STIs in adolescents and young adults: prevention and screening

Initiation of intimate sexual behaviours is natural during the course of adolescent development. GPs are well placed to promote sexual health among adolescent and young adult patients, which includes sexually transmissible infection prevention and screening.
First experiences of sexual arousal, emerging interest in sexuality and initiation of intimate sexual behaviours with others are natural and common during the course of adolescent development. GPs are well placed to offer assessment, anticipatory guidance and preventive care advice about a range of health behaviours, which begin during the second decade of life. It is appropriate for GPs to explore adolescent and young adult patients’ interest in, and experiences of, partnered sexual behaviour, within the context of a confidential consultation.
Throughout this article we will use the expression ‘adolescents and young adults’ to refer to those aged 15 to 24 years to reflect sexually transmissible infections (STIs) epidemiology in this age bracket. The median age of first vaginal intercourse in Australia is just under 17 years, and notification rates for notifiable STIs increase exponentially from the age of 15 years, reflecting the commencement of sexual activity.1,2 The WHO defines adolescents as those aged 10 to 19 years, and youth as those aged 10 to 25 years.3
STIs among sexually active adolescents and young adults are relatively common, and usually asymptomatic. In Australia, chlamydia is the only STI with a high enough prevalence to warrant universal, opportunistic screening in sexually active adolescents and young adults. However, some populations of adolescents and young adults are at increased risk of other STIs such as gonorrhoea and syphilis. Offering chlamydia testing should be incorporated into routine clinical practice with sexually active adolescent and young adult patients, while a more detailed sexual history will help direct further STI screening and advice. We will not discuss HIV or blood-borne virus epidemiology or presentations in this article but will include a summary of screening guidelines.
STI epidemiology and clinical presentations in adolescents and young adults in Australia
Chlamydia
Chlamydia is the most commonly diagnosed STI in adolescents and young adults and its prevalence in the Australian population is approximately 5.0% for women under 25 years and 3.9% for men under 29 years.4 Notification rates of chlamydia infection are also highest in the 15- to 29-year age groups.2 Chlamydia trachomatis is a Gram-negative bacterium that can cause cervicitis, urethritis and proctitis. Transmission can occur through all unprotected oral, vaginal and anal sex, as well as non-penetrative genital to genital contact and the sharing of sex toys.
Chlamydia infections are frequently asymptomatic: 50% of men and 75% of women will have no symptoms.5 Symptoms of chlamydia infection include dysuria, urethral discharge, vaginal discharge and vaginal bleeding. Infections can also affect the eye, anus and, less commonly, the pharynx. Women with untreated chlamydia are at increased risk of pelvic inflammatory disease (PID) and this risk increases with recurrent infection. PID may in turn lead to tubal infertility. Although the overall risk of infertility as a result of chlamydia infection is less than 1%, young women who have tested positive for chlamydia have a 70% greater risk of infertility than those who have tested negative.6 Other complications of untreated chlamydia infection include reactive arthritis, increased rates of ectopic pregnancy and chronic pelvic pain and epididymo-orchitis. Chlamydia increases the risk of contracting other STIs through inflammation and mucosal damage.7
Gonorrhoea
Gonorrhoea is much less common than chlamydia. The absolute infection risk for asymptomatic people younger than 29 years old is approximately 0.5%, with higher rates in men who have sex with men and Aboriginal and Torres Strait Island people.8 Incidence rates for gonorrhoea are three times higher for men than for women and six times higher in the Aboriginal and Torres Strait Islander community compared with non-Indigenous people. However, there has been a substantial increase in gonorrhoea notifications among non-Indigenous women in recent years.9 Gonorrhoea is caused by the Gram-negative bacterium Neisseria gonorrhoeae and is transmitted through vaginal, oral and anal sex.
Up to 80% of women and between 10 and 15% of men will be asymptomatic with infection, particularly with pharyngeal and rectal infection.5 Symptomatic infection with gonorrhoea can present with urethral discharge, dysuria, vaginal discharge, dyspareunia, anorectal irritation or conjunctivitis. Complications of gonorrhoea infection include epididymo-orchitis, PID and disseminated disease including macular rash and septic arthritis.
Genital herpes
Genital herpes can cause significant psychosexual morbidity for young people. An initial herpes simplex virus (HSV) episode can result in extensive painful anogenital ulcerations and, although severe complications are uncommon, young people can experience significant distress resulting from perceived social stigma and a lack of knowledge around the ramifications of infection and transmission. Although infection with HSV1 or HSV2 virus can often occur without symptoms, across the Australian population seroprevalence for HSV1 is 76% and for HSV2 12%.10 In adolescents and young adults presenting with genital herpes, health education should be offered with prompt treatment and an offer of follow up review to address concerns.
Genital warts
Genital warts are caused by the human papillomavirus (HPV), usually HPV types 6 and 11, which are among the types targeted by the quadrivalent and nonavalent HPV vaccines. HPV vaccination was incorporated into the National Immunisation Schedule in Australia for girls aged 12 to 13 years in 2007 and boys of the same age in 2013. Five years after the introduction of the girls’ vaccine in 2007, there was a reduction in genital warts presentations to sexual health clinics for Australian born women and heterosexual men under the age of 21 of 93% and 82%, respectively.11 With increasing HPV vaccination rates, the rates of genital warts in adolescents and young adults are likely to continue to decline.
Syphilis
Syphilis is caused by infection with the spirochaete bacterium Treponema pallidum and has been increasing in prevalence among men who have sex with men and remote Aboriginal and Torres Strait Islander communities.9 Syphilis is transmitted through skin to skin contact during unprotected vaginal, oral or anal sex and is highly contagious when an open sore (chancre) is present. Up to 50% of presentations will be asymptomatic.5 In primary syphilis, a patient may present with genital ulcers, which may be painful or painless, and enlarged non-tender inguinal lymph nodes, whereas patients with secondary syphilis may present with fever, malaise, headache, lymphadenopathy and rash. Latent syphilis can occur at any stage after infection when no symptoms are present. Complications of syphilis include neurological, ocular and cardiovascular involvement.
Approach to the STI prevention and screening consultation in adolescents and young adults
One of the key goals of consultations with adolescents and young adults is to engage them in a trusting relationship. Adolescents and many young adults are neither fully dependent on parents and carers for managing their health care nor adults with experience of talking about private issues with healthcare providers or navigating a complex healthcare system. Thus, engaging adolescent and young adult patients can take longer than a standard consultation, but is worth pursuing because of the importance of preventive health care in this age group.12
Best practice in consulting with adolescent and young adult patients involves, in most circumstances, spending some time alone with them. This is best negotiated before or at the very beginning of a consultation. Explaining confidentiality and its boundaries is also an essential part of best practice and all GPs are encouraged to familiarise themselves with these.13
As with any medical procedure or treatment, it is important to seek informed consent when screening for STIs. This is not an onerous process, and includes explaining procedures for treatment, partner notification and re-testing should a test be positive. Patients should be reassured that notification of STIs is confidential and related to public health surveillance.
Medicolegal considerations
Medicolegal concerns sometimes arise when consulting with adolescents under the age of 18 years in relation to consent to medical treatment, and under the age of 16 years (or 17 years in Tasmania and SA) in relation to the age of consent, confidentiality and mandatory reporting. More detail can be found among the list of resources (Box 1).14
{kind=link}
There are some important medicolegal considerations that GPs should be aware of when in consultation with adolescent and young adult patients.13,15 The mature minor principle applies in all Australian jurisdictions in relation to consent to medical treatment. If a GP considers an adolescent under the age of 18 to be a competent minor, then parent or guardian consent is not required for the great majority of medical treatments, including STI testing and treatment. There is no lower age limit.
Disclosure of sexual activity by an adolescent who is under the age of consent to have sex does not require mandatory reporting unless they are considered at risk of significant harm (such as nonconsensual sex, abuse, or concern about a substantial age or power difference between the adolescent and their sexual partner). Adolescent patients need to be reassured that discussions about their sexual activity or sexuality more broadly will be kept confidential unless an exemption applies.
Considerations about privacy of health information are also important. In relation to STI testing and treatment, when an adolescent turns 14 years of age, their parent or guardian can no longer access their Medicare or My Health Record information unless the adolescent explicitly grants this to them. Ask the patient if they are comfortable with STI pathology results being uploaded to My Health Record and if not, indicate this on the pathology request form. Request bulk billing from pathology providers and ensure that bills and results are not posted to the family home, unless previously discussed with the adolescent or young adult. Discuss the adolescent or young adult’s preferred method of communication for notification of results and reminders (e.g. SMS, phone call, email). Ensure that contact information is up-to-date to avoid inadvertently breaching confidentiality.
STI assessment, testing and screening
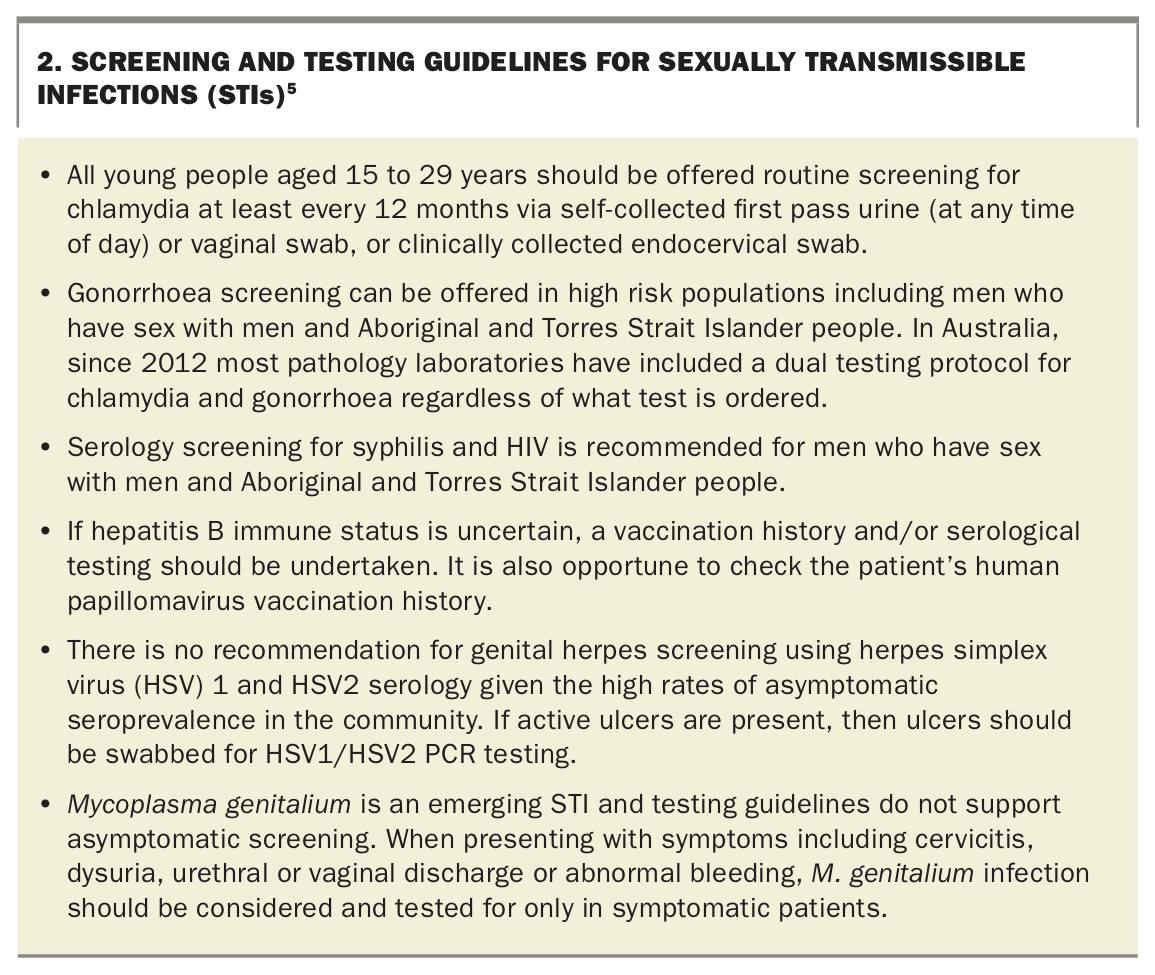
It is important to note the difference between STI testing and screening. If a young person has symptoms where an STI is among the differential diagnoses, then testing must be guided by the clinical picture as described above. Screening refers to the testing of asymptomatic individuals and should be guided by current guidelines (Figure).13 Current STI screening and testing guidelines are outlined in Box 2.5
{kind=link}
Mycoplasma genitalium is an emerging STI; however, testing remains controversial in some situations. GPs should be aware of the following when assessing patients for M. genitalium infection.4,5
- Men. In men, a first void urine specimen appears more sensitive than a urethral swab. A urine specimen for M. genitalium testing should be collected in all men with nongonococcal urethritis.
- Women. In women, a vaginal swab is the most sensitive specimen, but first void urine or cervical swabs can be used. Women who present with cervicitis or PID should be tested for M. genitalium. Testing is generally not recommended for women with vaginal discharge or abnormal bleeding, unless they have concomitant cervicitis or PID.
- Men who have sex with men. Asymptomatic rectal infection is common in men who have sex with men. Studies are conflicting around the association between M. genitalium and proctitis, although cases of proctitis in which M. genitalium is the sole pathogen detected have been reported.
- Asymptomatic people. Sexual contacts of people with M. genitalium, particularly those in a continuing relationship with an infected partner, should be offered testing. Men who have sex with men require urine and anorectal swabs. Throat swabs are unnecessary as pharyngeal infection is rare (1%).5 Screening other asymptomatic individuals for M. genitalium is currently not recommended.
GPs are encouraged to broaden the discussion about STI screening and explore the adolescent or young adult’s sexual and reproductive health.14 This might take place over a few consultations. Young patients can be given general information about contraception and condoms, and invited to discuss sexuality and relationship concerns or issues if or when they wish. Australian secondary students learn about condoms and STI prevention; however, GPs can still use the opportunity in a confidential consultation to explore access to and affordability of condoms, as well as issues and challenges that adolescents and young adults have in negotiating condom use. Although this article focuses on STIs and not HIV, it is pertinent to discuss PrEP with adolescents and young adults who might be at risk of HIV (mostly men who have sex with men). GPs can also direct young patients to appropriate online resources (Box 1).
Conclusion
Adolescents and young adults have the right to sexual health and confidential medical care. STI prevention and screening are an important aspect of primary and preventive health care in this population. GPs who engage young patients in a trusting relationship can have a positive impact on an adolescent and young adult’s sexual health. Key practice points to approaching STI screening and testing in adolescents and adults are summarised in Box 3. MT
{kind=link}