotic medication. Of note, mortality is lowest with use of long-acting injectable treatments and clozapine. Prescribing of high-dose antipsychotic medication is associated with higher mortality.13
Adherence to medication is key in determining the efficacy of treatment and preventing relapse. Absorption of some oral medications, particularly lurasidone and ziprasidone, may be affected by food. Depot antipsychotic treatment is associated with lower rates of relapse than treatment with atypical antipsychotics, even in patients who adhere to oral treatment.14
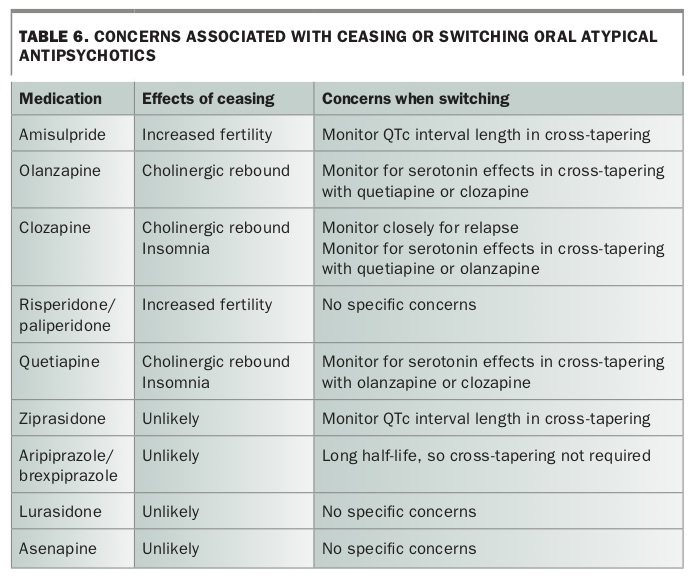
Switching medications is necessary when there has been a lack of efficacy or problematic side effects. Care should be taken to prevent relapse of illness when changing medication (Table 6). Cross-tapering strategies can be helpful in higher-risk situations. Combining antipsychotic medications is generally a specialist practice and requires extra monitoring of QTc interval length and other side effects.
{kind=link}
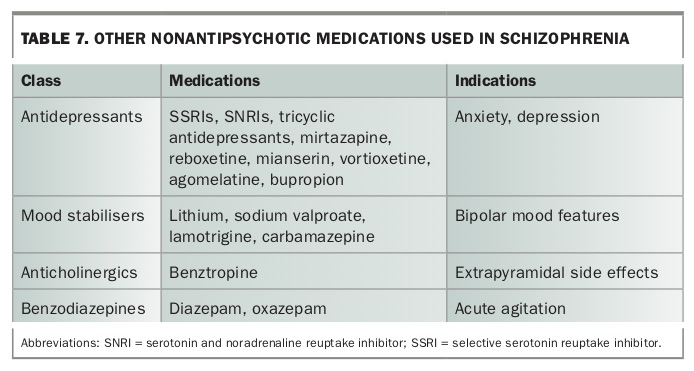
The simultaneous use of more than one psychotropic medication is common in Australia, but it should have a clear rationale and demonstrated efficacy.15 Patients with mood symptoms may benefit from the addition of a mood stabiliser or antidepressant (Table 7). Antidepressant monotherapy should be used with caution, as it may exacerbate psychosis. Care should be taken to avoid pharmacokinetic interactions, such as those of selective serotonin reuptake inhibitors (particularly paroxetine, fluoxetine and fluvoxamine) and anticonvulsants (e.g. carbamazepine).
{kind=link}
Patients with severe negative symptoms are likely to be taking clozapine and may benefit from the addition of low-dose amisulpride or a partial dopamine antagonist, such as aripiprazole.16 Benztropine may be prescribed for Parkinsonian side effects of antipsychotic medication, with caution regarding anticholinergic side effects, such as dry mouth and constipation.
Medication use in pregnancy
Women with schizophrenia who may become pregnant should be aware of the importance of contraception and the risks associated with medication. Women of childbearing age should be warned to avoid becoming pregnant while taking sodium valproate, which is associated with fetal neural tube, cardiac and facial malformation, as well as neurobehavioural effects.17
Antipsychotic medications do not appear to have a clear signal for teratogenicity, when corrected for confounders such as smoking and obesity.18 There is a higher rate of perinatal complications when antipsychotic medication is prescribed, but the benefits of treatment usually outweigh the potential complications.19 Women who become pregnant while taking antipsychotic medication can be referred to the National Registry of Antipsychotic Medication in Pregnancy (www.maprc.org.au/nramp).
Stopping antipsychotic medication
Advice about whether and how to cease medication is a frequent conundrum in clinical practice. For patients with recurrent or chronic psychosis, cessation of medication is likely to result in relapse.20 The situation in those with first-episode psychosis is less clear. For the past 10 years, the advice in the Royal Australian and New Zealand College of Psychiatrists (RANZCP) guidelines has been to continue medication for 12 months.21 However, new data suggest that patients who cease antipsychotic medication after a first episode have a greater than 90% risk of relapse over two to three years.22 It is likely that a recommendation to continue antipsychotic medication for significantly longer will at some point supersede the current RANZCP recommendation for first-episode patients who have fully recovered.
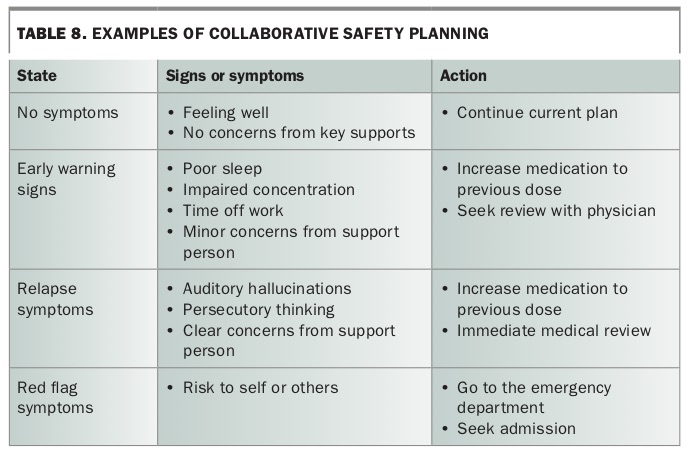
When a decision to cease has been made, care should be taken to slowly wean the medication and to have a relapse safety plan in place (Table 8). Safety planning can reduce risk and uncertainty for patients and their families and can improve transition into care when needed.
{kind=link}
Psychosocial treatment
A major component of schizophrenia treatment is psychosocial.3 GPs can engage in psychosocial treatment through the provision of psychoeducation and referral. Referral to psychology services may assist patients with symptom management and resilience to stress.
Patients or their GPs can refer to nongovernment psychosocial services in many states. Aspects of psychosocial rehabilitation are being funded under the National Disability Insurance Scheme (NDIS) for people aged under 65 years. GPs may be required to provide supporting documentation for NDIS applications.
Recovery model
Reflecting a changing paradigm in both public and private psychiatric services, the ‘recovery model’ is associated with changes in the Mental Health Acts of several states that foster increased autonomy. ‘Recovery’ aims to place the person’s values at the centre of treatment, to reduce stigma and promote hope. It is centred on the idea that recovery is not the presence or absence of symptoms but rather a set of personal and social goals determined by the individual.23 Although occasionally regarded as antipsychiatric, the recovery model is consistent with best-practice comprehensive psychiatric treatment.24
Physical health monitoring
Physical health status and access to physical healthcare services remain poorer for people with psychosis.25 Monitoring of physical health is therefore a major role of Australian GPs in providing care for patients with schizophrenia and related psychoses.
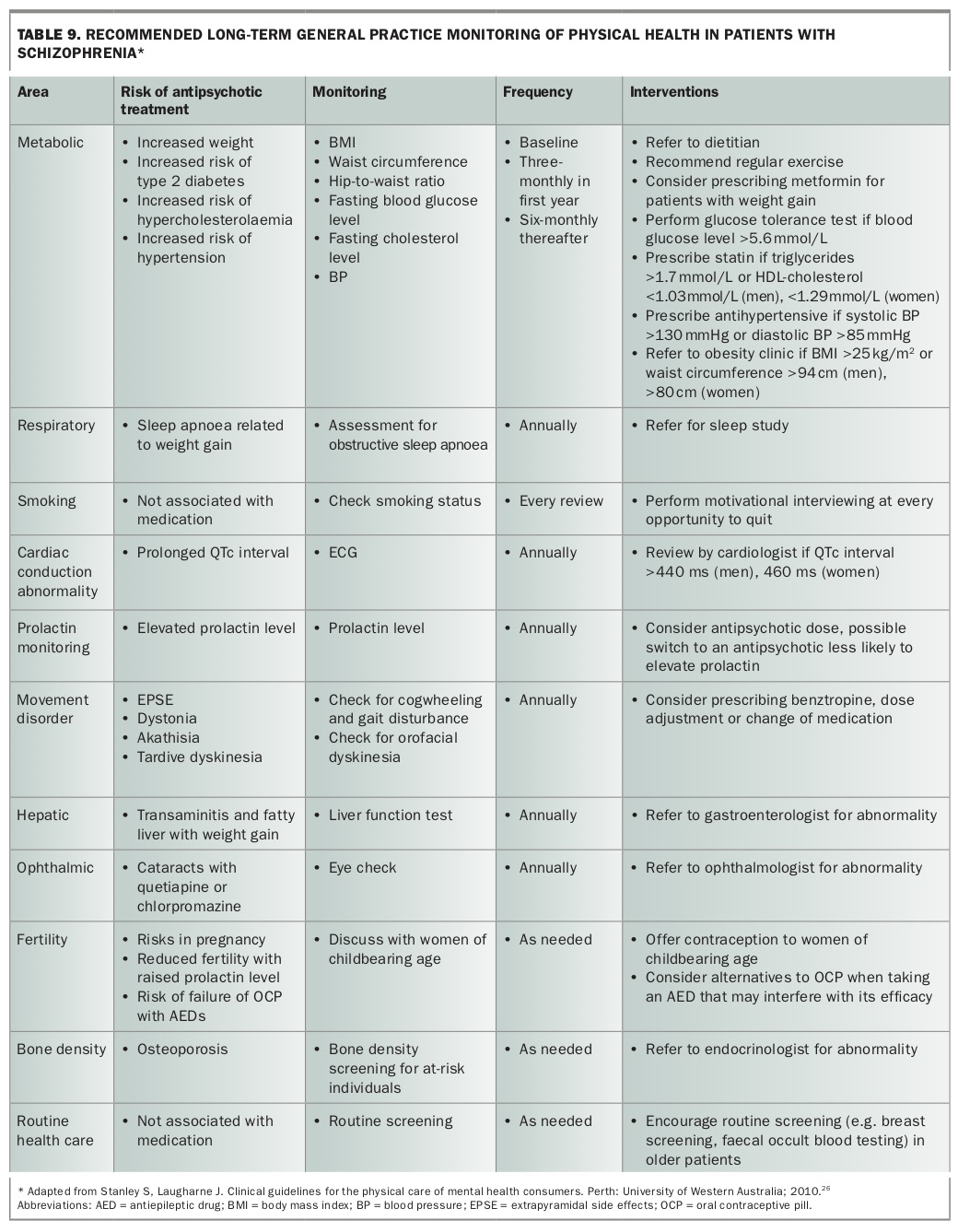
GPs have historically focused on QTc interval monitoring, movement disorders and smoking cessation. Newer challenges have included monitoring and managing metabolic problems, which are more likely to occur with some of the newer antipsychotic agents.26 Antipsychotic medications can elevate prolactin levels, and the consequences of this, such as amenorrhoea, also need to be understood. Recommended monitoring of physical health for patients with schizophrenia is shown in Table 9.26
{kind=link}
Drug and alcohol issues
Misuse of drugs and alcohol is commonly associated with psychoses and substantially worsens outcomes.27 Psychosis is exacerbated by substances that increase dopamine centrally, with amphetamines, meth-amphetamines and high-concentration tetrahydrocannabinol cannabis the most frequent examples. Synthetic cannabis can be particularly problematic and undetectable on urinary drug screening.
Misuse of anticholinergic drugs can occur, as this may induce euphoria, whereas misuse of other substances, including alcohol, may reflect self-medication of psychotic symptoms or psychosocial distress associated with schizophrenia. Recognition of comorbidity and motivational interviewing remain the keys to reducing substance misuse in the general practice setting.28 Effective treatment of psychosis (particularly with clozapine) also reduces substance misuse. Structured treatment programs, if available and acceptable to the patient, are helpful.
Smoking is highly comorbid with psychiatric disorder generally, and up to two-thirds of people with psychosis are current smokers.25 In those who are able to quit smoking, the blood concentration of some medications (e.g. clozapine, olanzapine) may be increased suddenly, causing increased side effects and toxicity.
Diversion of medication for street sale may occur with psychotropic drugs. Quetiapine is known to have a prison and street value.29,30
Referral to other services
Where possible, assessment by a consultant psychiatrist, who can then assist with the formulation of a longer-term management plan, should be undertaken. Patients with schizophrenia and related psychoses who are primarily managed in general practice should have periodic reviews with a consultant psychiatrist. Such initial consultations and reviews are facilitated through the Medicare item 291 scheme.
Some general practice clinics have access to a mental health nurse. In urban and relatively affluent areas, it is easier to access private psychiatry referral and advice, especially regarding medication, whereas telepsychiatry has made access to specialist private psychiatry services more available to rural and remote populations.3 Psychological intervention may be accessed privately; up to 10 sessions can be subsidised through Medicare in the Better Access scheme.
Many patients will derive benefit from dietitian and dental services. Exercise programs are also valuable in optimising physical health. Psychosocial support services, as well as occupational therapy options, can be accessed directly or through NDIS applications. Ideally, for patients with severe and unremitting psychotic illness, comprehensive treatment for schizophrenia is best delivered with input from a multidisciplinary team.
Referral to specialist public or private psychiatric services should always be made when significant risk is emergent, including risk related to psychosocial or functional decline in younger people. Referral should also be considered when the diagnosis is unclear, when the patient does not have competence to consent and is refusing treatment, and when treatment is ineffective or intolerable.
Families and carers
GPs are a crucial source of support for the families and carers of people with schizophrenia, in providing information and psychoeducation for families and psychological and physical health support for carers. Information about other support services, including peer support, can be accessed on the internet, such as through SANE Australia.31
Conclusion
GPs continue to play a major role in the management of schizophrenia, from initial presentation through to long-term remitted and chronic presentations. Effective management is enhanced by an understanding of the nature of the disorder, as well as treatment principles and practices. A good grasp of medication options and physical health management makes the GP an invaluable resource for patients and their families. MT