Plantar fasciitis: management in general practice

Plantar fasciitis is a common condition, occurring in both active and sedentary people. In most cases it is self-limiting. Management includes stretching and strengthening exercises. In chronic cases, the addition of proper fitting footwear and orthotics, activity modification and a graded exercise program are essential to recovery.
Case scenario
Simone is a 52-year-old woman who enjoys taking long hikes in the Australian bush and walking trips overseas. For the past year she has suffered from plantar fasciitis, and this has greatly restricted her walking. Wearing insoles and performing stretches have provided good relief, but she is missing her long hikes and is pleading for a resolution to her problem. What else can be done for this patient?
Commentary
The plantar fascia is a thick, fibrous aponeurosis that attaches to the inferior calcaneal tubercle and provides support to the medial longitudinal arch of the foot. Plantar fasciitis/fasciosis is common, and particularly affects those in the 45 to 65 years age group. One large study has suggested that two and a half times as many women as men are affected, but other studies have suggested that the prevalence is similar in both sexes.1,2 Plantar fasciitis occurs in both active and sedentary people and is therefore thought to result from chronic overload due to exercise or lifestyle, although the cause is not well understood and is likely to be multifactorial. If recognised early, management is more effective as chronic cases frequently do not respond to usual therapies (e.g. stretching, insoles, physiotherapy), often leading to patients seeking a range of costly and unproven remedies. It is a self-limiting condition in most cases but, as with epicondylitis (tennis elbow), many patients report chronic symptoms lasting years, despite trialling multiple treatments.
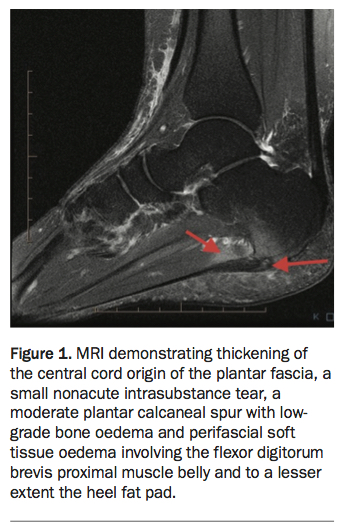
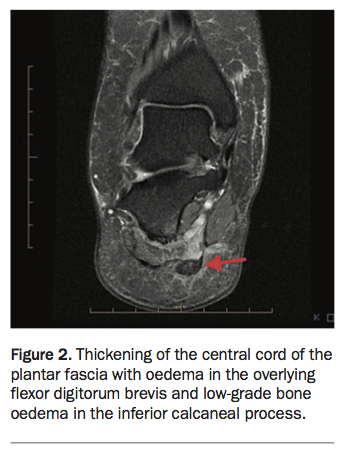
The use of the term ‘plantar fasciitis’ implies an inflammatory condition, but as is the case with epicondylitis, there is considerable evidence that this is a degenerative process – hence the term ‘plantar fasciosis’. However, some patients are clearly more symptomatic and MRI studies often reveal surrounding oedema suggesting an inflammatory process. A tear may or may not be present (Figures 1 and 2).
{kind=link}
{kind=link}
In active people, the onset of symptoms is usually associated with overuse, poorly fitting footwear and an increase or change in training. However, the condition is also commonly seen in sedentary people, in whom poor calf and intrinsic muscle strength, obesity and poor foot mechanics are likely to be contributing factors. Enthesitis associated with a seronegative inflammatory arthropathy, such as ankylosing spondylitis or psoriatic arthritis, can present as plantar fasciitis (but is usually bilateral).
Presentation
The classic history of heel pain as the patient starts to weight-bear in the morning or after a period of rest, with local tenderness to palpation over the insertion of the medial bundle (lateral bundle involvement is less common) of the plantar fascia to the inferior calcaneal process are the key clinical signs. Pain on passive stretching and eccentric or concentric loading (i.e. calf raises) may also be present.
Although the clinical presentation is a classic one in most cases, it is important not to miss other less common causes of chronic heel pain. These include:
- calcaneal stress fracture
- referred pain (e.g. radiculopathy)
- insertional Achilles tendinopathy (which is sometimes mistakenly assumed to be plantar fasciitis by the patient).
Investigation
In most cases investigation is not required. The presence of a plantar calcaneal spur at the enthesis is commonly seen on x-ray, but the patient needs to understand that these spurs are often found in asymptomatic individuals. There may be a role for a high-quality musculoskeletal ultrasound (or possibly an MRI) if there is a genuine need to exclude a stress fracture or other osseous abnormality. When the clinical diagnosis is not in doubt, the primary reason for investigation is to establish if it is a case of plantar fasciosis, or whether there is a tear in the fascia, as this may have some bearing on treatment choice (e.g. cortisone or platelet-rich plasma injection).
Management
The key management strategy in chronic cases, such as Simone’s, is to set the patient’s expectations regarding a return to walking and other weight-bearing activities. Activity modification is essential to recovery. Traditional management has involved rest, the wearing of insoles (possibly with referral to a podiatrist), stretching, physiotherapy, NSAIDs and corticosteroid injection. Corticosteroid injection, although usually effective, can be painful and, as with other chronic enthesopathies and tendinopathies, often only provides short-term relief. Repeated injections are ill advised and may lead to rupture of the plantar fascia bundle.
Other useful conservative treatment options include low-dye taping (which unloads the plantar fascia), night splints and heel cushions. It isn’t difficult to teach patients to tape their medial longitudinal arch to provide support for walking and prolonged weight bearing.
Rather than stretching exercises alone, Simone should also be doing some calf strengthening and intrinsic foot exercises. These can easily be prescribed by demonstrating to her how to perform calf raises (isometric and eccentric) and picking up pencils or curling up a kitchen towel with her toes.
Stretching of the calf muscles and the plantar fascia is important. Traditional remedies have included rolling the bare arch of the foot on a bottle or golf ball – although I would not recommend either option. A firm rubber ball or roller is ideal. Gentle massage and soft tissue releases can help, but in an active patient such as Simone, a lack of strength and endurance in the calf muscles is often neglected as one reason for lack of improvement.
Other treatment options
Other treatment options include extracorporeal shockwave therapy, which can be effective, especially in conjunction with an exercise and activity modification program. This modality is becoming more available and is used by some sports physicians, physiotherapists and podiatrists. However, there are different shockwave machines available and a more powerful and therefore more expensive machine is probably needed in this case. There is no good evidence that ultrasound, laser and other modalities are beneficial.
There has been a commonly held view that in a patient with chronic plantar fasciosis without a tear, a well-placed cortisone injection is indicated followed by one to two weeks of rest. In a patient with a confirmed tear, cortisone injection should be avoided, and the wearing of a walking boot prescribed for two to four weeks. Either option could be considered if the patient does not respond to activity modification, taping, and stretching and strengthening, with the addition of a night splint if appropriate. However, imaging may be required to assess for the presence of a tear before injection and also to identify any features that may benefit from anti-inflammatory measures. There is little to support cortisone injection other than that it can provide short-term relief. Correct placement is important to avoid complication, such as heel pad fat necrosis.
More recently there has been a trend towards platelet-rich plasma injections, particularly in the presence of a tear, and although there is no clear evidence to support this therapy, there are some positive reports in the literature.3 One study found that platelet-rich plasma injections were no more effective than cortisone but advocated the former as being less harmful.4
In chronic cases that have failed all nonoperative treatment there are rare indications for surgery although, in my experience, a significant number of patients who have undergone surgical treatment remain symptomatic. Over the past decade there has been a trend towards surgical release of the proximal medial gastrocnemius rather than or combined with the traditional plantar fasciotomy, especially in patients who have a shortened Achilles tendon, as this unloads the plantar fascia during the stance phase of gait.5
Conclusion
A diagnosis of plantar fasciitis can usually be confirmed clinically without investigation. Simone seems to be getting some relief from wearing insoles, stretching and reduced activity. It is important that she stretches before bed and avoids walking barefoot. She will probably benefit from calf and intrinsic muscle strengthening and then a graded upgrade in exercise with taping for support. Shockwave therapy may help (if it is available). The next option to consider would be a cortisone or platelet-rich plasma injection, depending on whether a tear is present, although in my practice I tend to avoid injections as I find that most patients respond to activity modification, the wearing of correct footwear and insoles/orthotics, and a graded exercise program.
Most cases settle within 12 months but some patients may be affected for years. The more difficult cases are often seen in those who are obese and sedentary with a chronic enthesopathy and tears because activity modification and traditional therapies are often ineffective. However, Simone is likely to respond to good management. MT
Acknowledgement
Thanks to Dr James Linklater, Consultant Radiologist at Castlereagh Imaging for the MRI images.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.