Assessing patients with seizures
Key questions in diagnostic evaluation of patients presenting with a seizure include is it an epileptic seizure or a nonepileptic mimic and, if epileptic, what are its features? Few investigations provide conclusive diagnostic results, and assessment is largely clinical. The cause of the seizure and likelihood of recurrence are important considerations when deciding on management.
- Many patients who present for the first time with a tonic-clonic seizure have had previous nonconvulsive seizures and have epilepsy.
- The diagnosis of epileptic seizure should never be assumed without a supporting history because several nonepileptic disorders, including syncope, paroxysmal movement disorders and psychogenic nonepileptic seizures, can mimic epileptic seizures.
- Electroencephalography is an important diagnostic test for patients presenting with seizures; the presence of interictal epileptiform discharges strongly supports a diagnosis of epileptic seizures, although normal results do not exclude a diagnosis of epilepsy.
- CT is useful only in the acute setting when looking for structural lesions such as a stroke, abscess, haematoma or tumour.
- Focal seizures and evidence of neurological dysfunction are predictive of seizure recurrence.
Seizures are common, with 23 to 61 per 100,000 people annually experiencing a single unprovoked seizure.1 A further 29 to 39 per 100,000 people annually experience an acute symptomatic (provoked) seizure, and 6 per 1000 develop epilepsy (recurrent unprovoked epileptic seizures) during their lifetime.1 GPs will see patients presenting after their first-ever epileptic or nonepileptic seizure, as well as patients with epilepsy presenting with breakthrough seizures. This article discusses the key issues that should be addressed in the diagnostic evaluation and treatment of these patients.
Is it an epileptic seizure?
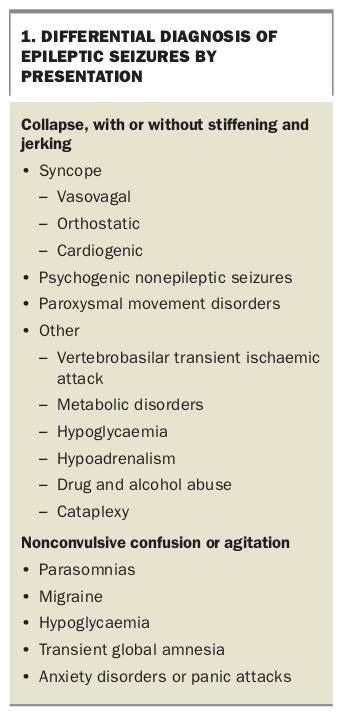
In a patient presenting with a seizure, it is important to consider episodic nonepileptic syndromes in the differential diagnosis. Mimics of epilepsy to consider can be divided into two categories, characterised either by unresponsiveness, collapse, stiffening and jerking movements or by a lack of pronounced motor activity (Box 1).2
{kind=link}
Syncope
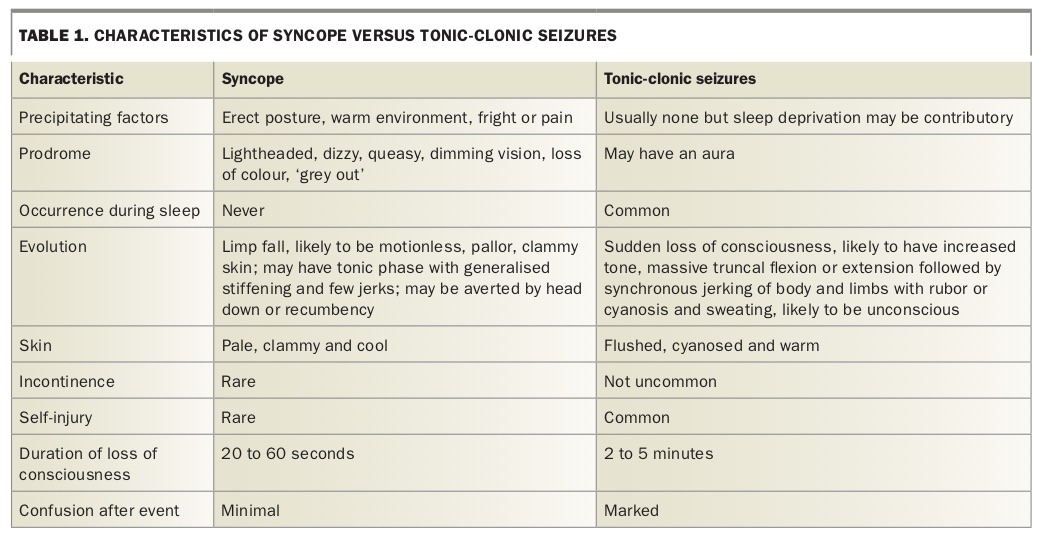
Syncope is often misdiagnosed as an epileptic seizure. Characteristics of the two conditions are compared in Table 1. With syncope, the patient is almost always erect (sitting or standing) and may recall a sense of nausea, sweating, light-headedness or dizziness, followed by visual impairment, distorted hearing and loss of muscle tone immediately preceding collapse. Stiffening, jerking of the limbs and even brief tonic-clonic movements are observed in up to 90% of syncope cases.3 Loss of consciousness is brief, lasting seconds rather than minutes, and postictal confusion is absent or brief. Patients can usually recall regaining consciousness where they collapsed and being attended to by witnesses to the event. In contrast, after recovery from a tonic-clonic seizure the patient next recalls the ambulance officers or the emergency department staff, and there can be a history of marked confusion or even aggression.
{kind=link}
Syncope in association with postural change suggests orthostatic syncope. Knowledge of the patient’s blood pressure on lying and standing may be helpful if orthostatic syncope is suspected, and a tilt table test may be required to support the diagnosis. Cardiac arrhythmia may also present as syncope, and all patients with unexplained collapse should undergo an ECG.4
Other differential diagnoses
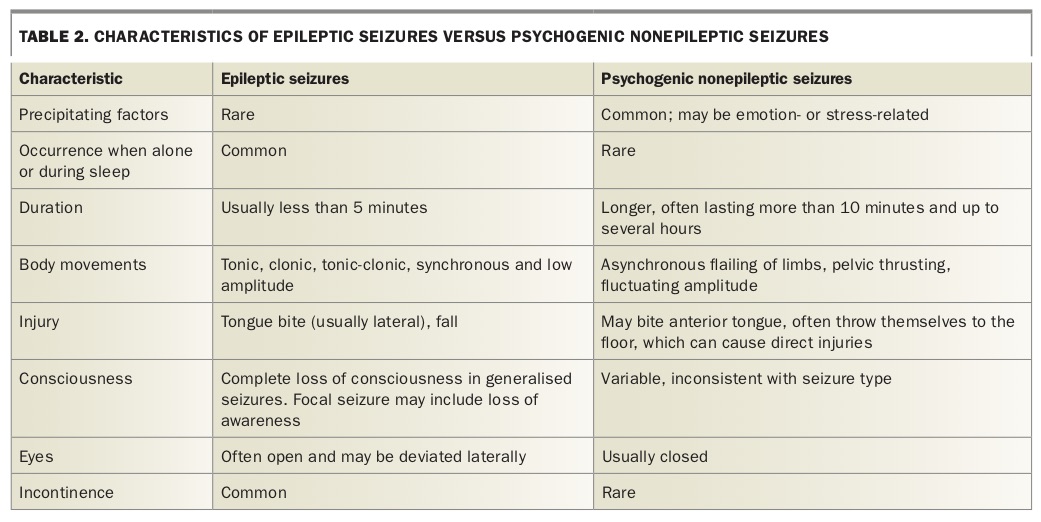
Psychogenic nonepileptic seizures are episodic behavioural events with sensory, motor or consciousness phenomena that resemble epileptic seizures (Table 2). They have a psychological basis and can be explained as an episodic dissociation in the setting of subconscious stress that is often cumulative and can be current or due to past events, even from the distant past.
{kind=link}
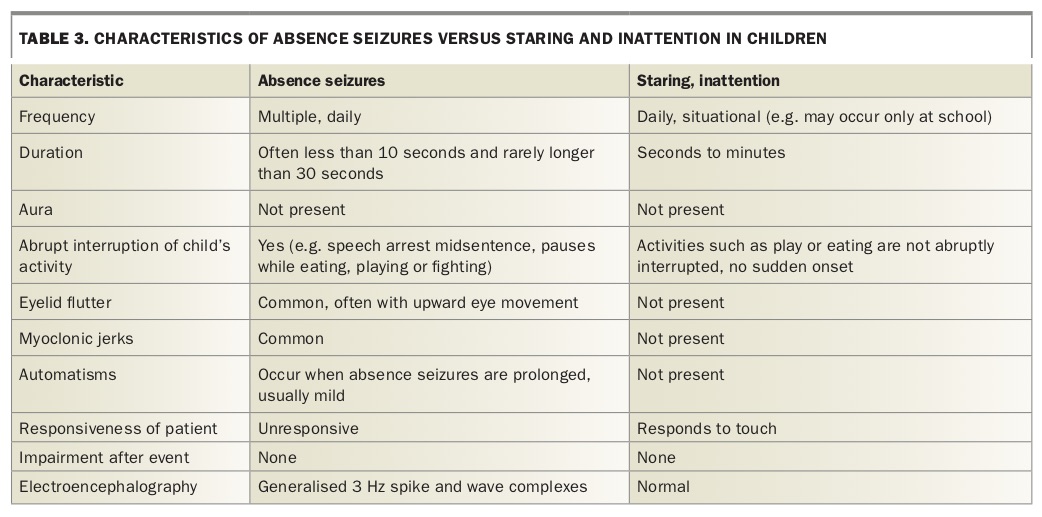
Events confined to sleep are more likely to be parasomnias than seizures, especially when they occur in children. Paroxysmal movement disorders can resemble seizures, but patients do not become confused or lose awareness. Children with episodic unresponsiveness may be experiencing focal seizures with altered awareness (previously termed complex partial seizures), absence seizures or nonepileptic daydreaming. The characteristics of absence seizures versus staring and inattention (differential diagnoses of episodic unresponsiveness in children without convulsions) are shown in Table 3.
{kind=link}
Is it the first seizure?
Up to 74% of patients with newly identified unprovoked seizures have experienced previous seizures.5 Absence seizures, focal seizures with retained awareness (previously termed simple partial seizures or auras) and myoclonic jerks may be ignored for years before medical attention is sought. Patients with seizures with altered awareness may have had many unwitnessed episodes in the past, but these may not be identified until a convulsive event occurs. Unexplained injuries and motor vehicle accidents may also be explained in retrospect by the diagnosis of epilepsy. A patient presenting after a first tonic-clonic seizure with previous focal seizures has a greater than 80% risk of further seizures.
Did the seizure have a focal or generalised onset?
Patients with focal seizures may experience warning symptoms in the form of an ‘aura’. An aura is a focal seizure with retained awareness and indicates a focal onset. Often patients find the symptoms bizarre and difficult to describe. They should be asked:
- whether the episodes are stereotyped (i.e. symptoms are always the same and the patient recognises them immediately as familiar)
- whether the episodes sometimes occur in isolation or always progress in a typical sequence, such as being followed by confusion or focal motor symptoms
- whether the episodes wake them from sleep.
Focal seizures can also present with loss of awareness, which is often reported by witnesses as altered behaviour or responsiveness. Witnesses may observe oral or manual movements, such as chewing or fidgeting (oral and manual automatisms), during this period. Patients with focal seizures of recent onset require detailed investigation with neuroimaging studies (see below, What investigations are required?).
Generalised seizures (absence, myoclonic or tonic-clonic seizures) are not preceded by an aura as bilateral neural networks are immediately involved. A common error is to assume a tonic-clonic seizure has a generalised onset because the patient has no recollection of the start of the event. However, focal seizures with loss of awareness may also progress to tonic-clonic seizures, and postictal amnesia often prevents recall of the start of the event.
Witness accounts of the onset of the seizure are always valuable and should be obtained if possible. Witnesses to a focal seizure may describe the patient having focal motor activity or a sudden behavioural change followed by automatisms accompanied by restlessness preceding the development of a tonic-clonic seizure. Postictal hemiparesis (Todd’s paresis) occurs contralateral to the hemisphere of focal onset.
Were there any precipitants?
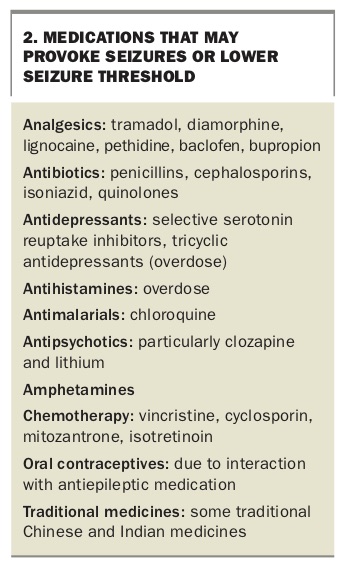
Seizures may be provoked by recreational drugs, alcohol, sleep deprivation, metabolic derangement, acute brain insults and some prescribed medications (Box 2). In young children, febrile illness is the most common cause of acute symptomatic seizures. In patients with epilepsy who present with breakthrough seizures, a history of missed medication doses, medication interactions or intercurrent illness should be sought.
{kind=link}
Is there any underlying neurological dysfunction?
A history of perinatal insults (stroke or hypoxia), developmental delay, central nervous system infections or head trauma suggests possible underlying cerebral pathology. The physical examination should include a search for:
- signs of systemic illness
- skin stigmata that characterise neurocutaneous disorders such as tuberous sclerosis, neurofibromatosis and Sturge-Weber syndrome
- signs of head trauma
- signs suggesting illicit drug use.
A careful neurological examination may also reveal:
- evidence of underlying cerebral pathology, such as limb asymmetry, which possibly suggests an early brain injury or malformation of cortical development
- sensory or motor signs that might support a focal lesion.
Findings suggesting a focal lesion are predictive of seizure recurrence.
What investigations are required?
Laboratory tests
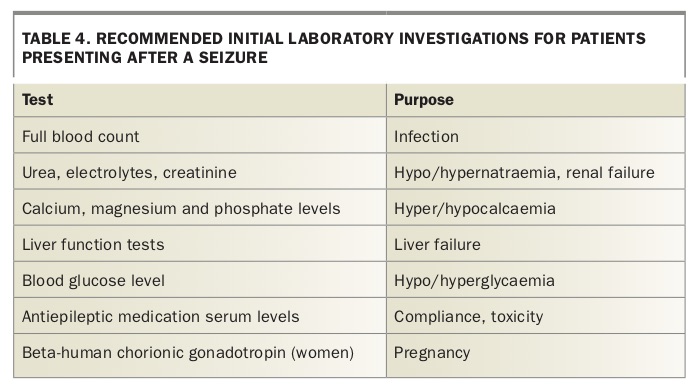
Initial laboratory investigations may identify an underlying cause for the seizures and direct the clinician to undertake more detailed metabolic screening (Table 4). However, routine biochemistry and haematology tests in a patient presenting to the emergency department after a seizure rarely reveal anything of value.6 For patients already being treated for epilepsy, measurement of serum levels of antiepileptic drugs is useful to assess medication compliance and toxicity. Cerebrospinal fluid obtained by lumbar puncture should be assessed if there is any suspicion of meningitis or encephalitis.
{kind=link}
Electroencephalography
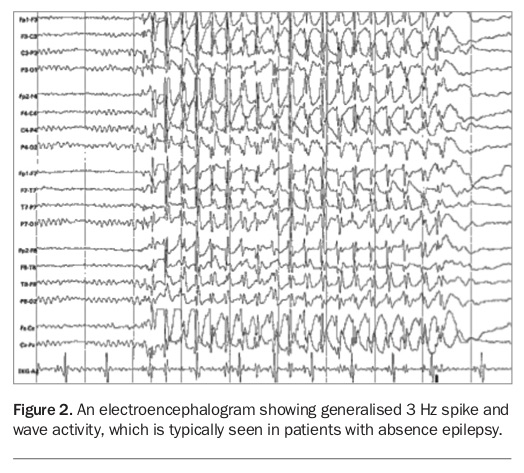
Electroencephalography (EEG) is an important diagnostic test for patients presenting with seizures (Figure 1). The presence of interictal epileptiform discharges strongly supports a diagnosis of epileptic rather than nonepileptic seizures and increases the likelihood of seizure recurrence. It also contributes greatly to the diagnosis of specific epileptic syndromes, which can guide medication selection (Figure 2). Focal abnormalities, slowing or spikes on EEG suggest a focal onset for the seizures and direct the search towards underlying structural pathology. Epileptiform discharges on EEG in a patient presenting after a first-ever seizure are strong predictors of seizure recurrence.
{kind=link}
{kind=link}
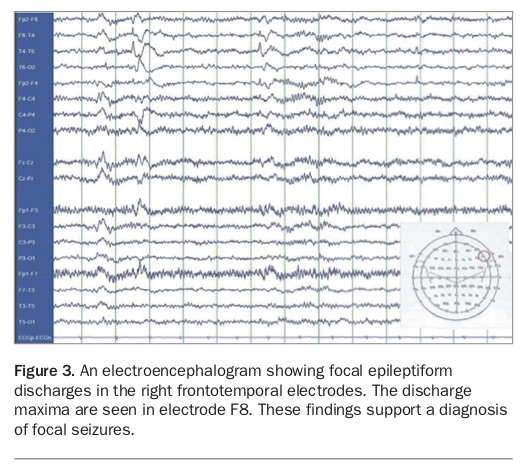
Nevertheless, EEG is not particularly sensitive. Only 30 to 50% of patients who present after an epileptic seizure have epileptiform discharges on EEG (Figure 3). EEG is more sensitive if it is performed within 24 hours of the seizure and after partial sleep deprivation.7,8 If the EEG results are normal but suspicion is high for a diagnosis of epilepsy then EEG should be repeated. A normal EEG result during wakefulness and sleep does not rule out a diagnosis of epileptic seizures.
{kind=link}
Imaging
In the acute setting, CT is helpful only when structural lesions such as a stroke, abscess, haematoma or tumour are sought. An urgent CT scan is imperative for patients who:
- are still confused or unconscious after 30 to 60 minutes
- have a history of recent head trauma
- have an abnormality on postictal neurological examination
- present with status epilepticus.
A CT scan is not an adequate investigation for a patient presenting with focal seizures. In this situation, the structural neuroimaging of choice is volumetric MRI, as it provides the best definition of normal and abnormal structures in the brain. It also enables identification of more subtle pathologies that underlie focal seizures, such as malformations of cortical development and mesial temporal sclerosis. All patients with new-onset focal seizures should undergo MRI to exclude structural abnormalities.9
What are the chances of seizure recurrence?
Patients presenting with a first seizure have a less than 50% overall risk of a second seizure in the next 12 months. Seizures are most common in the first three months after a first seizure; the risk is substantially reduced after this time.10
The chance of a seizure recurring is more than 60% over the next 10 years if the patient:
- presents with unprovoked focal seizures
- has evidence of underlying neurological dysfunction
- has epileptiform changes on EEG
- has a structural lesion on neuroimaging.
Patients who fit these criteria are regarded as having epilepsy.11 They should consider treatment with antiepileptic medication. Patients who present for the first time with a seizure but have a history of previous nonconvulsive seizures are also regarded as having epilepsy.
Conversely, patients whose seizures seem to result from a stimulus and who do not have underlying cerebral pathology or abnormal EEG or radiological findings have a less than 40% chance of experiencing recurrent seizures if they are able to avoid the provocative stimulus. Age is not an independent risk factor for seizure recurrence, and older patients presenting with a first seizure should be managed in the same manner as younger patients.12
Which patients require referral?
Not all patients require referral to a neurologist after a first seizure. Often there are identifiable provoking factors and many patients never have another seizure. However, all patients with an abnormal EEG or neuroimaging result should be referred to a neurologist, as should patients who experience more than one seizure. Patients in whom there is uncertainty or ongoing concerns may also be referred for assessment. It is most useful if all patients undergo MRI and EEG before specialist review.
What antiepileptic medication should be prescribed?
The choice of antiepileptic medication depends not only on efficacy but also on safety and possible long-term side effects. In women of childbearing age, the possibility of pregnancy should be considered, and fetal teratogenic effects and the use of contraception should be discussed. Sodium valproate should be avoided in women of childbearing age.
Generally, the type of seizure dictates the choice of therapy. Carbamazepine is recommended as the first-line agent for focal epilepsy and sodium valproate for generalised epilepsy, as these medications have similar efficacy to the newer agents.13,14 Alternatives to sodium valproate such as lamotrigine or levetiracetam should be used in women of childbearing age. Patients of Asian background have a higher risk of severe cutaneous adverse reactions with the use of carbamazepine. Screening for the human leucocyte antigen (HLA) B*15:02 allele is mandatory in patients from Southeast Asia before carbamazepine is prescribed. An alternative to carbamazepine is sodium valproate (with the above proviso about use in women of childbearing age), as it is effective against focal seizures as well as generalised seizures.
Ethosuximide is an appropriate treatment for patients with absence seizures but does not control focal unaware or tonic-clonic seizures.15
Lamotrigine, levetiracetam, topiramate, lacosamide, oxcarbazepine, vigabatrin and perampanel should be considered as add-on therapies and can be used prior to specialist review. These newer antiepileptic medications have not been shown to be more effective than the older agents. However, they can be better tolerated and have fewer drug-drug interactions. This is relevant in older patients with comorbidities and those using multiple medications.
Phenytoin (oral or injection) is still an excellent choice for patients with focal and generalised seizures in an acute setting. Levetiracetam, sodium valproate and lacosamide are available as intravenous preparations.
Benzodiazepines may be used as add-on therapy but are preferably kept as ‘rescue’ medications for prolonged seizure or clusters of seizures.
For patients unable to swallow tablets, liquid preparations are available for carbamazepine, sodium valproate, levetiracetam, ethosuximide, oxcarbazepine, vigabatrin, phenytoin and clonazepam.
What precautions should patients take?
Recommended safety precautions for patients with seizures should be sensible and relevant to the individual. Patients should be advised to avoid high-risk activities such as extreme sports, surfing, unsupervised swimming or bathing, and climbing to heights greater than their own for at least three to six months after an unprovoked seizure. The duration of these advised precautions depends on the likelihood of seizure recurrence and on the treatment strategy.
A patient who presents with their first seizure is prohibited from driving a private vehicle for six months (providing they do not have any further seizures) under the guidelines of state and territory driver licensing authorities. Patients diagnosed with epilepsy at presentation and started on medication must be seizure free for six months before returning to driving. The driving restrictions for a commercial vehicle are much stricter and specialist referral may be appropriate. In patients with epilepsy and a history of previously uncontrolled seizures, a seizure-free period of one to two years is required for a private vehicle, depending on local regulations. More details are available in the Austroads guidelines on Assessing Fitness to Drive.16
Useful resources for patients
The effect of an epileptic seizure on patients and their families can be profound. The more that individuals understand about their seizures and epilepsy, the less frightening the future will be. Helpful information can be obtained from the following educational resources:
- Epilepsy Action Australia: www.epilepsy.org.au (telephone 1300 374 537)
- Epilepsy Australia: www.epilepsyaustralia.net (telephone 1300 852 853)
- Austroads guidelines Assessing Fitness to Drive: https://austroads.com.au/drivers-and-vehicles/assessing-fitness-to-drive
Conclusion
The diagnosis of an epileptic seizure should never be assumed without a supporting history as nonepileptic disorders are common and great mimics. A witness history is the most important complement to the patient’s own history. Few investigations provide conclusive diagnostic results, and the assessment is largely clinical. It is important to try to determine the cause of the seizure and the likelihood of a recurrence when deciding on management and the need to commence antiepileptic medication. Many patients presenting for the first time after a seizure have had previous nonconvulsive seizures and have epilepsy. Seizure type and evidence of neurological dysfunction are strong predictors of seizure recurrence. MT