Hearing loss in adults – a common condition associated with cognitive decline
Hearing loss is a common condition that greatly impacts a patient’s communication, mood and quality of life. The relationship between hearing loss and cognition is increasingly defined. New self-administered hearing tests are available for earlier detection of hearing loss. Hearing aids are an effective treatment for mild-to-moderate hearing loss and surgical options may be available for patients with conductive hearing loss.
- Hearing loss is common in the community and increases with age. Mild-to-moderate hearing loss affects one in five adults by the age of 50 years.
- Moderate-to-severe hearing loss has a measurable impact on quality of life, employability and, in the elderly, independent living and cognitive decline.
- Hearing loss is best classified as conductive, sensory neural or mixed. This simple classification guides the clinical evaluation, range of available treatments and response to treatment.
- Online and self-administered tests of hearing are useful for screening.
- History, otoscopy and tuning fork tests allow most causes of hearing loss to be diagnosed, allowing a management plan to be formulated.
Hearing, as one of the five senses, assumes an important role at all stages of life. In early childhood, near-normal hearing in at least one ear is important for speech and language development. In later years, hearing is particularly important in maintaining quality of life, independent living and preventing cognitive decline. A recent global review of the incidence and impact of dementia has highlighted hearing loss in middle life as the dominant modifiable factor to reduce cognitive decline later in life, accounting for 9% of global dementia burden. Current trials are underway to investigate if early treatment of hearing loss in middle life will reduce the burden of dementia later on.1
How common is adult hearing loss?
Hearing loss affects around 17% of the population and is very common in the Australian adult community, with an increasing prevalence with age (17% in 50-year-olds, 48% in 60-year-olds and 64% in 70-year-olds).2 Most of the affected population has a mild-to-moderate degree of hearing loss that is highly suitable for assistance with a hearing aid. In adults, the impact of hearing loss on potential employment, quality of life and general function is equivalent to the disability burden of many health conditions recognised as national health priorities. For example:
- mild hearing loss is comparable with mild asthma
- moderate hearing loss is comparable with severe pain related to degenerative spinal disease
- severe hearing loss is comparable with severe diabetes associated with visual failure.3
Severe hearing loss (greater than 70 dB) affects a smaller proportion of the adult community but carries a greater disability burden. In the elderly, hearing loss is often combined with visual failure and cognitive decline, and can have a profound impact on independent living and quality of life.
Hearing loss and cognitive decline
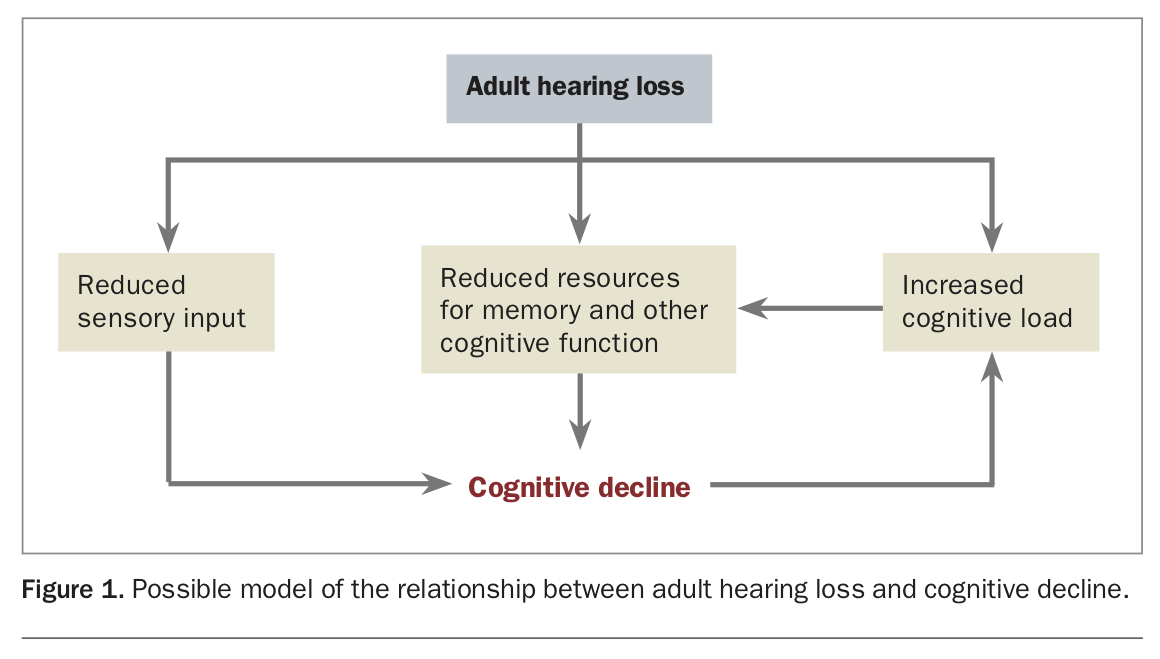
There is increasing recognition of the association between hearing loss and cognitive decline. A longitudinal study of hearing changes over decades and cognition in the same population indicates a very strong correlation and a possible causative association.4 Hearing loss may place an additional load on the mental resources of a vulnerable brain such that the person with hearing loss has to work harder to decode and process sounds. This additional load may mean that there are reduced resources for memory and other cognitive functions, leading to brain changes presenting as dementia (Figure 1). Analysis shows that up to 9% of the global burden of dementia is linked to hearing changes of varying degree (https://www.thelancet.com/infographics/dementia2017).1 What is still being investigated is whether the treatment of hearing loss will halt the progression of, or perhaps reverse, dementia.
{kind=link}
What causes adult hearing loss?
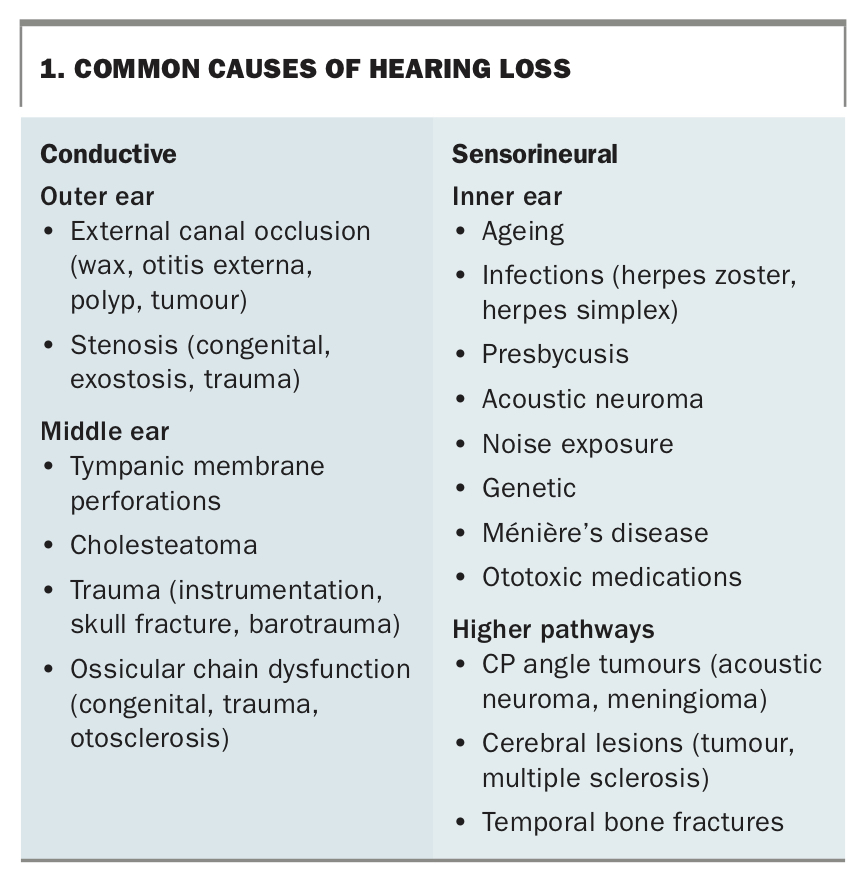
Hearing loss can be classified as conductive or sensory neural, depending on the part of the hearing pathway that is disrupted.5,6 Disruptions to the conductive hearing mechanisms involve the outer and middle ear and produce mild-to-moderate hearing losses, which respond well to treatment with surgery or hearing aids.
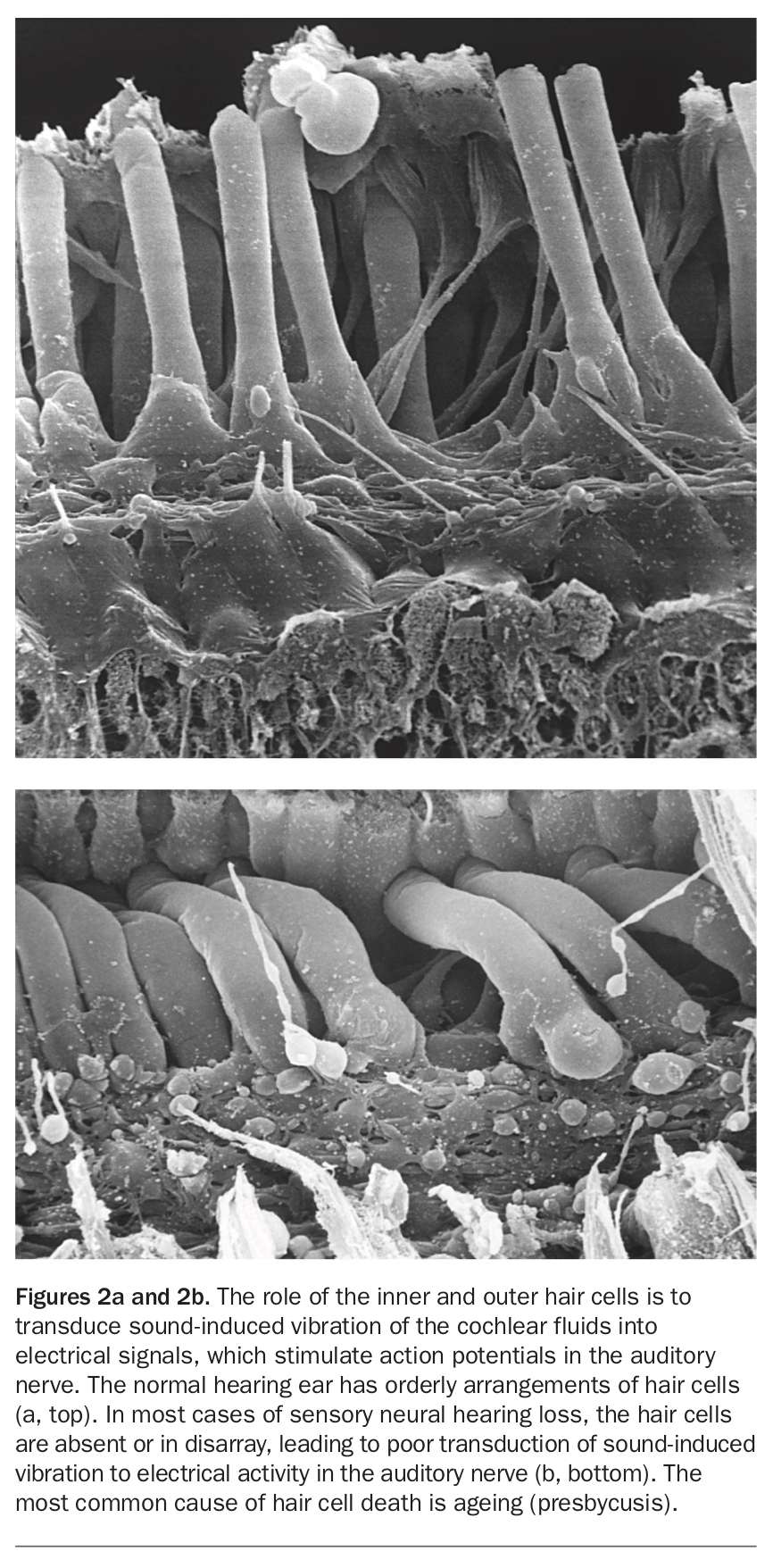
The more common causes of adult hearing loss involve the sensory neural parts of the hearing pathway comprising the inner ear and higher pathways (Box 1) and can result from hair cell lesions within the organ of Corti (Figures 2a and 2b). Often, several contributing factors to hair cell loss and profound hearing loss can be identified; however, sometimes the deafening aetiology is unknown. The hair cells are vulnerable to a variety of toxicities, and in some cases of profound hearing loss a single identifiable causative agent can lead to hair cell damage or loss and subsequent deafness, such as exposure to ototoxic agents (e.g. gentamicin or cisplatin) or following inflammation caused by meningitis.
{kind=link}
{kind=link}
A common pattern of hearing loss in adults is the effect of ageing (presbycusis) added to a pre-existing, nonageing factor of hearing loss, such as noise exposure, with a background genetic susceptibility leading to early hair cell dysfunction. A more detailed discussion of the various conductive and sensorineural causes of hearing loss is discussed in a previous article on hearing loss.7
Assessing hearing loss in the clinic
A simple history and examination of the ear will allow most types of hearing loss to be classified as conductive or sensory neural. The historical time course of the hearing loss and associated otological features such as discharge, bleeding, pain, vertigo, tinnitus or cranial nerve signs, allow the underlying cause of the hearing loss to be determined. Evaluation should be accompanied by the tuning fork test.6
Many causes of conductive hearing loss can be diagnosed with visual inspection of the external ear, canal and drum. An opened ear canal with no element of occluding mass excludes causes of conductive hearing loss such as wax impaction, foreign bodies, tumours, exostosis and stenosis. Visualisation of a healthy intact drum, which is mobile on pneumatic insufflation, also excludes perforations, cholesteatoma, otitis media and middle ear effusions as causes of conductive hearing loss. Otosclerosis due to fixation of the stapes bone is a common cause of progressive conductive hearing loss where the drum appearance and mobility is normal.
In patients with sensory neural hearing loss, the otoscopic examination is generally normal but the tuning fork tests indicate that the hearing changes are due to disruption of the cochlea and higher pathways. Further diagnosis of inner ear hearing losses is dependent on history, results of audiometry and imaging studies.
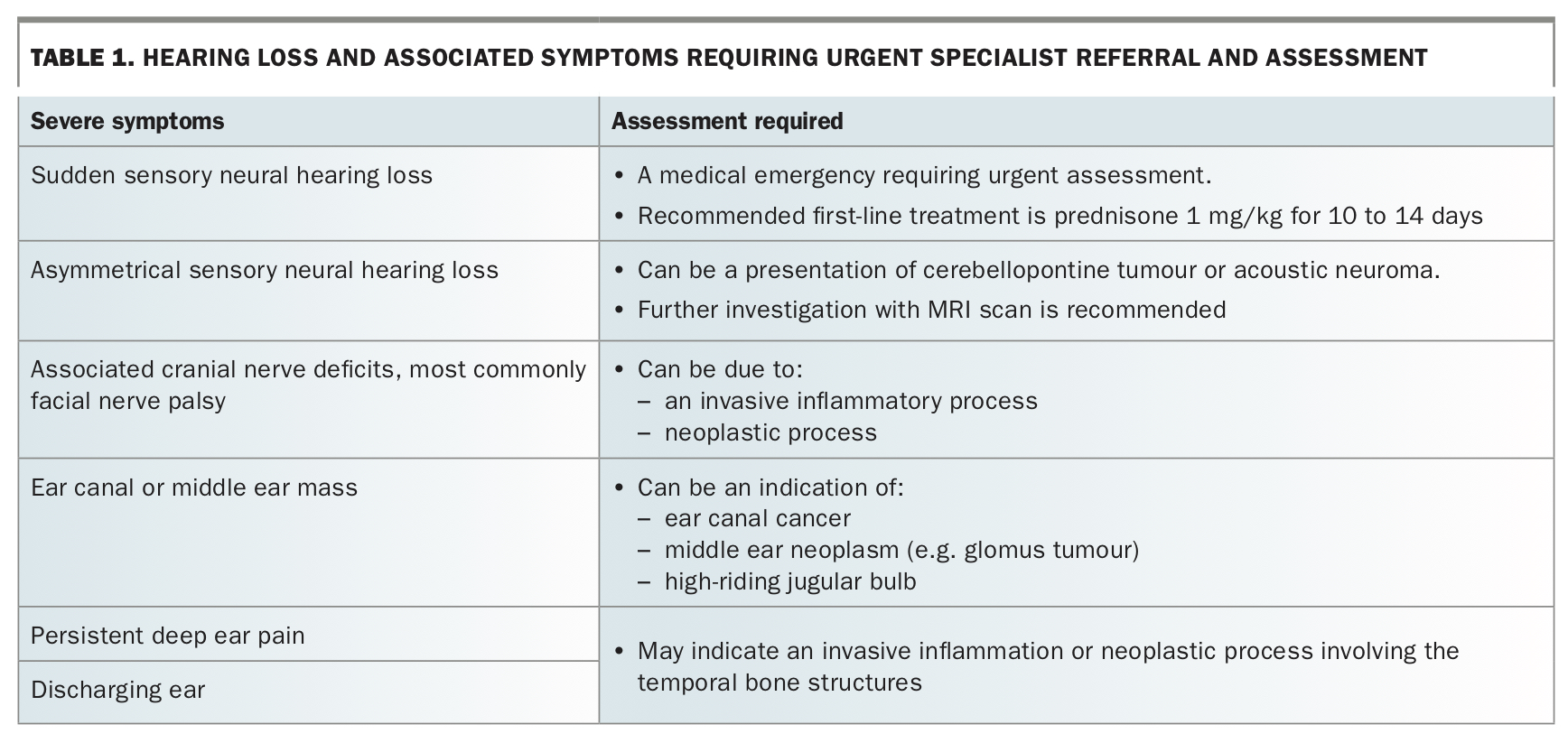
Most cases of adult hearing loss are slowly progressive with no urgency for specialist referral or assessment (Box 2). However, several presentations of hearing loss do require urgent referral (within days to a few weeks) because they may indicate more severe underlying diseases (Box 3). These are listed in Table 1.
{kind=link}
{kind=link}
{kind=link}
Tuning fork tests
The Weber and Rinne tests are most commonly used to assess hearing loss. These simple office tests are performed with a 512 Hz tuning fork by comparing symmetry in hearing between the two ears (Weber test), and the efficiency of hearing through normal hearing middle mechanisms (air conduction) and direct stimulation of the cochlea through the skull bones (bone conduction; Rinne test). The technique in using the tuning fork is important and improves with practice. Particular patterns of patient responses can be detected for conductive hearing losses, sensory neural hearing loss and symmetrical hearing.
Audiometry
A pure-tone audiogram and tympanometry are part of a battery of tests that are performed by audiologists, who are trained in hearing assessment and rehabilitation. These tests allow quantification of various aspects of a patient’s hearing and balance functions including:
- pure-tone thresholds
- speech discrimination
- middle ear function (tympanometry)
- inner ear function (otoacoustic studies).
The audiometer is an electronic device that delivers pure tones to the ear being tested at various frequencies and intensities. Air conduction thresholds are obtained using headphones and bone conduction thresholds are obtained by directly stimulating the cochlea using a vibratory stimulator that is placed on the mastoid. Conductive hearing losses are evidenced by normal bone conduction, but a reduction of air conduction thresholds. The difference between the air and bone conduction thresholds is the degree of conductive hearing loss. In sensory neural hearing loss, loss of cochlear nerve function causes both air and bone conduction thresholds to be reduced.
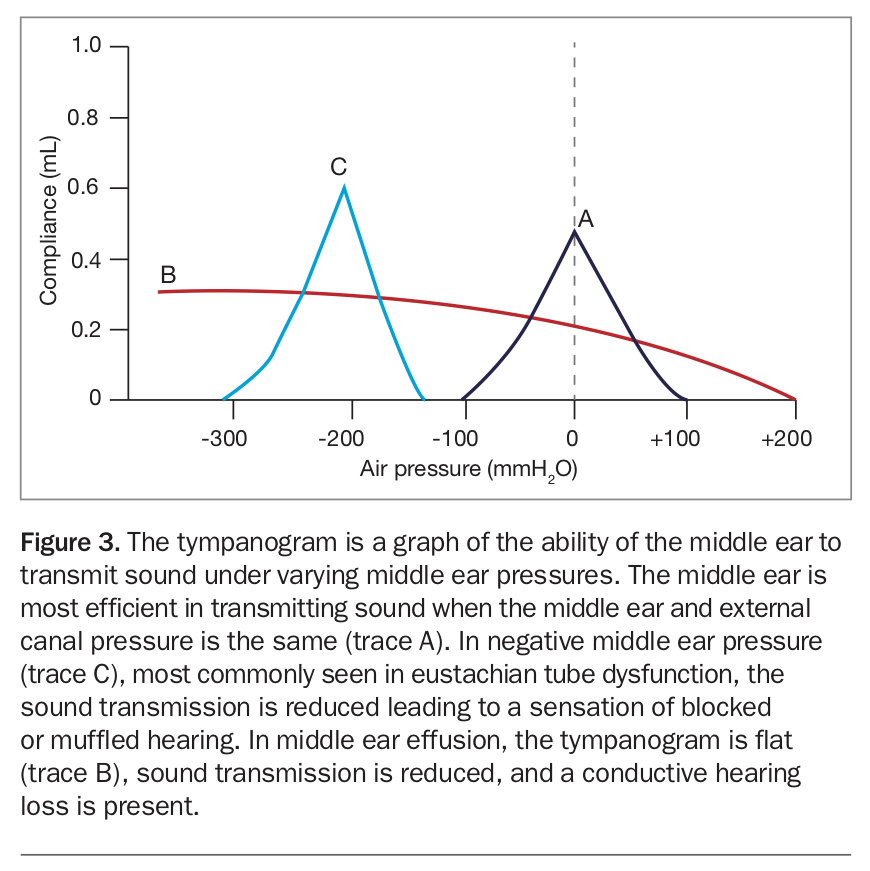
A tympanometer consists of an air-tight ear probe connected to a device that measures changes in middle ear impedance at varying external canal air pressures. The various compliance curves that can be produced suggest different types of middle ear pathology including middle ear effusion, perforations or eustachian tube dysfunction (Figure 3).
{kind=link}
Apps and online screening tests
Recently, several online and app-based screening tests have been developed that allow patients to broadly screen and monitor their hearing ability. The freely available app developed by the World Health Organization, hearWho, is based on recognising spoken digits in background noise (available online at: www.who.int/deafness/hearWHO/en/). It can be administered in any quite environment using a mobile phone and ear buds. The easy to use app clearly display the users’ results and keeps a personalised track record of their hearing status over time. Abnormal screening results can then be followed up by more formal audiometry. The Sound Scouts app is another free self-testing app developed by the National Acoustic Laboratory. It is pictorially based and primarily used for testing children, but can be applied to adults (available online at: www.soundscouts.com/au).
Treatment of hearing loss
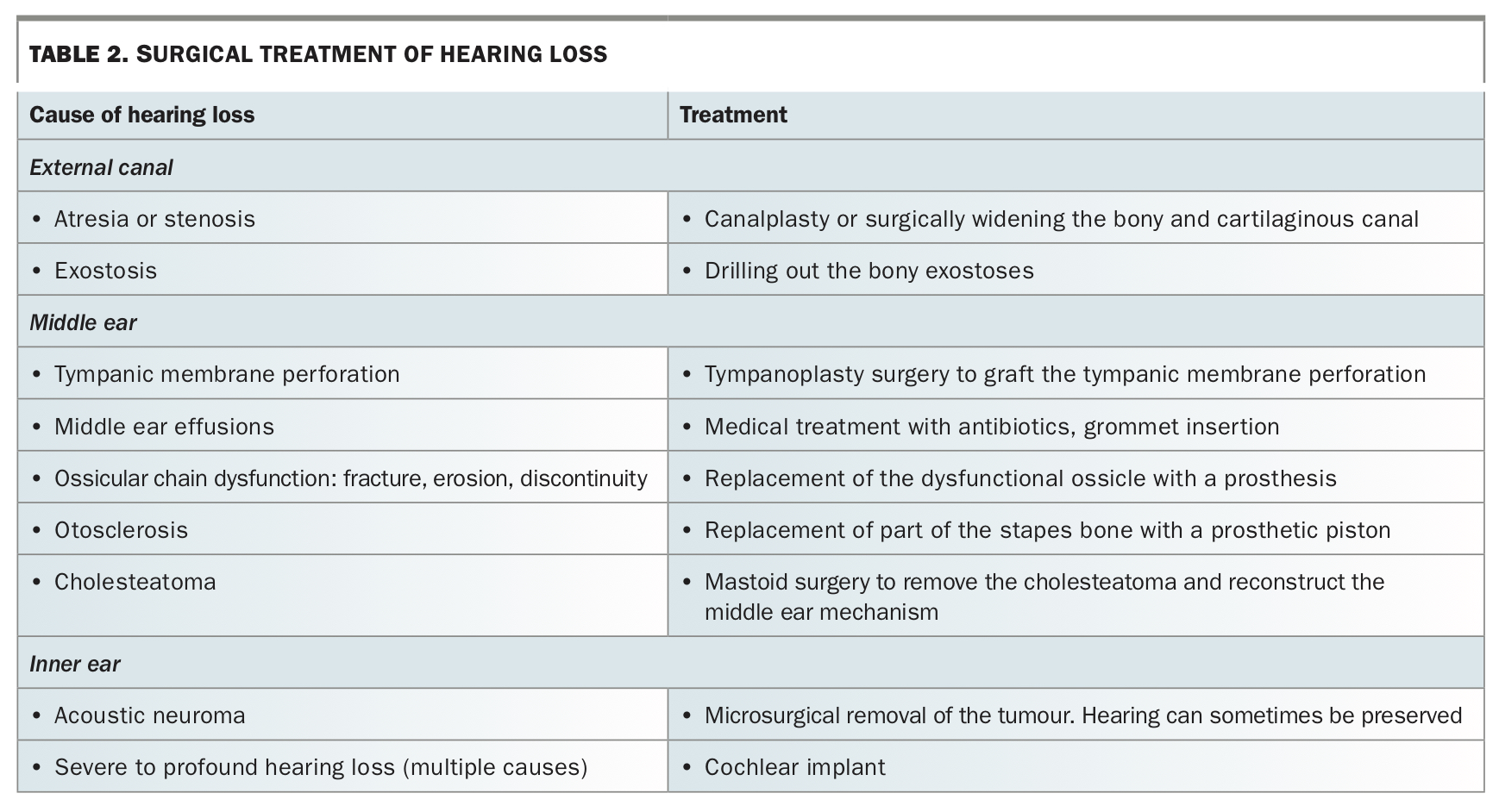
Hearing loss is a symptom that indicates an abnormality of the sound–conducing mechanisms of the outer, middle or inner ear, the auditory nerve and/or higher pathways. Specific treatments for the underlying disease process often produce an improvement in hearing thresholds (Table 2). When the hearing loss is disabling, a specific medical treatment in some cases of infective or inflammatory disease can improve hearing. Many causes of conductive hearing loss respond to surgical treatment. When no specific treatment is available, a carefully fitted hearing aid can minimise the hearing disability.
{kind=link}
Hearing aids
Hearing aids can be effective both in patients with conductive and sensory neural hearing loss. They consist of a microphone, amplifier and speaker. Some models have multiple programmable elements, allowing for listening in varied environments. Hearing aids come in a variety of sizes and designs, but are increasingly becoming smaller and have minimal cosmetic impact on patients. Some types of hearing aids are partially implantable. There are no specific rules in selecting who will benefit from a hearing aid, but the important feature is that the functional characteristics of the aid must match the patient's hearing loss.
A common complaint with hearing aids is that they do not work, particularly in noisy backgrounds, leading to frustration and non-use. This can happen for multiple reasons that are not related to the hearing aid or its cost. One approach to minimising this experience is to trial the hearing aid for several days in different listening environments before incurring significant costs. If in doubt, referral to an ENT surgeon or otologist would be the next step.
Surgery
Modern ear surgery is highly evolved, and there are a range of procedures to improve hearing thresholds in patients with many types of conductive hearing losses. Stapedectomy surgery for patients with otosclerotic hearing loss can produce sustained improvements in hearing often at near normal thresholds. Prosthetic replacements of damaged middle ear ossicles can also significantly improve hearing thresholds. Canalplasty, to correct external canal stenosis, and tympanoplasty, to repair perforations, often improves hearing as well as reducing infection rates.
Cochlear implants or the bionic ear are electronic devices that are implanted within the cochlea allowing direct electrical stimulation of the auditory nerve endings. The surgery for cochlear implantation has become routine, and the outcomes for postlingually deafened adults are greatly improved hearing, often sufficient to provide free communication over the telephone.
Conclusion
The role of the GP is to recognise that hearing loss is common in the community, and that its impact on patients and their families can be significant. The effect of hearing loss on cognition, quality of life and independent living, particularly in the elderly, needs earlier recognition and more purposeful assessment. Initial management consists of determining the nature of the hearing loss using clinical assessment and simple tuning fork tests, arranging audiometry to quantify the hearing loss and imaging to exclude possible conditions requiring treatment. MT
References
11(6): 48-59.
11(6): 117-119.